


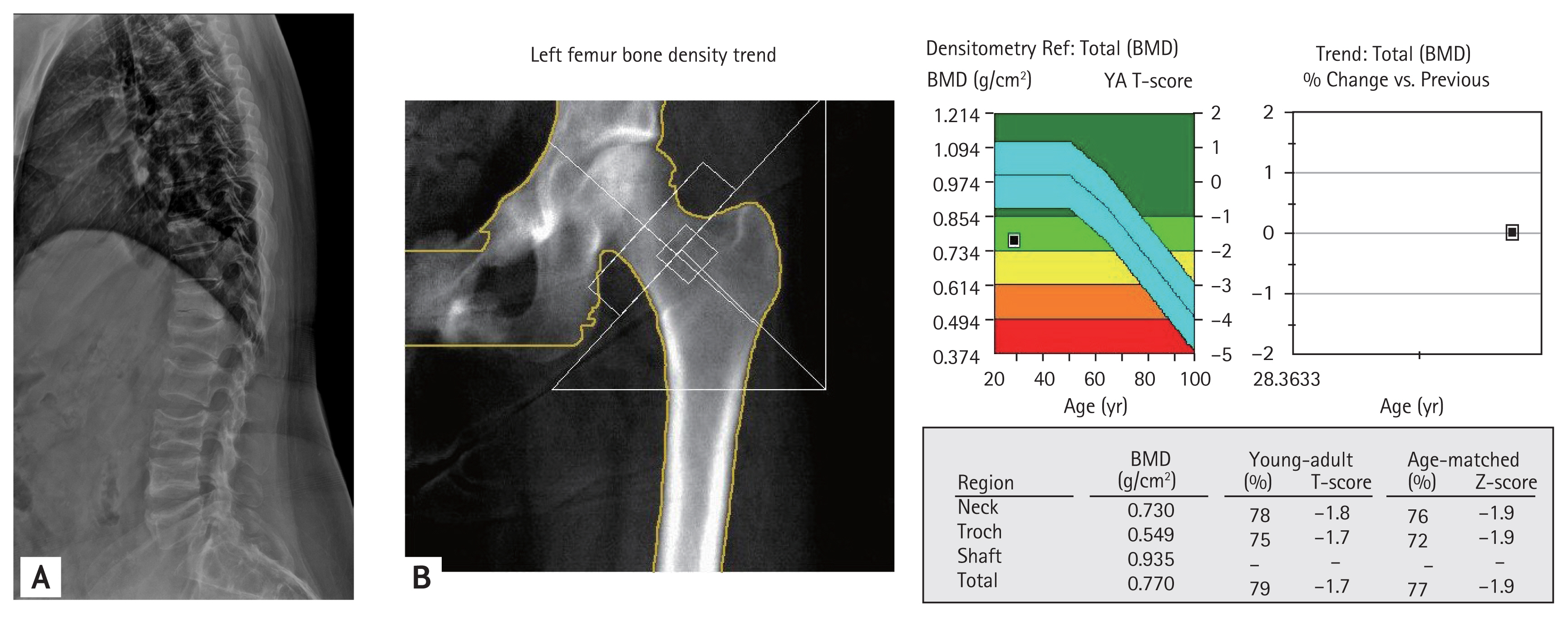
A 28-year-old woman visited the endocrinology department with a chief complaint of back pain after falling. Four months ago, she had preeclampsia and gestational diabetes mellitus, which resulted in the premature delivery of her second baby at 29 weeks of gestation. Her first baby was also delivered prematurely at 35 weeks of gestation 1 year ago. The patient’s height, weight, and blood pressure were 155 cm, 63 kg, and 148/100 mmHg, respectively. Additionally, truncal obesity and purple abdominal striae were observed. On radiography, multiple compression fractures were observed in the thoracic and lumbar vertebrae. In particular, T9, T10, T12, and L1 to L4 were fractured (Fig. 1A). The bone mineral density of the lumbar spine could not be evaluated owing to a fracture. Her hip Z-score was −1.9 (Fig. 1B). Contrast enhanced computed tomography scan of the abdomen was conducted to reveal a mass measuring 2.8 × 2.0 mm in size on the right adrenal gland (Fig. 2). Hormonal tests of the adrenal gland were performed, and the results were as follows: 0.9 ng/mL/hr plasma renin activity, 5.7 ng/dL aldosterone, 6.3 ratio of aldosterone to renin, 0.09 nmol/L (< 0.50) plasma metanephrine, 28.4 μg/dL serum cortisol, 1.37 pg/mL adrenocorticotropic hormone (ACTH), and overnight 1-mg dexamethasone suppressed cortisol of 28.6 μg/dL (< 1.8). The results were compatible with ACTH-independent Cushing’s syndrome (CS). Weekly alendronate with daily calcium and cholecalciferol replacement therapy was initiated for osteoporosis. After a laparoscopic removal of the adrenal mass, her morning serum cortisol level decreased to 1.1 μg/dL. Active CS during pregnancy is associated with a high rate of maternal and fetal complications. Pregnancy-associated CS is easy to overlook and remains a diagnostic challenge. This is because pregnancy itself is rare in CS patients. Various symptoms and signs of CS can also occur in relation to normal pregnancy. Furthermore, interpretation of diagnostic tests is also difficult. The predominant etiology of CS is adrenal adenoma, which is reported in 40% to 60% of cases. The present case demonstrates the importance of considering CS as a differential diagnosis in a patient who presents with multiple vertebral fractures, preeclampsia, or gestational diabetes mellitus, regardless of whether the patient is pregnant or postpartum.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




 |
 |