


INTRODUCTION
Incidence of colorectal cancer (CRC) has increased in the world (8.2 per 100,000 in year 2008 vs. 17.2 per 100,000 in year 2012) [1,2].Interestingly, there is sex difference of CRC in terms of incidence (10.0 per 100,000 in males vs. 9.2 per 100,000 in females) and mortality (8.0 per 100,000 in males vs. 9.0 per 100,000 in females). In Korea, the incidence of CRC has rapidly increased; CRC became the second most common cancer (52.6 per 100,000). CRC was the sixth most common cancer (16.3 per 100,000) among cancers that caused mortality [3]. Similar to other countries, there is also sex difference of CRC in term of incidence (62.5 per 100,000 in males vs. 42.7 per 100,000 in females) and mortality (18.5 per 100,000 in males vs. 14.1 per 100,000 in females) in Korea [4,5]. Male is a risk factor of CRC. CRC also develops earlier in males than in females. Thus the screening protocol of CRC should be different between males and females [4,5]. However, CRC screening guidelines do not distinguish males and females. CRC developed from proximal (right-sided) or distal (left-sided) colon shows differences in incidence according to geographic region, age and sex [6,7]. It is known that patients with proximal colon cancer are older and having more females than those with distal colon cancer. In addition, there is a difference in cancer morphology. That is, proximal colon cancer is more often flat while distal colon cancer has a polypoid-type which can be more easily detected by colonoscopy [8]. Tumor location and prognosis of CRC are also different between males and females. However, studies that consider sex specific design and interpretation of CRC are insufficient.
Colonoscopy is important for screening and diagnosis of CRC [5]. As inadequate bowel preparation affects the effectiveness and accuracy of colonoscopy examination. Thus, bowel preparation and colonoscopy quality management are important [9,10]. Several studies have reported that age, sex, physical activity, and disease are associated with bowel preparation [11-13]. The length of colon is known to be longer in females than in males [14,15]. However, there has been no research on each factor so far. In addition, previous studies have not identified other colonoscopy quality factors including cecal intubation rate, insertion time, and polyp detection rate together [11-13]. We hypothesize that there are sex differences in colonoscopy preparation quality, cecal intubation time, and withdrawal time (from point of cecal intubation to final withdrawal). If there is difference in colonoscopy quality between sexes, CRC screening guidelines which do not distinguish females from males should be revised to improve the high mortality and poor prognosis of female CRC patients [1-4]. With this background, the aim of this study was to determine sex difference of colonoscopy quality in terms of bowel preparation, insertion time, withdrawal time, and polyp detection rate.
METHODS
Data source
Medical records and colonoscopy readings of subjects who underwent colonoscopy at Seoul National University Bundang Hospital (SNUBH) from March 2015 to April 2018 were analyzed.
Informed consent was waived by Institutional Review Board of SNUBH (No. B-1812/513-106). Subjects were searched using SNUBHŌĆÖs Clinical Data Warehouse, the hospitalŌĆÖs own database analysis program [16]. In addition, medical information was collected from electronic medical record system, including sex, age, past medical history, indication of colonoscopy, sedation medication, name of colonoscopist, colonoscopy finding, Boston bowel preparation score (BBPS), number of polyp, number of diverticulum, cecal intubation time and withdrawal time. We excluded colonoscopy cases with history of surgery on colon or abdomen. In addition, colonoscopy cases done by colonoscopists within 5 years were excluded.
Analysis of colonoscopy quality indicators
We examined sex difference of baseline characteristics including age, history of surgery, indications of colonoscopy, sedation medication and bowel preparation drug. We also identified sex difference of colonoscopy quality indicators including BBPS, cecal intubation rate, cecal intubation time, withdrawal time and polyp detection rate [9,10].
There are various bowel preparation scales including Aronchick bowel preparation scale (ABPS) [17-20], Ottawa bowel preparation scale (OBPS) [18-20], and BBPS [19-21]. The ABPS was widely used to assess bowel preparation quality ranging from excellent (1 point) to inadequate (5 points) by evaluating the percentage of total colonic mucosal surface covered by fluid or stool without scoring separate colon segments [19]. The OBPS can access colonic mucosal cleanliness by colon segment on a scale of 0 (excellent) to 4 (inadequate). The BBPS was developed in 2009. It has been validated in various studies [19-21]. The BBPS separates the colon into three segments: right, transverse, and left colon. Each segment is scored from 0 to 3, with a score of 3 indicating good bowel cleansing. Total score for the three segments ranges from 0 to 9. We chose the BBPS to assess bowel preparation. The BBPS is a useful scale because it is associated with polyp detection rate and follow-up interval of colonoscopy [21,22].BBPS score higher than 6 was defined as adequate bowel preparation. A recent study has defined adequate preparation as having BBPS score of 2 or 3 for all colon segments [23].If a subject had a BBPS score of 0 or 1 in any colon segment, the preparation was considered inadequate.
