


INTRODUCTION
Hypertrophic cardiomyopathy (HCM) is an autosomal dominant hereditary cardiomyopathy characterized by left ventricular (LV) hypertrophy not attributable to loading conditions, such as hypertension, valvular heart disease, or congenital heart disease [1]. HCM is closely related to sudden cardiac death (SCD) and malignant ventricular tachyarrhythmias due to myocyte and myofibrillar disarray and interstitial fibrosis [2,3].
The use of primary prevention implantable cardioverter-defibrillators (ICDs) in HCM patients at high-risk of SCD was introduced more than 20 years ago and was shown to provide absolute protection by terminating lethal tachyarrhythmia events [4]. Risk stratification and the subsequent use of ICDs in clinical practice have substantially reduced disease-related mortality [5,6]. A risk assessment for SCD is recommended for all HCM patients to identify those who will benefit from ICD implantation. However, decision-making regarding ICD implantation in HCM patients as a primary prevention measure can be challenging considering the low SCD event rate versus the risk of device-related complications [7]. While in some patients ICD implantation is potentially life-saving [8], a substantial proportion of ICD recipients experience implant-related complications, such as those related to inappropriate ICD therapy, lead dysfunction, infection, bleeding, and thrombosis [9ŌĆō11]. For younger patients with HCM who are candidates for primary prevention ICD implantation, the risk period associated with treatment may extend over a period of years or even decades. Therefore, SCD risk assessments and the indications for primary prevention ICD implantation in patients with HCM continue to evolve, as, despite international guidelines, a consensus has yet to be reached.
In the following, we review recent guidelines and published data on the risk factors that contribute to SCD in HCM. We then discuss the risk assessments and updated indications for ICD implantation in this population.
REVIEW OF RECENTLY UPDATED GUIDELINES REGARDING RISK STRATIFICATION AND ICD IMPLANTATION
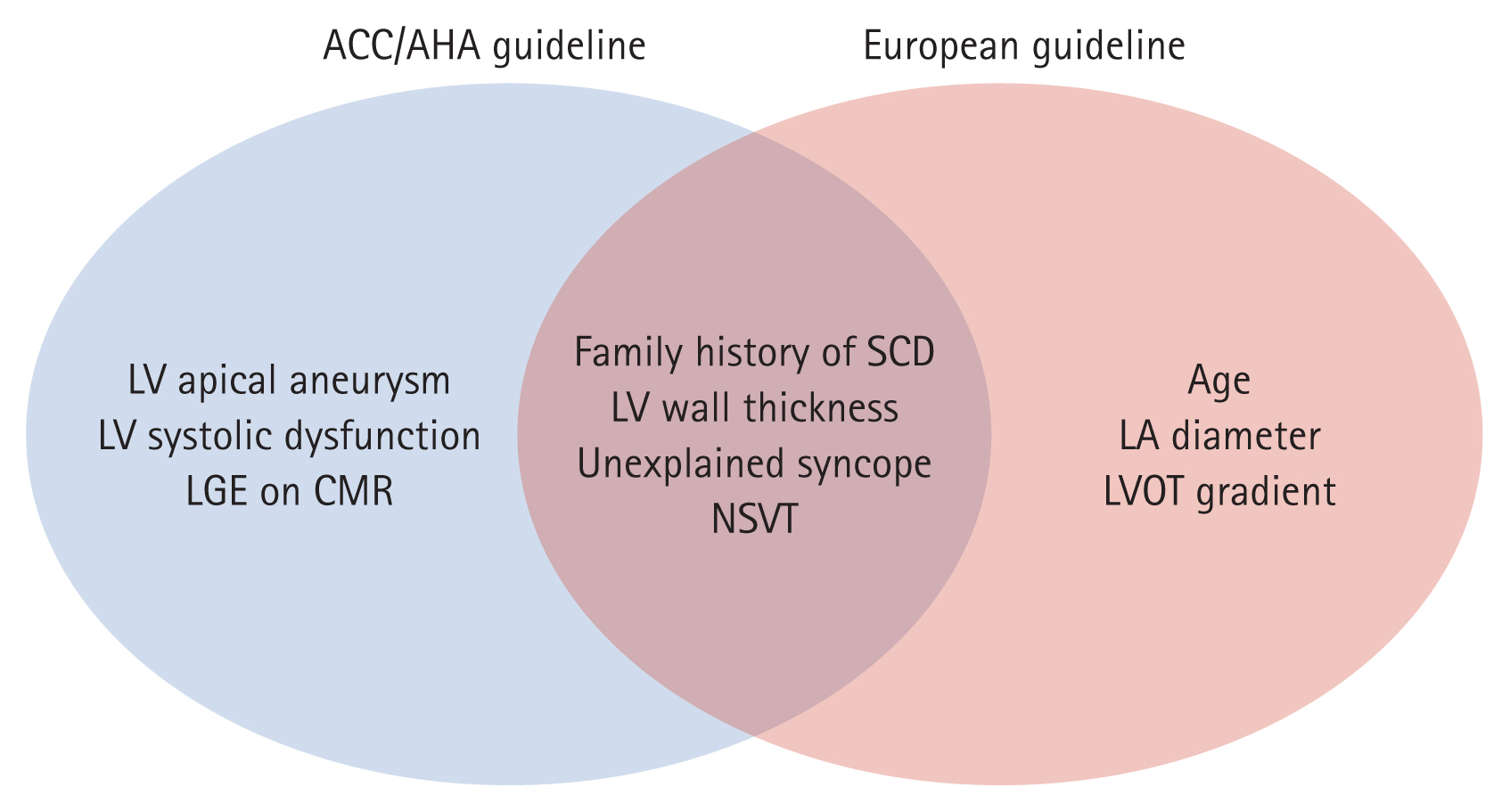
The American College of Cardiology (ACC)/American Heart Association (AHA) and the European Society of Cardiology (ESC) have each published major guidelines for ICD implantation [12,13]. The two guidelines are in agreement regarding the class I indications for secondary prevention ICD implantation in patients with HCM (i.e., patients with HCM who have suffered a previously documented cardiac arrest or hemodynamically significant ventricular tachyarrhythmias). This recommendation is based on the observation that patients with HCM who survive malignant ventricular tachyarrhythmias are at high-risk of recurrent SCD due to subsequent lethal arrhythmic events. However, disagreement persists regarding ICD implantation as a primary prevention measure (Fig. 1).
