


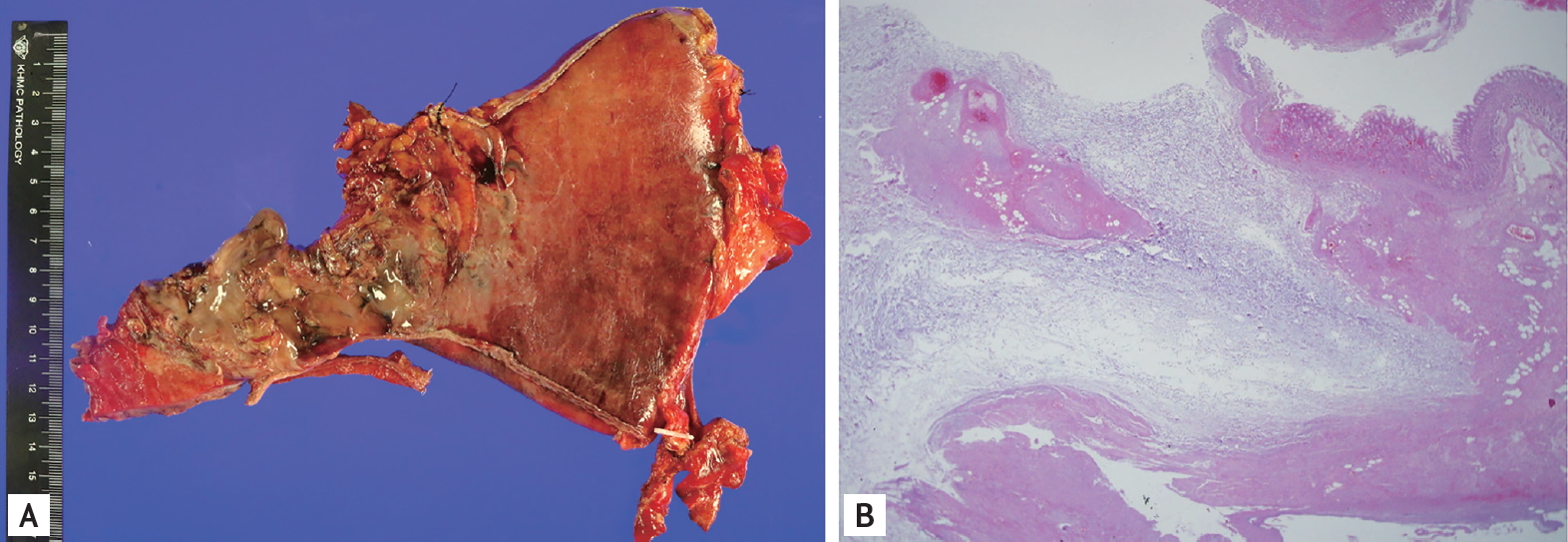
A 74-year-old man presented with a 10-day history of nausea and vomiting. He had been diagnosed as having diabetes mellitus, for which he was followed at a local clinic. Laboratory data revealed hypotension (60/45 mmHg), leukopenia (2,850/µL), and elevated C-reactive protein levels (38.97 mg/dL), which were indicative of sepsis. Although no acute signs or symptoms were observed, immediate computed tomography (CT) study was performed to determine the cause of the sepsis. The scout image showed a collection of mottled gas surrounding a kidney shadow within the left abdomen, indicating a retropneumoperitoneum (Fig. 1A). CT images showed an intramural rim-enhancing fluid collection at the gastric fundus, presumably an intramural abscess. The gastric wall of the esophagogastric (EG) junction and the fundus were poorly visible, and an extensive retroperitoneal abscess and air collections were found within the left anterior and posterior pararenal spaces (Fig. 1B and 1C). We suspected sepsis due to a gastric retroperitoneal perforation, and the patient was referred for emergent surgery. Necrosis of the gastric fundus and EG junction, and profound retroperitoneal inflammation were found during surgery; therefore, a proximal gastrectomy and delayed esophagojejunostomy were performed. Microscopic examination revealed a transmural infarction with a submucosal abscess involving the EG junction and fundus (Fig. 2). The patient was doing well at 1-year postoperative follow-up. Written informed consent was obtained.
In this case, the patient showed no acute signs or symptoms that would have indicated a surgical abdomen. Instead, he presented with vague symptoms, including nausea and vomiting. An unusual retroperitoneal perforation of a gastric abscess, manifesting vague signs and symptoms, masked the surgically emergent condition. However, in a patient with diabetes mellitus, sepsis may warrant further evaluation. Retroperitoneal extension of a gastric abscess is an unusual but possible condition because of the extraperitoneal portion of the stomach. This is the gastric bare area, which encroaches upon the posterior surface of the gastric fundus and subcardial portion. Proximal gastric cancers or inflammation can invade the gastric bare area and, from there, the retroperitoneum.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