Difference of BBPS was analyzed according to two kinds of bowel preparation drugs, Coolprep (Taejoon Pharmaceutical, Seoul, Korea) and Picosolution (Pharmbio Korea, Seoul, Korea). Coolprep consists of two pouches (A and B). Components of pouch A contain polyethylene glycol 50 g, potassium chloride 0.5075 g, sodium chloride 1.3455 g and sodium sulfate anhydrous 3.75 g. Components of pouch B contain ascorbic acid 2.35 g and sodium ascorbate 2.95 g. This should be diluted in 2 L before intake. Components of Picosolution in 170 mL contain citric acid 12 g, magnesium oxide 3.5 g and sodium picosulfate hydrate 10 mg. After drinking each bottle of Picosolution in 170 mL subjects should drink 1 L water according to the regimen. However, when subjects had history of constipation three bottles of Picosolution (510 mL) were recommended.
Statistical analyses
Continuous variables are expressed as mean ┬▒ SD (range). Categorical variables are presented as absolute values and percentages. All quantitative variables were compared between the two groups using an independent samples t test to evaluated sex difference of colonoscopy quality indicators. FisherŌĆÖs exact test was used for categorical variables as appropriate. All statistical tests were two-sided without adjustment for multiple comparisons. Statistical significance was considered when p value was less than 0.05. All analyses were carried out using SPSS for Windows version 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
Subject characteristics
Data from 12,561 colonoscopies were analyzed. These colonoscopies were done by 11 colonoscopists who were professors in gastroenterology with colonoscopy experience of 5 years or more. Colonoscopies were performed for 6,413 males and 6,148 females. Characteristics of these 12,561 cases are shown in Table 1. Age was similar between male and female groups (57.5 ┬▒ 13.8 years vs. 57.8 ┬▒ 13.5 years, p = 0.695). The ratio of screening colonoscopy was similar between males and females (p = 0.425). The ratio of colonoscopy due to symptom (abdominal