


INTRODUCTION
Obstructive sleep apnea (OSA) is characterized as a condition in which the upper airway repetitively collapses during sleep, completely or partially, resulting in frequent arousal and oxygen desaturation. According to previous reports, an estimated 425 million people aged 30 to 69 years have moderate to severe OSA, and up to 90% of OSA in the general adult population is misdiagnosed, and consequently untreated [1]. OSA is a growing health concern that has been related to a variety of comorbid conditions, including metabolic, cardiovascular (CV), renal, pulmonary, and neuropsychiatric disorders [2]. The lack of oxygen caused by OSA leads to increased health risks, such as CV disease, aortic aneurysm, high blood pressure, stroke, diabetes mellitus (DM), depressive illness, cognitive impairment, and even mortality, if not treated [3,4]. Given that undiagnosed OSA has major consequences in terms of public safety and all-cause mortality, focusing on the early detection and treatment of OSA is crucial.
Despite the crucial implications of untreated OSA, prompt diagnosis is often difficult. The gold standard for diagnosing OSA requires overnight polysomnography, which is time-consuming, expensive, and labor-intensive [5]. Furthermore, assessing OSA necessitates specialized personnel and equipment, which are rarely found in primary care clinics. As a result, to triage patients for early detection of OSA, a simple and reliable screening method is necessary. Several screening methods have previously been developed, and their efficacy has been validated. However, the limitations of these methods include the duration, complications associated with the method, and the requirement of upper airway evaluation [6,7].
The STOP-BANG questionnaire is an OSA screening tool that includes four self-reportable (STOP: snoring, weariness, witnessed apnea, and elevated blood pressure) and four demographic (BANG: body mass index [BMI], age, neck circumference, and gender) questions [8]. In the original validation trial, the STOP-BANG questionnaire with a score of ≥ 3 had a sensitivity of (84, 93, and 100) % for detecting mild, moderate, and severe OSA, respectively. The STOP-BANG questionnaire is frequently employed, given its high diagnostic accuracy, ease of use, and clear risk stratification criteria. However, BMI and neck circumference, two STOP-BANG questionnaire questions, are impacted by region-specific body features, which may alter the STOP-BANG questionnaire performance in different geographic locations [9].
The objective of this study was to investigate the prevalence of high-risk OSA as determined by the STOP-BANG questionnaire using nationwide data collected from the 2019 to 2020 Korean National Health and Nutrition Survey (KNHANES). We further intended to investigate the clinical features and comorbidities associated with high-risk OSA.
METHODS
Study population
We used data from the KNHANES, a nationwide population-based cross-sectional survey. This survey was conducted in eight phases: KNHANES phases I (1998), II (2001), III (2005), IV (2007–2009), V (2010–2012), VI (2013–2015), VII (2016–2018), and VIII (2019–2021). Data from KNHANES VIII–1 and VIII–2 (2019–2020) conducted by the Korea Centers for Disease Control and Prevention were assessed in this study. Written informed consent was obtained from all participants prior to survey administration. The present study was exempted from review by the Institutional Review Board of the Catholic University of Korea (VC22ZISI0106), because it employs deidentified and publicly available data.
