


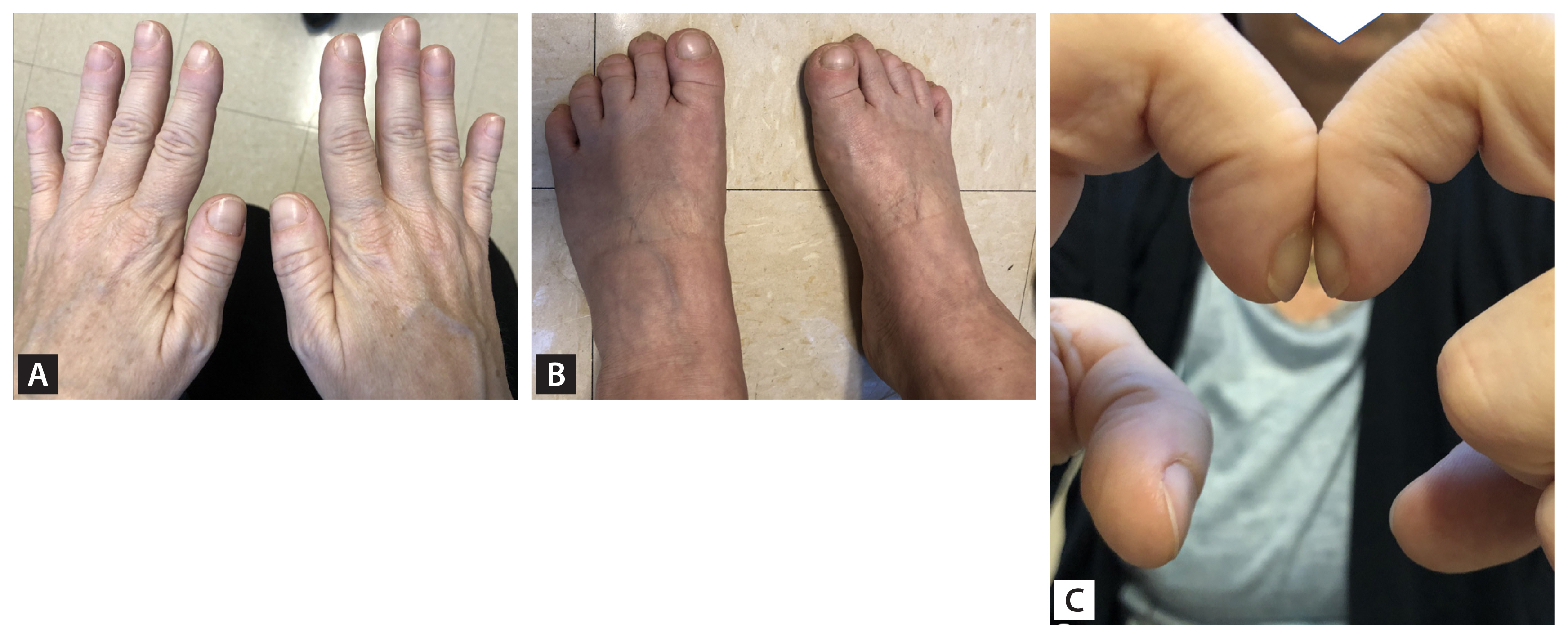
A 47-year-old female presented with joint swelling and arthralgias of bilateral hands and feet with fatigue and weight loss. Past medical history included melanoma 8 years ago with a negative sentinel lymph node biopsy. She had significant digital clubbing, confirmed with Schamroth window test (Fig. 1). X-rays revealed a large lung mass and periosteal reaction (Fig. 2). She was ultimately diagnosed with hypertrophic osteoarthropathy (HOA) due to metastatic melanoma.
Clubbing is important to identify because the differential diagnosis is actually quite limited. Clubbing can be benign and occur with no other findings; otherwise, it is associated with HOA. HOA is a syndrome caused by abnormal skin and osseous tissue proliferation of the extremities. It is diagnosed by digital clubbing, joint effusions, and periosteal reaction on imaging. In most cases, clubbing develops first and may be the only sign of HOA.
Primary HOA is typically hereditary, and accounts for 3% to 5% of HOA cases. Secondary HOA is most often associated with pulmonary etiologies (e.g., lung carcinoma, metastases, pulmonary infections, and chronic lung diseases). HOA is also associated with other intrathoracic causes (e.g., cyanotic heart disease, atrial myxomas, and infective endocarditis). Less commonly, HOA is associated with inflammatory bowel disease and cirrhosis. Localized HOA of one or two limbs can also occur.
Diagnosis of HOA relies on imaging of affected joints; there are no serologic tests. Plain radiographs typically demonstrate soft tissue changes associated with clubbing symmetric periosteal bone reaction in absence of fracture, and preserved joint spaces. If diagnostic uncertainty remains, bone scintigraphy with technetium 99m is more sensitive and the gold standard.
For primary HOA, there are no known treatments, and does not affect life expectancy. Secondary HOA requires further work-up for underlying cause which should include chest imaging, followed by directed treatment. Clubbing can resolve with treatment of underlying pathology.
Verbal informed consent was obtained from patient.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