pain, hematochezia, and diarrhea) was higher (p < 0.001) in females. On the contrary, the ratio of colonoscopy due to CRC, polyp, and inflammatory bowel disease (IBD) was higher in males (p < 0.001, respectively) [3]. The dose of midazolam for sedation was higher in males (4.5 ┬▒ 1.0 mg vs. 4.3 ┬▒ 1.2 mg, p < 0.001). However, the dose of pethidine was lower in males (36.7 ┬▒ 12.8 mg vs. 38.2 ┬▒ 12.9 mg, p = 0.001). Picosolution was more frequently selected for bowel preparation solution in females (p < 0.001).
Sex difference of colonoscopy quality indicators
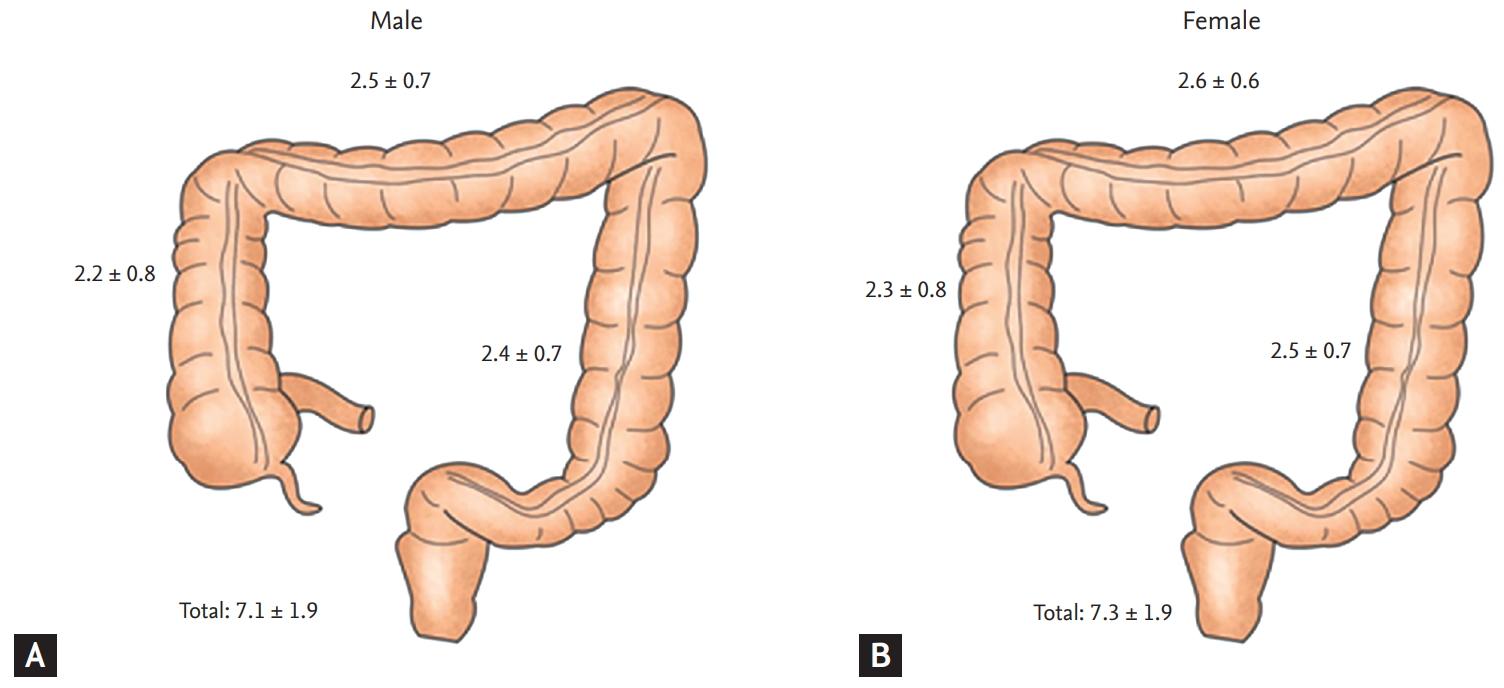
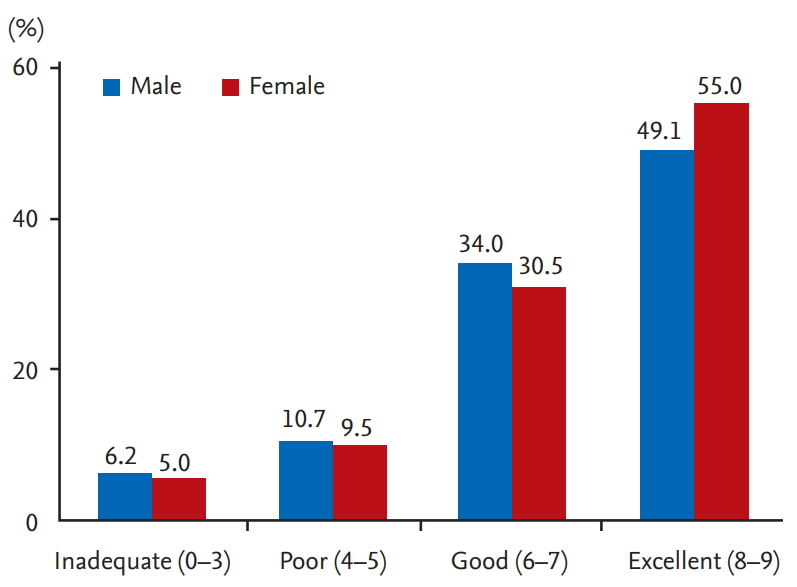
Total BBPS indicating the degree of colon cleanness was lower in males (7.2 ┬▒ 1.9 vs. 7.4 ┬▒ 1.8, p = 0.001). Each segment was slightly higher in females than in males (Table 2, Fig. 1). The proportion of patients with an adequate bowel preparation (BBPS Ōēź 6) was significantly lower in males than female group (5,437 [84.8%] in males vs. 5,340 [86.9%] in females, p = 0.001). The proportion of patients with an adequate bowel preparation (BBPS Ōēź 2 for all segments) was also significantly lower in males than in females (5,097 [79.5%] in males vs. 5,048 [82.1%] in females, p < 0.001). In addition, we classified patients by preparation result of BBPS (inadequate, 0 to 3; poor, 4 to 5; good, 6 to 7; excellent, 8 to 9) (Fig. 2). The ratio of patients with excellent preparation result (BBPS 8 to 9) was significantly (p < 0.001) higher in females than in males (Table 2). The ratio of patients with inadequate preparation result (BBPS 0 to 3) was significantly (p < 0.001) higher in males.
There was no significant difference in cecal intubation rate between males and females (95.2% in males vs. 95.4% in females, p = 0.512) (Table 2). However, cecal intubation time was significantly longer in females (male, 6.2 ┬▒ 6.1 minutes vs. female, 8.3 ┬▒ 6.4 minutes, p < 0.001). In addition, withdrawal time was significantly longer in males (7.9 ┬▒ 3.5 minutes in males vs. 7.4 ┬▒ 3.1 minutes in females, p < 0.001).