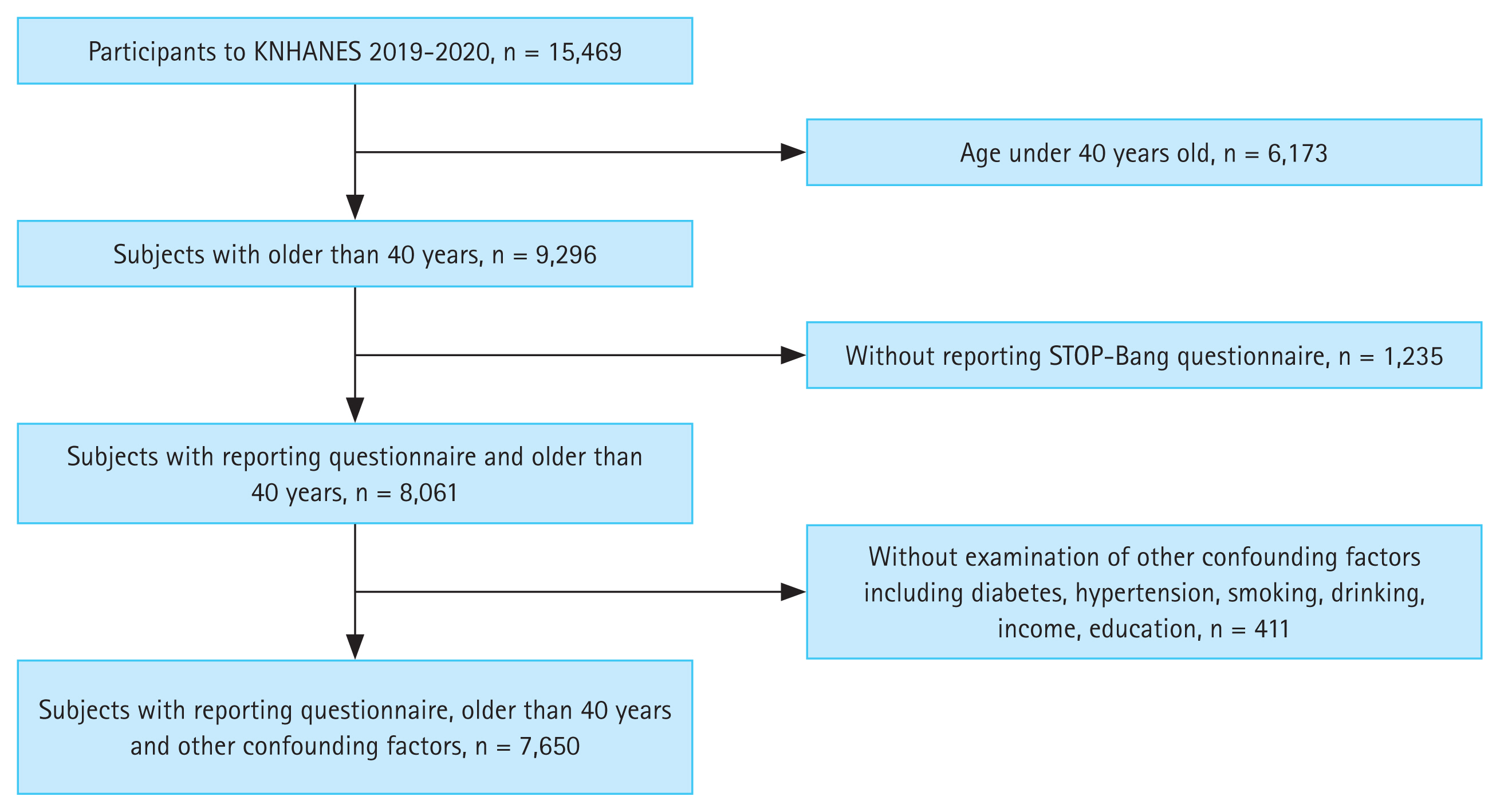
The KNHANES consists of several surveys about general health and nutritional status, health examinations, and laboratory investigations [10]. This survey used a stratified multistage probability sampling method to represent the Korean adult population, and the method considered geographic area, sex, and age group by referring to household registries. There were 15,469 participants from KNHANES VIII–1 and VIII–2. We excluded those under the age of 40 years (n = 6,173). Among them, 8,061 participants properly answered OSA-related questionnaires, such as the STOP-BANG questionnaire. We also excluded participants without information on other confounding factors, such as DM, hypertension, smoking, drinking, income, or education level. Finally, the data of 7,650 participants were included in the analysis (Fig. 1).
Survey for OSA
Patients aged ≥ 40 years were asked about the risk factors associated with OSA using the STOP-BANG questionnaire, which contains four questions and four objective measures with yes/no answers: (1) Snoring: Do you snore loudly (louder than talking or loud enough to be heard through closed doors)?; (2) Tired: Do you often feel tired, fatigued, or sleepy during daytime?; (3) Observed: Has anyone observed you stop breathing during your sleep?; (4) Pressure: Do you have or are you being treated for high blood pressure?; (5) BMI > 30 kg/m2; (6) Age > 50 years old; (7) Neck circumference > 36.3 cm; and (8) Gender (if male) [11]. The total sum of “yes” responses was counted.
