


INTRODUCTION
Immune recovery after allogeneic hematopoietic stem cell transplantation (HSCT) depends on several variables during the transplantation including the specific conditioning regimens, types of donor, source of hematopoietic progenitor cells, and approaches to prevent graft-versus-host disease (GVHD) [1]. For example, T-cell depletion is used to decrease the frequency of GVHD. T-cell depletion of the allograft leads to significantly delayed immune reconstitution and increases morbidity and mortality due to infection in both younger and older recipients [1,2]. In patients with GVHD, immune reconstitution and response to vaccines is further hindered by the use of systemic corticosteroids and other immunosuppressive drugs to treat chronic GVHD [3]. In addition, thymus is extremely sensitive to immunosuppressive treatments for GVHD prophylaxis, and GVHD itself [4].
Reconstitution of the immune system following allogeneic HSCT is a complex process that requires successful engraftment of hematopoietic stem cells, as well as adequate thymic function. Recovery of innate and adaptive immune systems occurs gradually during the post-transplantation period. Innate immunity usually recovers during the initial several months, whereas reconstitution of adaptive immunity occurs over the first 1 to 2 years. Delay in immune system recovery is associated with morbidity and mortality [5].
For patients who undergo stem cell transplantation, day 100 following the procedure is an important milestone. The risk of transplant-related complications and infections is the highest during the first 100 days post-transplantation. Immune recovery after allogeneic HSCT is characterized by cellular immune deficiencies involving a reduced number of cytotoxic lymphocytes, natural killer (NK) cells in the innate immune system, and T-cells in the specific immune system [5].
In this study, we assessed the clinical factors including the GVHD prophylactic regimens that affect the immune recovery status at 100 days after allogeneic HSCT in patients who receive fludarabine-based conditioning. In addition, the effect of immune reconstitution on clinical outcomes including the overall survival, disease-free survival, non-relapse mortality, and relapse rate was evaluated.
METHODS
Ethical statement
This study was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital (2015-07-029) with written informed consents.
Patients
One hundred fourteen patients were included in this retrospective analysis. The patients received allogeneic HSCT at Soonchunhyang University Bucheon Hospital from August 2004 to April 2016. The diagnoses included acute myelogenous leukemia (AML), acute lymphoblastic leukemia (ALL), myelodysplastic syndrome (MDS), lymphoma, multiple myeloma, chronic myelogenous leukemia (CML), and aplastic anemia. The pre-transplantation status of acute leukemia patients varied and included first complete remission (CR1), second complete remission (CR2), third complete remission (CR3), and refractory status. To calculate hematopoietic cell transplantation-comorbidity index (HCT-CI), baseline studies were conducted that included echocardiography and pulmonary function tests. Based on the risk stratification using HCT-CI scores [6], patients were categorized into two risk groups. The standard-risk group showed low or intermediate risk, and the high-risk group had high risk. Several conditioning regimens with various dose intensities were administered according to disease type, disease status at the time of transplant, and HCT-CI scores. The myeloablative conditioning regimens included busulfan (12.8 mg/kg)/fludarabine (150 to 160 mg/m2) with or without antithymocyte globulin. The reduced intensity conditioning regimen included busulfan (6.4 to 9.6 mg/kg)/fludarabine (150 to 180 mg/m2) with or without antithymocyte globulin (thymoglobulin, 5 to 9 mg/kg in 3 days) or alemtuzumab (30 mg/day for 2 days). The combination of fludarabine (150 mg/m2)/cyclophosphamide (120 mg/kg)/antithymocyte globulin was used as a conditioning regimen for patients with aplastic anemia. Patients received peripheral blood stem cells from matched sibling donors, matched unrelated donors, or haplo-identical related donors. Patients received calcineurin inhibitor-based GVHD prophylaxis (cyclosporine-A or tacrolimus).