Colonoscopy biopsy was more frequently performed in males (p < 0.001). Polyp detection rate was also higher in males (32.1% vs. 20.8%, p < 0.001) (Table 3). In addition, the number of cases with three or more polyps was higher in males (p < 0.001). Diverticulum was also more frequently detected in males (9.5% vs. 6.1%, p < 0.001).
Sex difference of bowel preparation score according to drug
We also analyzed sex difference of BBPS according to bowel preparation drug (Table 4). Coolprep was the most commonly used bowel preparation drug (n = 12,160). Picosolution was used in 381 patients. Total BBPS score of Coolprep was significantly lower in females (7.2 ┬▒ 1.9 in males vs. 7.4 ┬▒ 1.8 in females, p = 0.026). Adequate bowel preparation (BBPS Ōēź 6) of Coolprep was also lower in males (5,288 [84.6%] in males vs. 5,125 [86.7%] in females, p = 0.001). In recent guideline of adequate bowel preparation (BBPS Ōēź 2 for all segments), the ratio of adequate bowel preparation with Coolprep was lower in males (4,956 [79.3%] in males vs. 4,841 [81.9%] in females, p < 0.001). However, there was no sex difference in the ratio of bowel preparation with Picosolution.
Next, we analyzed sex difference of BBPS according to history of polypectomy and IBD (Table 5). Regarding history of polypectomy, total BBPS (7.4 ┬▒ 1.8 in males vs. 7.7 ┬▒ 1.6 in females, p < 0.001), adequate bowel preparation (BBPS Ōēź 6) (958 [88.3%] in males vs. 572 (91.7%) in females, p = 0.028), and achievement of adequacy (911 [84.0%] in males vs. 550 [88.1%] in females, p = 0.018) were significantly lower in males.
For cases with IBD, adequate bowel preparation was significantly higher in males (359 [96.8%] in males vs. 196 [91.6%] in females, p = 0.011).
DISCUSSION
Recently, there has been a growing interest in sex specific difference. Some studies have reported health difference between males and females [14,15,24]. Sex and gender differences show diverse physiological and psychological factors. Sex hormones and gender differences might play important roles in disease development and progression [24]. For instance, Menon et al. [25] have suggested that sex hormones can directly affect bacterial metabolism, bacterial growth, and gene expression of virulence factors through steroid nuclear receptor expression including estrogen receptor ╬▓.In addition, Kim et al. [26] have demonstrated that reflux symptoms affect female patients with gastroesophageal reflux disease more than in male ones, and quality of life was also more impaired in females.In terms of cancer, Kotake et al. [27] have shown that reduced risk of cancer-specific death for women relative to men persists over time. Zheng et al. [28] have shown that sex hormones play a crucial role in the pathogenesis and development of hepatitis B virus-induced hepatocellular carcinoma. Males with private insurance undertook colonoscopy more frequently [29]. However, employed males were less likely to eat salty food, be older, and smoke [29]. Diagnostic interval was longer for females than for males in CRC (mean difference; 10.4 days; 95% confidence interval, 4.3 to 16.5; p = 0.001) [30].
There have been some reports regarding sex difference in colonoscopy quality [13,31-33]. Ness et al. [13] have suggested that male sex (odds ratio, 0.85) is associated with inadequate bowel preparation. Similarly, Rotondano et al. [31] have examined factors associated with quality of bowel cleansing and found that men gender is a predictor of inadequate cleansing at right colon and left colon (p = 0.040 and p = 0.014, respectively). In addition, Akere and Otegbayo [32] have examined 167 patients to find factors affecting cecal intubation time. They found that men are associated with prolonged cecal intubation time (913.86 ┬▒ 453.28 seconds in males vs. 910.44 ┬▒ 513.33 seconds in females, p = 0.443). In contrast, males showed higher success rate of cecal intubation within 20 minutes than females (83.9% in males vs. 77.6% in females, p = 0.004) [33]. However, there is a lack of research that conclusively proves the sex difference in colonoscopy quality. In addition, previous studies have limitation such as small sample size [31] and insufficient variables [31,32].In addition, there has been no research analyzing colonoscopy quality between males and females like the present study. Furthermore they only statistically analyzed sex as one factor for multivariance [13,31-33].There are various colonoscopy quality indicators including colonoscopy surveillance, cecal intubation rate, adenoma detection rate (Ōēź 25% in males and Ōēź 15% in females), colonoscopy withdrawal time (average Ōēź 6 minutes) and quality of colon preparation [34]. However, few studies have been performed with a comprehensive approach in terms of sex specific manners.