2020 ACC/AHA GUIDELINES
Current ACC/AHA guidelines, most recently updated in 2020, suggest the use of several non-invasive SCD risk markers to estimate the risk level, including familial history of SCD from HCM, massive LV hypertrophy, unexplained syncope, LV dysfunction or LV apical aneurysm, extensive late gadolinium enhancement (LGE) on cardiac magnetic resonance (CMR) imaging, and non-sustained ventricular tachycardia (VT) on ambulatory monitoring. One or more of the recognized risk markers in HCM is considered relevant and major within the overall clinical profile of a clinically diagnosed patient and thus sufficient for the consideration of primary prevention ICD implantation.
In adult HCM patients, the major risk factors for SCD include: (1) sudden death judged to have been definitively or likely attributable to HCM in Ōēź 1 first-degree or close relative at the age of Ōēż 50 years; (2) massive LV hypertrophy Ōēź 30 mm in any LV segment; (3) Ōēź 1 recent episode of syncope in the previous 6 months that is suspected to be arrhythmic in origin according to the clinical history (i.e., unlikely to be neurocardiogenic [vasovagal] or related to LV outflow tract obstruction [LVOTO]); (4) the presence of a LV apical aneurysm independent of its size; and (5) decreased LV systolic function (ejection fraction [EF] < 50%). These patients are eligible for ICD implantation (class IIa). In adult HCM patients who lack major SCD risk factors, ICD may be considered in those with extensive LGE on contrast-enhanced CMR imaging or non-sustained VT during ambulatory monitoring (class IIb). Greater weight is assigned when the non-sustained VT runs are repetitive (Ōēź 3 episodes), longer (Ōēź 10 beats), and faster (Ōēź 200 bpm), usually occurring over 24 to 48 hours of extended ambulatory electrocardiogram (ECG) monitoring. The significance of short, single bursts of non-sustained VT in predicting ICD-treated VT or ventricular fibrillation (VF) is less certain in the absence of other major risk factors [14]. A risk assessment strategy based on major risk markers and using ACC/AHA guidelines is most appropriate in young and middle-aged patients with HCM, considering the very low event rate of SCD in older (> 60 years) HCM patients [3,5,6].
The 2020 AHA/ACC risk assessment methodology for SCD in HCM patients was validated in a Chinese HCM cohort. The risk assessment for SCD according to the 2020 AHA/ACC guidelines showed better discrimination (greater area under the curve, 0.71; 95% confidence interval [CI], 0.56 to 0.87; p < 0.001) than either the 2011 American College of Cardiology Foundation (ACCF)/AHA guidelines (0.52; 95% CI, 0.37 to 0.67; p = 0.76) or the 2014 ESC guidelines (0.68; 95% CI, 0.54 to 0.81; p = 0.02) [15].