Evaluation of the immune status post-transplantation
For the identification and enumeration of different subpopulations of peripheral blood lymphocytes, immunophenotypic analysis using flow cytometry was performed at 100 days after the transplant. To determine the T-cell status, the percentage and the absolute numbers of CD3+, CD4+, and CD8+ cells per microliter of blood were evaluated. Absolute counts were calculated based on the proportion of these cells in the lymphocyte gate, percentage of lymphocytes, and complete blood counts. The CD16 + CD56+ cell numbers and percentages were determined to measure NK cells. To evaluate the B-cell status, we evaluated the percentage and the absolute counts of CD19+ B-cells and the serum levels of immunoglobulin (Ig) including IgG, IgM, and IgA. The lymphocyte reference ranges [7] were 801 to 2,534/╬╝L for CD3+ cells, 482 to 1,620/╬╝L for CD4+ cells, 341 to 1,352/╬╝L for CD8+ cells, 62 to 1,278/╬╝L for CD16 + CD56 + NK cells, and 71 to 830/╬╝L for CD19+ B-cells. The reference ranges of serum immunoglobulin were 408 to 1,788 mg/dL for IgG, 70 to 400 mg/dL for IgA, and 40 to 230 mg/dL for IgM.
Statistical analyses
The primary endpoint was the impact of clinical factors including GVHD prophylactic regimen in immune recovery of patients undergoing allogeneic HSCT. The secondary endpoints included the correlation between the immune recovery status and clinical outcomes. The clinical outcomes were disease-free survival (DFS), overall survival (OS), acute and chronic GVHD, non-relapse mortality (NRM), and relapse. All outcomes were measured from the time of stem cell infusion. The DFS was defined as survival without leukemia progression or relapse. Patients alive without disease progression or relapse were censored at the time of last contact. The OS was based on death from any cause. Surviving patients were censored at the time of last contact. Relapse was defined as the time to onset of hematologic recurrence or disease progression. Genetic relapse was assessed by the decrease in the rate of donor chimerism status below 95% or the reappearance of tumor target gene markers. NRM was defined as death from any cause without relapse in continuous complete remission or without progression. The incidence of grade II to IV or III to IV acute and chronic or extensive chronic GVHD was based on classical criteria [8,9].
The patients were categorized into two groups according to the immune recovery status 100 days after allogeneic HSCT. Based on quantitative analysis of peripheral lymphocytes via flow cytometry, the normal group was defined by T-cell subsets, B-cells, or serum immunoglobulins within their reference ranges, and the abnormal group was defined by levels outside the reference ranges.
Statistical differences in demographic and clinical characteristics between the normal and abnormal groups were evaluated using chi-square or FisherŌĆÖs exact test for categorical variables, and StudentŌĆÖs t test or WilcoxonŌĆÖs rank sum test for continuous variables. The Mann-Whitney U test was used to determine the statistical validity of non-parametric statistics depending on whether the intensive tendencies of two independent variables varied in the non-even distribution group. Probabilities of OS and DFS were estimated using Kaplan-Meier survival curves. Log-rank test was used to compare survival curves. A univariate Cox proportional hazards regression analysis was performed to correlate clinical variables with immune recovery. Based on the results of univariate Cox proportional hazard regression analysis, significant variables were selected for multivariate Cox proportional hazards regression analysis.
A p value of 0.05 was considered statistically significant. All statistical analyses were performed using SPSS 14.0 KO version for Windows (SPSS Inc., Chicago, IL, USA) and a freely available R 3.1.3 version (http://cran.r-project.org/).
RESULTS
PatientsŌĆÖ demographic and clinical characteristics
The study included a total of 114 patients. The demographic and clinical data are presented in Table 1. The median follow-up of the survivors was 43 months (range, 6 to 113). The median age at baseline was 43.5 years (range, 2 to 71). Sixty-two patients (54.4%) were male. Transplants were performed in 35 patients (30.7%) from 2004 to 2008, in 47 patients (40.2%) from 2009 to 2014, and in 32 patients (28.1%) from 2015 to 2017. Among the 114 patients, the most common type of disease was AML (n = 59, 51.8%) followed by ALL (n = 27, 23.7%). Eleven MDS patients and four lymphoma patients were included. Among the 11 MDS patients, six carried a lower risk, and five had a higher risk based on International Prognostic Scoring System of MDS at the time of diagnosis. Four lymphoma patients showing partial response to chemotherapy received HSCT. Other cases included multiple myeloma (n = 4), chronic myeloid leukemia in blast crisis (n = 3), severe aplastic anemia (n = 3), chronic lymphocytic leukemia (n = 2), and primary myelofibrosis (n = 1). We could not classify cytogenetic risk based on cytogenetic and molecular findings at diagnosis because of insufficient information available and changing criteria for risk stratification with time. Myeloablative conditioning regimens were used for 82 patients (71.9%). Thirty patients (26.3%) had a matching sibling donor, and others had alternative donors including matched unrelated donors (n = 68, 59.7%) and haplo-identical related donors (n = 16, 14%). In vivo T-cell depletion was performed in 78 patients (68.4%; thymoglobulin in 71 patients and alemtuzumab in seven patients). Ninety-two patients (80.7%) received tacrolimus-based regimen to prevent acute GVHD.