In the present study, we investigated sex difference in colonoscopy quality in many aspects using a big administrative database. Colonoscopy quality indicators including adenoma detection rate, colonoscopy withdrawal time, and quality of colon preparation are important to detect colon polyp and CRC in early stages [34]. However, there has been no study about sex difference in these indicators. Males and females have different incidence and mortality of CRC. Our results suggest that sex difference of colonoscopy quality indicator might be associated with early detection and mortality of CRC.
Clearly, sex difference was identified in bowel preparation. We analyzed various guidelines for adequate bowel preparation and found that females showed better bowel preparation results. It is known that bowel preparation is influenced by various factors [11-13,35,36]. Our study showed that sex factor could influence bowel preparation based on a large cohort database. Our results suggest that we should more carefully educate male patients who receive colonoscopy for adequate bowel preparation. Whether sex difference of bowel preparation is associated with chromosome or genetic difference merits further study.
Our study showed sex difference in cecal intubation time and withdrawal time. Sex difference of cecal intubation time might be associated with anatomical difference between males and females [14,15]. Thus, we need to schedule female patients with enough colonoscopy time. Sex difference of withdrawal time might be associated with polyp detection rate. Male showed higher polyp detection rate. Therefore, withdrawal time in males might need to be longer than in females.
Our study showed that polyp detection rate was different between males and females. It might be associated with the higher incidence of CRC in males [1-3]. Thus, careful colonoscopy inspection is needed for males. These results suggest that different indication of colonoscopy and colonoscopy follow-up interval might be needed based on sex difference of bowel preparation method and colonoscopy withdrawal time. More studies are needed to determine the appropriate colonoscopy follow-up term for males.
We analyzed sex difference of bowel preparation with bowel preparation drugs Coolprep and Picosolution widely used in Korea. Some studies have reported that these two drugs have no significant adverse effects with similar bowel of cleansing [37-40]. In the present study, females showed better total BBPS score, adequate bowel preparation (BBPS Ōēź 6), and recent adequate bowel preparation (BBPS Ōēź 2 for all segments) in Coolprep. However, there was no sex difference in cases of Picosolution in contrast to Coolprep. We cautiously believe that the reason might be because subjectsneedes to drink 2 L of Coolprep with mixed solution from the beginning. Thus, males might not have followed the instruction more precisely than females. Our results suggest that bowel preparation might be different depending on which bowel preparation drugs are taken. Thus, male patients should be educated how to clean bowel more carefully. In addition, it is necessary to study how to clean the bowel in males. Whether different bowel preparation drugs show different effectiveness remains controversial. Previous reports have suggested that bowel preparation is associated with not only drugs, but also drug compliance and fiber diet education [35,36]. Our study showed that there was a sex difference in bowel preparation status using bowel preparation drugs. Thus, when Coolprep or Picosolution was planned, this result should be carefully considered. In addition, there was a difference in size between Coolprep and Picosolution groups. Therefore, more studies are needed.
We thought that analysis of colonoscopy by experienced colonoscopists was our studyŌĆÖs strength. The skill and career of colonoscopist depending on training period can affect cecal intubation time and polyp detection rate. Our study eliminated the selection bias due to exclusion of colonoscopy cases by colonoscopists with experience of less than 5 years.
However, our study has some limitations. First, this study was performed in one institute due to the Personal Information Protection Acting Korea. However, there was an advantage of research because description format was made before this study. Thus a consistent approach was possible and description was well educated with the figure to avoid selection bias. Second, we analyzed colonoscopy information according to electronic medical records for a large number of cases. However, we could not verify other factors such as patientŌĆÖs compliance and history of colonoscopy. In addition, our study could not deal with analysis of pathologic result. We thought that analysis of pathologic findings including grade of adenoma and carcinoma should be needed.
In conclusion, there was a sex difference in colonoscopy indicator. Males showed less clean bowel preparation. However, polyp detection rate in males was higher than that in females. Thus, males should be educated regarding how to perform bowel preparation carefully. Colonoscopists need to reserve relatively more time of colonoscopy for females. Whether the sex difference of various colonoscopy indicators is associated with chromosome or genetic difference merits further study.
KEY MESSAGE
1. We identified sex difference in bowel preparation, cecal intubation time, withdrawal time, and polyp detection rate. Males had poorer bowel preparation and higher polyp detection rate than females.
2. Males need education regarding how to perform bowel preparation carefully. Females need plenty of time for colonoscopy insertion. Males need plenty of withdrawal time.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