2014 ESC GUIDELINES
ESC guidelines suggest the use of an individualized estimated 5-year SCD risk assessment model that incorporates several disease-related risk factors into a logistic regression equation [13]. This model was created based on a cohort of 3,675 individuals from six centers [16]. The parameters of the risk calculator include: (1) maximal LV wall thickness; (2) left atrial (LA) diameter; (3) maximal LV outflow tract (LVOT) gradient; (4) family history of SCD; (5) non-sustained VT; (6) unexplained syncope; and (7) age at clinical evaluation.
The resulting HCM Risk-SCD formula is as follows: probability of SCD at 5 years = 1 ŌĆō 0.998exp (prognostic index), where the prognostic index = [0.15939858 ├Ś maximal wall thickness (mm)] ŌĆō [0.00294271 ├Ś maximal wall thickness2 (mm2)] + [0.0259082 ├Ś LA diameter (mm)] + [0.00446131 ├Ś maximal (rest/Valsalva) LVOT gradient (mmHg)] + [0.4583082 ├Ś family history SCD] + [0.82639195 ├Ś non-sustained VT] + [0.71650361 ├Ś unexplained syncope] ŌĆō [0.01799934 ├Ś age at clinical evaluation (years)] [13]. This model includes LA diameter and LVOT gradient as risk factors, with the model for these factors including LV wall thickness as a continuous rather than a dichotomous variable. However, the calculated risk for SCD fails in patients with severe LV hypertrophy (Ōēź 35 mm) because the relationship between maximum LV wall thickness and risk is nonlinear. The HCM Risk-SCD should thus be used with caution in patients with severe LV hypertrophy (Ōēź 35 mm) given the limited available data [17]. In addition, the HCM Risk-SCD estimate does not consider the impact of recently evaluated newer markers, such as apical aneurysm, decreased LV systolic function (LVEF < 50%), and the presence of LGE.
The HCM Risk-SCD model predicts the 5-year probability of SCD based on clinical risk factors and weights unique to overall risk. In the published HCM Risk-SCD dataset, three risk categories (high, intermediate, and low) for SCD were determined by consensus. For every 16 ICDs implanted in patients with a 5-year SCD risk Ōēź 4%, potentially one patient will be rescued from SCD at 5 years [16]. Therefore, ICD implantation should be considered in high-risk patients with an estimated 5-year risk of SCD Ōēź 6% and it can be considered in intermediate-risk patients with an estimated 5-year risk of Ōēź 4% to < 6% according to the 2014 ESC guidelines [18].
This HCM Risk-SCD model was validated in a Korean HCM population of 730 patients. The primary endpoint, defined as a composite of appropriate ICD intervention and SCD, developed in 1.1% (7/615) of the low-risk group, 4.6% (3/65) of the intermediate-risk group, and 12.0% (6/50) of the high-risk group. The model had a high negative predictive value and high accuracy for predicting appropriate ICD intervention or SCD but a relatively low sensitivity [19].
The HCM Risk-SCD calculator has a relatively high negative predictive value, suggesting that it reduces the number of ICD implants in low-risk patients and possibly limits ICD overuse in those patients. This HCM Risk-SCD model may help individuals by quantifying their SCD risk during shared decision-making with the treating physician.
POTENTIAL PROGNOSTIC FACTORS
The aim of SCD risk assessment in patients with HCM is to identify those who would benefit from ICD implantation, as ICD implantation in high-risk patients significantly reduces the rates of SCD and HCM-related mortality. However, in some patients, although traditional risk factors are absent, the risk of SCD is nonetheless significant [5,20,21], which has led to a search for additional risk markers to improve current risk models and aid in clinical decision-making. The investigated risk factors that have raised interest are shown in Table 1.
T1 MAPPING AND ENTROPY ON CMR IN THE EVALUATION OF FIBROSIS
Focal myocardial fibrosis can be quantified by LGE, based on comparisons between normal myocardium and regions of focal myocardial damage. Diffuse fibrosis is not well detected by standard LGE-CMR protocols but it can be seen using post-contrast T1 mapping, a recently developed method. A prolonged myocardial T1 with elevated extracellular volume in patients with HCM suggests diffuse myocardial fibrosis, even in the absence of regionally definite LGE and hemodynamic LVOTO [22]. In adult patients with HCM, diffuse fibrosis is a predictor of non-sustained VT and aborted SCD [23]. A computational modeling approach that merges data from LGE-CMR with that from post-contrast T1 mapping is able to reveal extensive diffuse fibrotic remodeling, which is a risk factor for SCD and ventricular tachyarrhythmia in HCM and is associated with the occurrence of new ventricular tachyarrhythmias [24].