Outcomes of allogeneic hematopoietic stem cell transplantation
Most patients (98.2%) showed successful engraftment of donor cells, except for two patients with engraftment failure. The cumulative incidence of overall acute GVHD and grade II to IV acute GVHD on day 100 was 59.6% and 33.3%, respectively. The chronic GVHD rate at 3 years was 26.3% (Table 2). Viral reactivation including cytomegalovirus (CMV) and/or Epstein-Barr virus was identified in 71 patients (62.3%).
Three and 5-year OS rates were 76% and 59.4%, respectively. The number of deaths and causes of mortality over the entire follow-up period are shown in Table 2. The 1-year cumulative incidence of non-relapse mortality was 6.1% (n = 7). Forty-five patients (39.5%) died during the follow-up period and relapse occurred in 27 patients (23.7%). Relapse was the most frequent cause of death (n = 19). Other causes included acute and chronic GVHD (n = 14), infection (n = 8), engraftment failure (n = 2), and secondary cancers (n = 2).
Cox proportional hazards regression analysis was used to identify the impact of clinical variables on survival outcome. Disease status at the time of HSCT, risk stratification by HCI-CI, and chronic GVHD were significantly associated with survival outcome. Compared with CR status at HSCT, non-CR status at HSCT had a negative effect on OS (hazard ratio [HR], 2.54; p = 0.034). Moreover, high risk HCT-CI was associated with worse overall survival (HR, 2.94; p = 0.000). Chronic GVHD had a positive effect on survival outcome (HR, 0.30; p = 0.006), while moderate-to-severe acute GVHD (grade II to IV) tended to have a negative effect on overall survival without statistical significance (HR, 1.74; p = 0.068) (Table 3).
Clinical characteristics and immune recovery
One hundred four patients were evaluated for immune function reconstitution of T-cell subsets and humoral immunity 100 days after allogeneic transplantation (Table 4). The recovery of CD3+ T-cell was in the reference range in 88 patients (77.2%), whereas CD4+ cells recovered to normal levels in only 30 patients (26.3%). The CD8+ cells were restored to normal levels in 85 patients (74.6%). Among 108 patients assessed for NK cell status, 97 (89.8%) showed the normal range of NK cells. The B-cell recovery was in the reference range in 68 patients (59.6%). The serum levels of immunoglobulin G, A, and M were normal in 105 (92.1%), 78 (68.4%), and 85 (74.6%) cases.
Table 5 presents the results of statistical analyses of the individual effects of clinical variables on T-cell immune reconstitution. Prevention of GVHD using a tacrolimus-based regimen and T-cell depletion with thymoglobulin or alemtuzumab were significantly associated with delayed immune reconstitution of T-cells. The analysis of T-cell subset recovery according to clinical characteristics is summarized in Table 6. The median values of CD3+ and CD4+ cell counts were significantly lower in patients who underwent T-cell depletion than in patients without T-cell depletion. While CD8+ cell counts tended to increase in patients progressing to chronic GVHD, a significant decrease was detected in patients with acute GVHD and acute grade 2 or higher GVHD requiring active treatment, including steroids. The number of CD3+ cells was significantly reduced in patients progressing to chronic GVHD, and CD4+ cell counts tended to decrease in patients with CMV reactivation. However, there was no difference in T-cell subsets according to the relapse of underlying disease.