Clinical and laboratory measurements
Anthropometric, socioeconomic, health-related variables, and biochemical measurements were included in the analysis. BMI was calculated as weight in kilograms divided by height in square meters. BMI was categorized into five groups: underweight (< 18.5 kg/m2), normal weight (≥ 18.5, < 23 kg/m2), overweight (≥ 23, < 25 kg/m2), obese (≥ 25, < 30 kg/m2), and severely obese (≥ 30 kg/m2) according to the World Health Organization guidelines for the Asian-Pacific region [12]. Obesity was defined as subjects with BMI ≥ 25 kg/m2. Waist circumference (WC) in the KNHANES was assessed by measuring at the midpoint between the lowest rib and the anterior iliac crest in the standing position. Abdominal obesity was defined as WC ≥ 90 cm in men, and ≥ 85 cm in women, according to the Korean Society for the Study of Obesity [13].
Socioeconomic variables included gender, age, household income, educational level occupation (employed or unemployed), and residency area (urban or rural). Educational attainment was classified as elementary school or less, middle school, high school, and college or more. Residence area was defined as urban residence when residing in Seoul, Gyeonggi-do, or five metropolitan cities in Korea. The information on household income was obtained through the questionnaire, and stratified into five groups for each quintile. Household income was calculated as an equivalent income by dividing monthly income into the square root of family size.
Health-related variables included smoking and alcohol drinking status, physical activity, fasting plasma glucose (FPG), renal function, and lipid profiles. Smoking status was classified into three groups: never smoker, former smoker, and current smoker. Former smokers were distinguished from current smokers based on their present smoking status. Subjects who ceased smoking at the time of the survey were considered former smokers, regardless of the duration of smoking cessation. Alcohol drinking status was classified into three groups: never, mild-to-moderate, and heavy drinkers, according to daily alcohol consumption at the time of the survey. Never drinker was defined as individuals consuming on < 1 occasion/month. Mild-to-moderate drinking was defined as individuals drinking < 30 g of alcohol/day. A heavy drinker was defined as an individual drinking ≥ 30 g of alcohol/day [14]. Physical activity was defined as performing moderate-intensity physical activity for at least 30 min/day at least 5 times/week or strenuous-intensity physical activity for at least 20 min/day at least 3 times/week [15].
For biochemical measurements, FPG and lipid profile levels were measured after overnight fasting using a Hitachi Autonomic Analyzer 7600-210 (Hitachi, Tokyo, Japan). Glycosylated hemoglobin (HbA1c) levels were measured by high-performance liquid chromatography on a Tosoh G8 device (Tosoh, Tokyo, Japan) [16]. The estimated glomerular filtration rate (eGFR) was calculated using the Modification of Renal Diet equation from baseline serum creatinine [17].
Primary outcome and assessment of covariates
The primary outcome was the prevalence of high risk of OSA, and OSA risk was assessed using the STOP-BANG score as follows: (1) high risk of OSA: yes to 5–8 items; (2) intermediate risk of OSA: yes to 3–4 items; and (3) low risk of OSA: yes to 0–2 items [18].
The presence of comorbidities was determined by asking respondents if they were ever diagnosed with, or treated for, the following conditions: DM, hypertension, hypercholesterolemia, or chronic kidney disease (CKD). The diagnosis of DM was indicated if any of the following were present: FPG ≥ 126 mg/dL, current use of antidiabetic medication, a previous history of DM, or HbA1c ≥ 6.5% [19]. Hypertension was diagnosed if any of the following were present: systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg, the current use of antihypertensive medications, or a self-reported physician diagnosis of hypertension [20]. Total cholesterol ≥ 240 mg/dL, or use of cholesterol-lowering medications, were all used to diagnose hypercholesterolemia [19]. CKD was defined as eGFR < 60 mL/min/1.73 m2 [17].
Statistical analysis
General characteristics are presented as percentages (standard errors [SE]), and as the means and SE for quantitative variables. To perform group comparisons, the Rao-Scott chi-square test and analysis of variance (ANOVA) were used for categorical and continuous data, respectively. Both univariate and multiple logistic regression analyses were used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for evaluating factors associated with the OSA high-risk group (STOP-BANG score 5–8). In addition to the unadjusted model, the following confounding factors were considered in the multivariable regression model: age and sex for model 2; and age, sex, education level, household income quintile, smoking status, alcohol consumption, physical activity, DM, hypertension, hypercholesterolemia, CKD, obesity, and abdominal obesity for model 3. All statistical analyses were conducted using SAS version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA). The p values provided are two-sided, with a level of significance of 0.05.
