


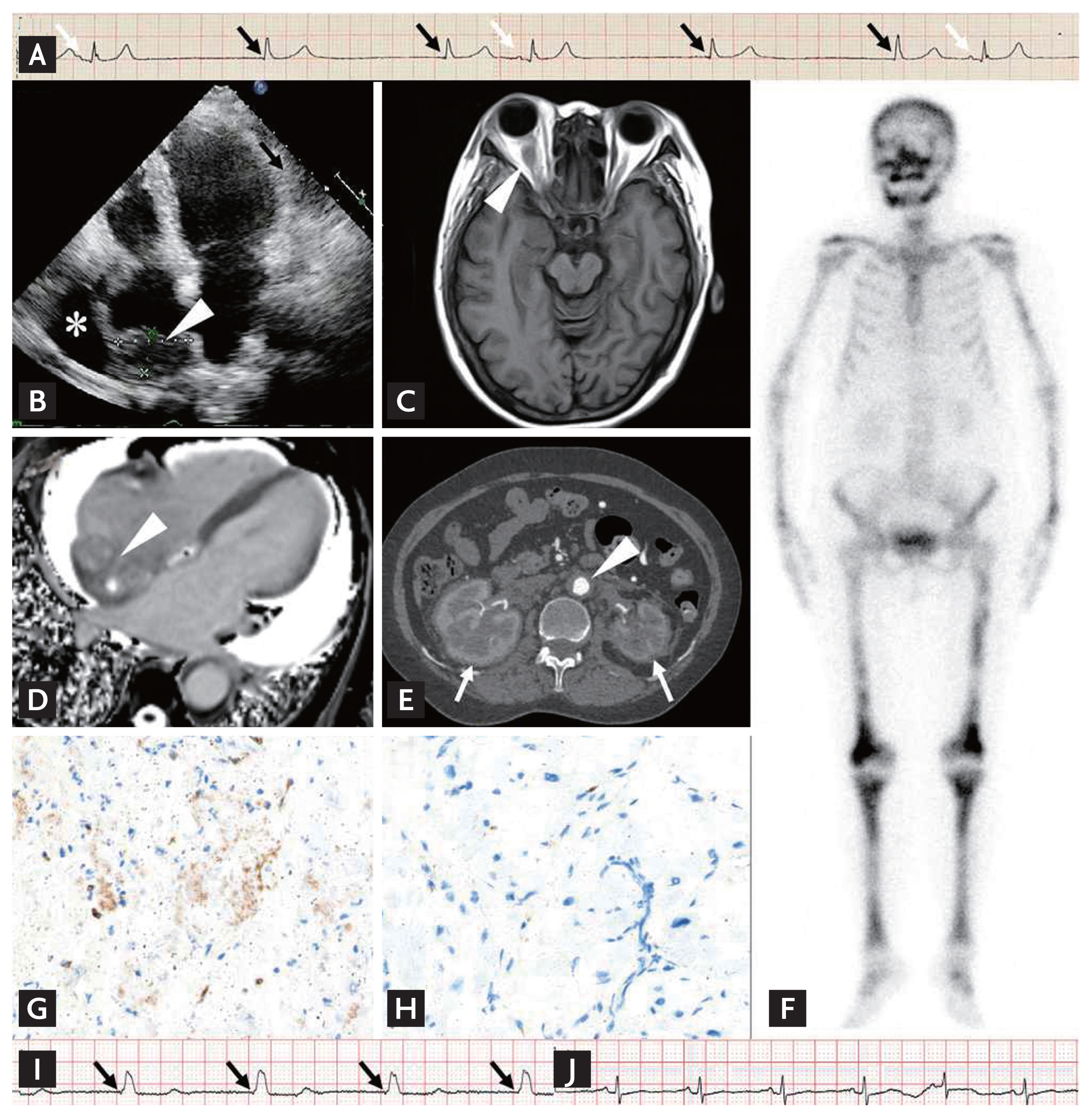
A 64-year-old woman was admitted because of progressive exertional dyspnea for 4 years and recurrent syncope for 2 days. A diagnosis of sinus node syndrome (SSS) was confirmed based on sinus arrest with atrioventricular junctional escape rhythm on electrocardiogram (Fig. 1A). Further cardiac and neurological examinations revealed a mass on right atrium (RA) and pericardial effusion on echocardiography (Fig. 1B), and a right retro-orbital lesion with normal T1-hypointense enhancement but short T2hypointense enhancement (Fig. 1C) on cerebral magnetic resonance imaging (MRI), indicating Erdheim-Chester disease (ECD). Ancillary imaging examinations further demonstrated typical features of ECD, including the irregular mass on the RA and a right atrio-ventricular groove with relatively shorter T1 and longer T2 relaxation times (Fig. 1D) on cardiac MRI, a ŌĆścoated aortaŌĆÖ and a ŌĆśhairy kidneyŌĆÖ (Fig. 1E) on computed tomography, and symmetrical increased uptake of radiotracer in the skull and long bones of the extremities (Fig. 1F) on bone scintigraphy. ECD was finally confirmed by myocardial mass biopsy with typical histological and immunohistochemistry findings of CD68(+), CD1a(ŌłÆ), S100(ŌłÆ) (Fig. 1G and 1H) with negative BRAFV600E mutation. A single chamber ventricular pacemaker was implanted for SSS treatment, and 3 million units of interferonalpha was administered twice a week for ECD treatment. The patient was pacemaker-dependent at the 2-month follow-up (Fig. 1I), but displayed a restored intrinsic sinus rhythm after 4 months of interferon-alpha treatment (Fig. 1J).
As a non-Langerhans cells histiocytosis with multiorgan involvement, 70% of patients with ECD have abnormal heart imaging. The most common finding is RA infiltration. In a previous similar case with RA involvement and SSS, an RA lead was implanted in an area with a less thickened wall and no delayed enhancement on cardiac MRI. However, we abandoned the RA approach in consideration of not only the technical difficulties, but also the progression of infiltration that might compromise pacing function. Moreover, the patient experienced SSS remission after interferonalpha treatment, but longer follow-up was needed to observe the long-term effect.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