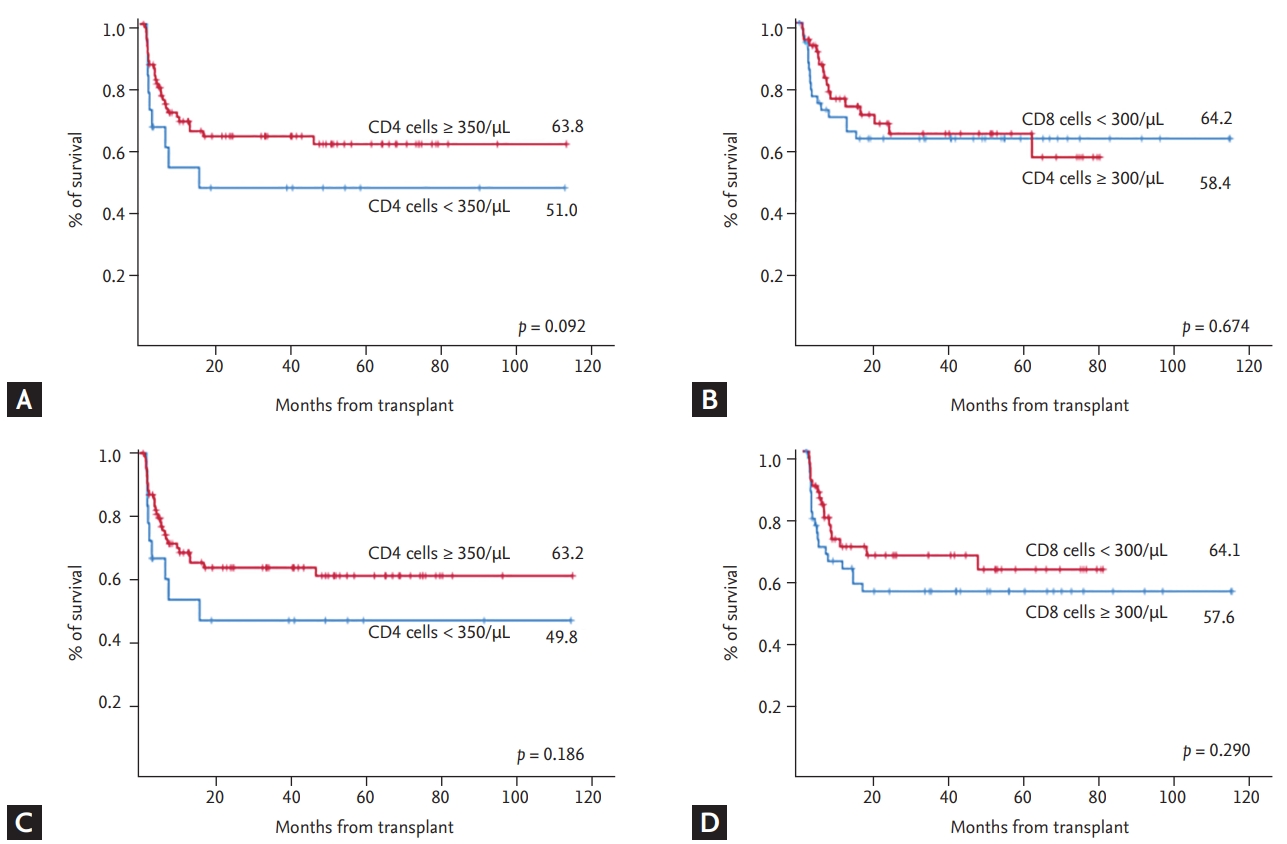
The difference in clinical outcomes depended on the analysis of T-cell recovery to normal status (Table 7). No significant differences in overall acute GVHD or grade II to IV acute GVHD were found between the normal and abnormal groups of T-cell reconstitution (p = 0.798 and p = 0.826, respectively). However, the incidence of chronic GVHD was significantly increased in the group with normal recovery compared to the abnormal group (p = 0.01). In addition, Epstein-Barr virus reactivation was more frequently detected in the abnormal group of T-cell subsets (p = 0.045). All viral reactivation events including CMV appeared to be more frequent in the abnormal group of T-cell subsets, but without statistical difference. Other variables were not significantly correlated with T-cell reconstitution. In the analysis of survival outcomes at 100 days after transplantation based on the recovery of T-cell subsets, the overall survival and relapse free-survival tended to be higher in patients with CD4+ cells recovering above 350/╬╝L, no without any statistical significance (Fig. 1). The recovery of CD8+ cells had no effect on the survival outcomes. T-cell depletion had the biggest negative effect on T-cell immune reconstitution (odds ratio, 6.71; p < 0.001) based on multiple logistic regression analysis (Table 8).