RESULTS
Clinical characteristics according to STOP-BANG score category
Table 1 demonstrates the clinical characteristics of the study population according to the STOP-BANG score category. Among 7,650 total individuals, 919 subjects (12.0%) had a high risk of OSA (score 5–8). Compared to the intermediate- or low-risk group, the high-risk OSA group showed higher proportions of men, greater BMI, increased rates of smoking, heavy alcohol consumption, and abdominal obesity, and a higher proportion of employed responders. Regarding health-related factors, the high-risk OSA group had higher FPG, blood pressure, and triglyceride levels, and lower total cholesterol, high-density lipoprotein cholesterol, and eGFR levels. The high-risk STOP-BANG score group showed a significantly higher comorbidity prevalence. In the high-risk group, 67.1% had abdominal obesity, 32.7% DM, 73.3% hypertension, and 66.1% obesity, which was significantly higher, compared to the intermediate and low risk group. The clinical characteristics for males and females were both similar to the general population when they were analyzed separately (Supplementary Table 1).
In the STOP questionnaire, the prevalence of each item decreased in the following order: hypertension (38.0%), tired feeling (30.9%), snoring (20.3%), and observed stopping breathing during sleep (10.0%) (Table 2). In the BANG questionnaire, the prevalence of each item decreased in the following order: age > 50 years (69.6 %), male sex (48.5 %), neck circumference > 36.6 cm (41.9 %), and BMI > 30 kg/m2 (5.3 %).
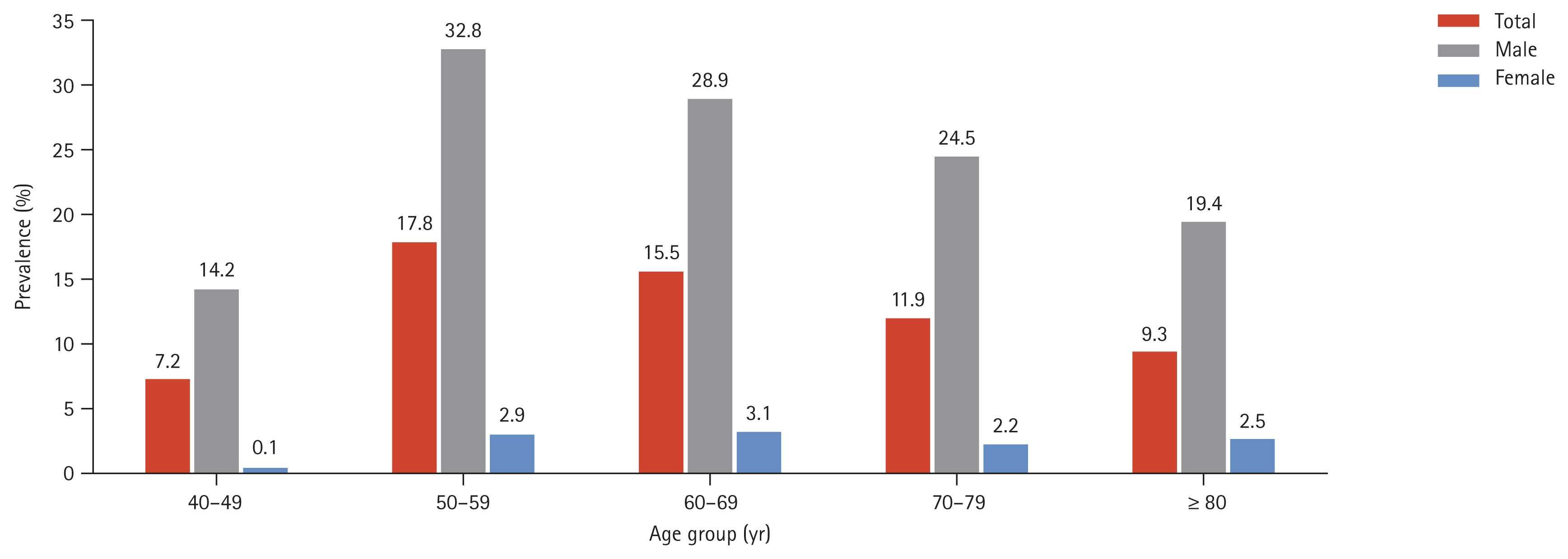
Fig. 2 shows trends in the prevalence of a high risk of OSA categorized by the STOP-BANG scoring system by age and sex groups. When classified according to age group, the prevalence of high risk of OSA was highest in patients in their 50s (17.8%) and 60s (15.5%), and lowest in the patients in their 40s (7.2%) in the total (p for trend < 0.001) and male populations (p for trend < 0.001). However, in the female group, the prevalence of a high risk of OSA was highest in the patients in their 60s (3.1%) and 50s (2.9%), and lowest in those in their 40s (0.1%) (p for trend < 0.001). The prevalence was increased approximately 10-fold in males compared with females across all age categories.
Combined comorbidities and high risk of OSA
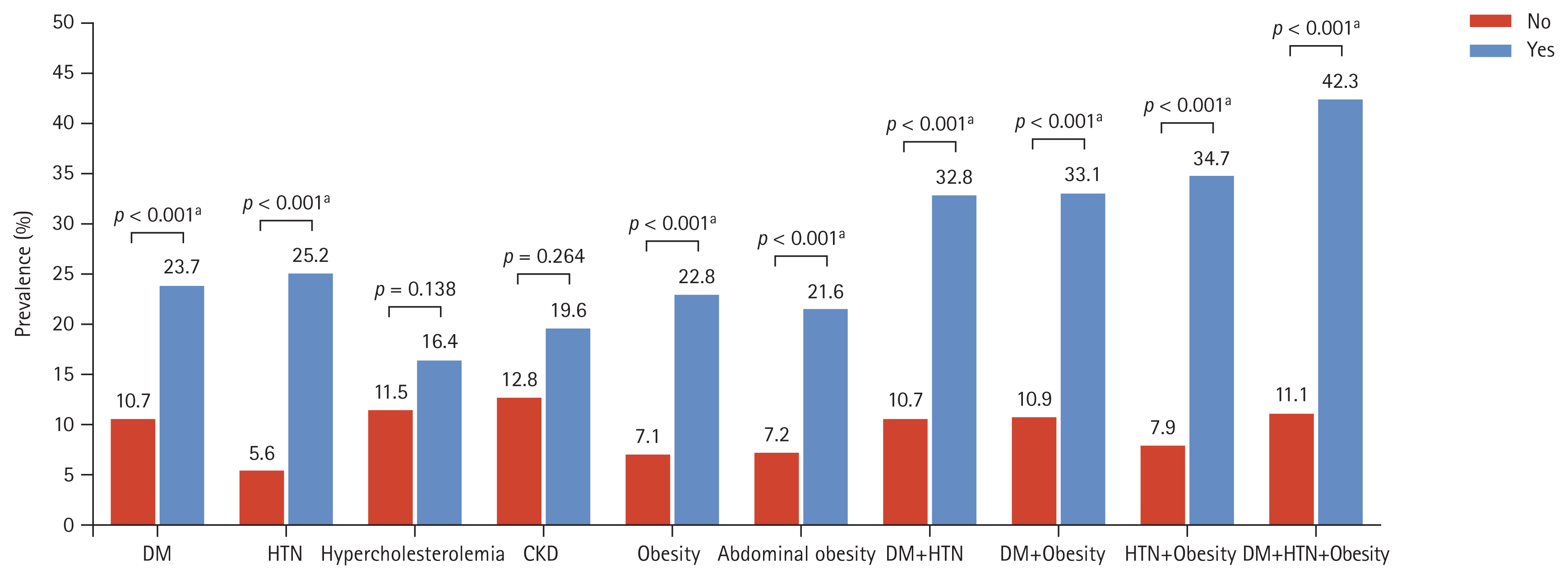
Those with high-risk OSA showed significantly higher proportions of individuals with comorbidities (DM, hypertension, hypercholesterolemia, CKD, obesity, and abdominal obesity) than the low- or intermediate-risk group (p < 0.001 for all, except for CKD, p = 0.264) (Fig. 3). In particular, if the subjects had DM, hypertension, and obesity at the same time, the prevalence of high risk in the OSA population increased up to approximately four times, compared to those who did not have any of the comorbidities (42.3% vs. 11.1%, p < 0.001). The association was also apparent when the prevalence of high-risk OSA was obtained based on the measures of hypertension, diabetes, and obesity according to decile group (Supplementary Table 2). The prevalence tended to increase with higher measures of systolic/diastolic blood pressure, FPG, HbA1c, BMI, and WC.