No significant variable was found to affect the recovery of NK cells (Table 9). However, patients receiving greater than 6 ├Ś 106 CD34+ cells/kg more frequently reached the reference range than patients receiving fewer than 6 ├Ś 106 CD34+ cells/kg, with nearly statistical significance (p = 0.054). We did not find any impact of B-cell recovery status on clinical outcomes after transplantation.
DISCUSSION
The recovery of innate and adaptive immune systems occurs gradually during the post-transplantation period. The timing of immune reconstitution is affected by many variables during the transplantation, such as the source of stem cells, disparity of human leukocyte antigen and minor histocompatibility antigen, the conditioning regimen, graft manipulation, immune suppressive therapy (especially corticosteroids), and the presence of GVHD [1]. Given the complexity of the transplantation process, it is impossible to quantify the impact of any one of these factors on individual engraftment; all of these factors work in concert to regulate immune reconstitution.
The type of conditioning regimen affects immune recovery after transplantation, and varies depending on treatment intensity and the effect of immunosuppression. Fludarabine has been widely used in reduced intensity conditioning regimens in combination with other drugs, confirming the effect of strong immunosuppressive effect on donor cell engraftment and in reducing non-relapse mortality [10]. However, the effect of fludarabine on T-cells was attributed to increased relapse after transplantation, resulting in poor DFS, and the OS was not improved compared to other pretreatment regimens [11].
Since the recovery of immune function after transplantation is affected by a wide variety of clinical conditions, data pertaining to the recovery of each cell over time are scarce. In the case of peripheral blood stem cell transplantation, neutrophil recovery occurs at approximately 2 weeks. The recovery of NK cells occurs at 1 to 3 months and earlier than the recovery time of more than 1,000/╬╝L CD4+ T-cells [5]. CD8+ T-cells recover faster than CD4+ T-cells but 100 days after transplantation. Similar results were obtained in this study (Table 6). The number of lymphocytes recovered up to 100 days after transplantation affects the transplantation outcome. In the present study, we found that the degree of recovery of CD4+ cells tended to affect the clinical outcomes. Therefore, early recovery of T-cells after transplant may have important clinical implications. The engraftment of neutrophils and platelets was achieved at a median of 11 days after transplant. NK cell counts were restored to the normal range in about 90% of patients by day 100 post-transplantation. Successful engraftment of neutrophils, platelets, and NK cells was obtained at similar times, as described previously.
In patients undergoing HSCT, the adaptive immune system is significantly impaired largely due to the loss of naïve T-cells and the reduced function of existing T-cells [12]. A functional thymus is essential to generate an effective T-cell repertoire following HSCT. However, thymus-dependent differentiation of T-cells, particularly in the case of CD4+ T-cells, is a critical hurdle in aging patients who commonly experience thymic atrophy [13]. The peripheral naïve T-cell receptor repertoire is never fully restored in older patients and infectious morbidity is directly related to low CD4+ T-cell counts [14]. Whereas CD8+ T-cells are predominantly derived by clonal expansion that occurs outside the thymus [15], CD8+ T-cell recovery is not affected by aging [16]. Within the first 100 days after HSCT, cellular immunodeficiency due to insufficient NK cells and T-cells increases the susceptibility of patients to viral reactivation including CMV and Epstein-Barr virus, as well as viral diseases [17,18].