In multivariable logistic regression analysis, the high risk of OSA was significantly associated with increasing age (OR, 1.01; 95% CI, 1.00 to 1.02), males (OR, 13.24; 95% CI, 9.34 to 18.77), and higher education (OR, 1.93; 95% CI, 1.34 to 2.77), after adjusting for multiple demographic, biochemical, and comorbidity confounders (Table 3). However, no association was noted between household income status, employment, smoking, alcohol consumption status, or physical activity, and higher STOP-BANG scores. The presence of comorbidities, such as DM (OR, 1.57; 95% CI, 1.25 to 1.97), hypertension (OR, 4.81; 95% CI, 3.88 to 5.97), obesity (OR, 2.02; 95% CI, 1.60 to 2.56), and abdominal obesity (OR, 1.61; 95% CI, 1.28 to 2.02) were significantly associated with a high risk of OSA. Participants who had DM, hypertension, and obesity altogether had almost 4-fold high risk of OSA, compared to those with no comorbidities (OR, 3.88; 95% CI, 2.94 to 5.11). In terms of gender, the high risk of OSA was significantly associated with age, education level, and abdominal obesity only in males. In contrast, DM, hypertension, and obesity were all associated with the high risk of OSA in both males and females (Supplementary Table 3).
DISCUSSION
In this recently investigated, large nationwide cross-sectional study, we found that comorbidities, such as DM, hypertension, and obesity, were significantly associated with a high risk of OSA, based on the STOP-BANG questionnaire in a Korean adult population. Notably, these three comorbidities had a synergistic impact in elevating OSA risk. The STOP-BANG scoring questionnaire was first introduced in the KNHANES VIII in 2019. Hence, this is the first nationwide study on the association of chronic metabolic disease with a high risk of OSA in the representative Korean population utilizing the STOP-BANG questionnaire. According to the results of our study, screening for OSA should be more actively recommended for patients with DM, hypertension, and obesity, particularly males.
The STOP-BANG questionnaire is well recognized as a reliable OSA screening tool that is both simple and self-reportable [8]. The validity of this method is evidenced in several prior systemic reviews. A recent meta-analysis confirmed that the STOP-BANG questionnaire can be used as a screening tool to help triage individuals with suspected OSA [9]. Another previous meta-analysis validated the strong performance of the STOP-BANG questionnaire for OSA screening [21]. The correlation between STOP-BANG scores and the probability and severity of OSA is also well indicated. A STOP-BANG score of (5–8) indicated individuals with a high chance of moderate/severe OSA in recent prospective research using a surgical population [18]. Another previous study also classified patients with a STOP-BANG score of (0–2) as low risk for moderate to severe OSA, whereas those with a score of (5–8) were classified as high risk for moderate to severe OSA [22]. This classification was utilized in our study to evaluate clinical features according to the severity of OSA.
Several studies employing the STOP-BANG questionnaire, including the Asian population, have been reported. According to earlier systematic reviews, the prevalence of moderate-to-severe OSA was 21.3%, whereas that of severe OSA was 7.8% [23]. In a study of the Singapore population, the prevalence of moderate-to-severe OSA was 28.1%, and that of severe OSA was 10.7% [24]. Other questionnaire-based studies reported that the prevalence of high-risk OSA ranged (12.4 to 15.8) % in the Korean adult population; however, those studies of the Korean population utilized the Berlin questionnaire [25,26]. Altogether, the results of our study seem to be consistent with previous data regarding the adult population.
Our study presents a remarkably higher prevalence of high-risk OSA in males, compared with females. The male predominance in high-risk OSA was frequently presented in previous epidemiologic studies, and male sex is a widely accepted risk factor for OSA [27]. The 10-fold predominance of high-risk OSA in males correlates with an old renowned study conducted in 1979 [28]. However, recent studies show a rather mild male predominance, compared to our study [26]. This discrepancy may be explained by a more recent study that indicated an unacceptably low sensitivity of the STOP-BANG questionnaire in females, compared to males [29]. Due to the bias toward males, sex-specific cutoffs for STOP-BANG should be carefully investigated. Although the predominance of male in high-risk OSA is apparent in our study, the clinical characteristics among males and females were not largely different, and the tendency was comparable to the general population.
Our study also presents that socioeconomic factors, such as education level, household income, region of residence, and occupation status, were associated with high risk of OSA. The hypothesis that lower socioeconomic status is linked to poor sleep quality and increased prevalence of OSA is supported by various research [30,31], and a significant higher risk for OSA was observed in association with less education and lower economic income [32]. Common comprehensive measures of socioeconomic status include household income, location of residence, occupation status, and basic education or education-derived variables [25]. Although there is no conclusive evidence on the relationship between socioeconomic status and the risk of OSA, it is widely accepted that socioeconomic status has an impact on a range of health practices, biomarkers, and chronic diseases [30]. Therefore, our results support the notion that composite indicators of socioeconomic status, such as household income, area of residence, occupation status, and education attainment, are associated with the risk of OSA.
The most significant finding of our study is the association of a higher STOP-BANG score with a higher comorbidity prevalence, as well as a synergistic effect, when all three comorbidities are present. According to our results, hypertension, DM, and obesity were significantly associated with high-risk OSA, and the prevalence of high-risk OSA consistently increased with higher measures of hypertension, DM, and obesity. OSA has long been understood to play a role in CV disorders, particularly hypertension, heart failure, and stroke [3]. OSA is further exacerbated by an increase in body weight. According to studies, gaining 10% of one’s body weight increases the risk of OSA by six times [33]. Obesity-related fat deposition in the neck can obstruct the pharyngeal lumen, causing it to collapse when sleeping [34]. OSA is also known to cause arterial stiffness, which can lead to a CV disorder, and OSA therapy can help to reduce arterial stiffness [35]. Furthermore, sleep breathing disorders may increase the risk of DM through affecting plasma insulin levels and glycemia [36]. Thus, it is possible to deduce that OSA and comorbidities, such as hypertension, DM, and obesity, interact, and have an impact on one another. According to our results, OSA should be screened and detected early in patients with DM, hypertension, or obesity, especially if all three are present. The health impact of OSA in certain chronic metabolic illnesses could be decreased by using this validated short questionnaire, and the importance of lifestyle modification and active treatment of coexisting diseases should be emphasized for those individuals.
Our study has several limitations. First, the subjects were not clinically confirmed to have OSA using polysomnography. The risk stratification was exclusively based on the participant’s self-reporting questionnaire. The fact that our study’s prevalence of high-risk OSA was comparable to that of prior population-based studies implies that our sampling approach was rather reliable. Second, given that our sample excluded patients aged less than 40 years, the biased sample may have affected the true clinical significance of our data. However, previous data show that utilization of health care is only substantial in OSA patients over the age of 40 years, which supports the KHANES policy of only administering the STOP-BANG questionnaire to those over the age of 40 years [37,38]. As a result, in terms of social welfare, populations above the age of 40 years should be prioritized for the early identification of OSA. Finally, this study was inevitably performed with a cross-sectional design, given the retrospective analysis of the established dataset. Thus, causal associations between high-risk OSA and other comorbidities, or the use of antihyperglycemic, antihyperlipidemic, and antihypertensive medications, cannot be completely clarified. However, this research has advantages in retrieving data from a nationally representative survey sample with a high response rate; therefore, a large amount of data was provided to overcome potential confounding issues. Furthermore, our data were obtained from a large sample, which improved the precision of our findings, and allowed for numerous statistical adjustments. This study is the first to report the prevalence of high-risk groups of OSA based on the STOP-BANG questionnaire in a Korean population, and provides the clinical implication of a high-risk OSA group.
In conclusion, we present for the first time that based on the STOP-BANG questionnaire, the prevalence of high-risk OSA groups in the general Korean population was 12.0%. OSA must be screened and detected early in patients with DM, hypertension, and obesity. The health burden of OSA in chronic metabolic disease could be reduced using this simple and validated short questionnaire. In the future, the exact prevalence of OSA needs to be diagnosed by a confirmed method in this high-risk group of OSA in the Korean population.
KEY MESSAGE
1. The STOP-BANG questionnaire revealed that the prevalence of a high risk of obstructive sleep apnea (OSA) was 12.0% in the Korean population over age 40 years.
2.A high risk of OSA was associated with socioeconomic (older age, male gender, current smoker, heavy alcohol drinker) and chronic metabolic disease, particularly in those with diabetes mellitus, hypertension, or obesity.
3. Active OSA screening, prevention, and management may improve health outcomes related to OSA in patients with diabetes mellitus, hypertension, or obesity.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