In this study, T-cell subsets including CD3+ T-cells, CD4+ T-cells, and CD8+ T-cells returned to the reference range in about 40% of patients within 100 days after HSCT. Evaluating the risk of viral reactivation according to T-cell recovery status revealed that the risk of EBV reactivation was higher in the abnormal group than in the normal group. All viral reactivation events including CMV reactivation appeared to be more frequent in the abnormal group of T-cell subsets. The absolute number of CD4+ cells in patients with CMV reactivation was significantly lower than in patients without CMV reactivation. Therefore, viral reactivation might be directly correlated with T-cell recovery status.
In addition, we assessed the impact of clinical variables on T-cell reconstitution. GVHD prophylaxis with the tacrolimus-based regimen and T-cell depletion before HSCT resulted in delayed immune reconstitution of T-cells. T-cell depletion was a serious adverse effect following T-cell recovery. Acute GVHD tended to negatively affect the recovery of T-cell subsets; however, no consistent results with statistical significance were observed. Clinical risk factors for immune reconstitution including the source of stem cells, degree of human leukocyte antigen disparity, and conditioning regimen were not significantly associated with delayed immune recovery in this study. The addition of fludarabine with greater immunosuppressive effects to conditioning regimen reduced the frequency of acute GVHD during the early period after transplantation, even though over two-thirds of donors were alternative donors. Since 2011, selectively targeted therapy including ruxolitinib, imatinib, or cell therapy has been used to actively treat acute GVHD patients. Further, decreased use of long-term or high-dose steroids, was observed. The incidence of chronic GVHD was higher in the normal group of T-cell subsets than in the abnormal group, which differed from a prior report that suggested possible immune dysfunction in patients who developed chronic GVHD after HSCT [19]. The difference might be related to the lower incidence of extensive chronic GVHD requiring systemic therapy including corticosteroids. However, the exact cause leading to the difference is unclear.
The humoral immune response is mediated by antibodies and requires both functional B- and T-cells. In addition to the delayed recovery of T-cells described above, a significantly impaired reconstitution was observed in cells of B-cell lineage following HCT [20]. After HSCT, the reconstitution of B-cell repertoire is often delayed because of complications associated with GVHD, age, and infections [21]. Normal B-cell counts are reached between 6 and 9 months after HSCT and after more than 12 months post-GVHD. Antibody production is also impaired after HSCT. Serum IgM levels return to normal usually within 3 to 6 months, whereas recovery of serum IgG levels may be delayed up to 1 year or longer. Impaired antibody immunity has been correlated with an increased risk of infections after HSCT primarily due to encapsulated bacteria [22]. In this study, about 60% of the patients achieved the normal range of B-cell counts and serum levels of immunoglobulin including IgG, IgM, and IgA 100 days after transplantation. B-cell recovery appeared to be faster than the reported incidence, even with GVHD and older age. No risk factor was associated with delayed B-cell reconstitution.
This study has several limitations. Major limitations were the participation of patients diagnosed with various hematologic diseases and the different types of transplantation using various donor types. Because the disease per se or the treatment process might be affected by the immune system, it may be difficult to obtain objective results due to a possible selection bias. Further, the small sample size prevented definitive conclusions. Therefore, classification of patients into uniform groups and further analysis based on groups was a difficult task. Finally, only absolute counts of lymphocyte subsets (CD3+ T-cells, CD4+ T-cells, CD8+ T-cells, and NK cells) were relatively simple and facilitated the evaluation of immune reconstitution. However, functional assessment tests such as T-cell repertoire and T-cell receptor expression were not performed.
In summary, there is a delayed immune reconstitution in patients undergoing allogeneic HSCT with tacrolimus-based GVHD prophylactic regimens, T-cell depletion, and possibly due to acute GVHD resulting in increased morbidity from viral reactivation. Treatment strategies to prevent infectious complications are needed to enhance immune reconstitution and recovery following allogeneic HSCT with fludarabine-based conditioning.
KEY MESSAGE
1. The immune recovery status post-allogeneic hematopoietic stem cell transplantation (HSCT) was affected by graft-versus-host disease (GVHD) prophylactic regimens, T-cell depletion, and possibly those manifesting acute GVHD.
2. Delayed immune reconstitution resulted in increased morbidity from viral reactivation.
3. Treatment strategies to prevent infectious complications are needed to enhance immune reconstitution following allogeneic HSCT with fludarabine-based conditioning.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