Entropy measures the uncertainty of tissue composition as reflected by the uncertainty of signal intensity and it is computed from all signal intensity values in LGE-CMR. Recently, the measurement of entropy was applied to evaluate heterogeneity in fibrotic lesions [25,26]. Scar heterogeneity, which is quantified by determining the entropy within a scar, and LGE extent were shown to be independent risk indicators of ventricular arrhythmias [26].
GENETIC FACTORS
Genetic testing in HCM patients has developed rapidly and is now widely used; however, recent guidelines do not include specific recommendations for its clinical application to SCD risk stratification. Thus far, there is little evidence supporting the use of genetic testing to identify HCM patients at high-risk of SCD.
A meta-analysis of 7,675 patients with HCM determined a 0.4% rate of SCD in those with mutation-negative HCM and risks of 5%, 11%, and 17% for those with myosin-binding protein C (MYBPC3), beta-myosin heavy chain (MYH7), and cardiac troponin T (TNNT2) mutations, respectively [27]. Although HCM caused by mutations in thin myofilament proteins, such as TNNT2, results in less hypertrophy, they increase the risk of systolic LV dysfunction [28]. TNNT2 gene mutations can lead to severe myocyte disarray and a high incidence of SCD in younger patients without LV hypertrophy or with only mild LV wall thickness and low HCM penetrance [29ŌĆō32]. The incidence of SCD is significantly higher in mutation-positive than mutation-negative patients [27]. However, studies have shown that, in HCM, a single mutation in genes encoding proteins of the cardiac sarcomere does not predict SCD or appropriate ICD intervention due to ventricular tachyarrhythmias [10,28]. Patients with multiple mutations demonstrate earlier disease onset and more severe disease progression [33], and those with double or triple mutations are at higher risk of end-stage disease progression and ventricular tachyarrhythmias [34]. In this subset of patients, serious disease progression may contribute to SCD even in the absence of traditional risk factors [35]. MYBPC3 gene mutation also revealed multiple loci associated with SCD in HCM despite MYBPC3 usually developing at later age and having a favorable disease progression [36]. Additional research is needed to determine the extent to which multiple mutations are an additional risk factor for SCD in HCM.
The recommendations based on recent guidelines for genetic testing apply only to screening for HCM and do not support risk assessment and decision-making regarding ICD implantation [13,37]. Therefore, clinical decisions regarding ICD in the primary prevention of SCD should not be made on the basis of genetic testing until further evidence is available.
CARDIOPULMONARY EXERCISE TESTING
A recent prospective study of 623 HCM patients (median follow-up, 3.7 years; 25 events) identified a ventilation versus carbon dioxide correlation during exercise (VE/VCO2 slope) as an independent predictor of SCD, with a best accuracy of > 31 for predicting the SCD endpoint compared using 2011 ACCF/AHA or 2014 ESC guideline algorithms [38]. In an analysis of 63 patients who had a hard endpoint of appropriate ICD intervention or death among 1,005 HCM patients, the factors that remained significant in a stepwise multivariable analysis were the percentage of age- or sex-predicted peak oxygen consumption (VO2), normal recovery of heart rate at 1 minute, absence of atrial fibrillation (AF), and surgical relief of LVOTO [39]. In a recent meta-analysis of 11,672 patients with HCM, the mean maximal oxygen consumption (VO2max) was significantly lower in patients with combined cardiovascular death than in those who survived (ŌłÆ6.20 mL/ kg/min; 95% CI, ŌłÆ7.95 to ŌłÆ4.46; p < 0.01). A lower VO2max is consistently observed in HCM patients at risk of major cardiovascular outcomes. VO2max is the most common performance measure in functional studies, with higher values reached in patients on cycle-ergometers than on a treadmill [40]. However, the cardiopulmonary functional assessment of patients with HCM requires protocol standardization.
The HYPertrophic Exercise-derived Risk score for heart failure (HyperHF), which includes both cardiopulmonary exercise testing and echocardiographic parameters, was proposed as a valuable predictor of SCD-related events [41]. A novel HyperHF score using the LA volume index had better predictive power for a composite of SCD- and stroke-related events [42].
ATRIAL FIBRILLATION
Impaired LV diastolic function is one of the mechanisms for progressive LA enlargement and the subsequent development of AF [43,44]. AF can be a marker of advanced disease, representing electroanatomical remodeling. We previously reported the case of an HCM patient with AF but without traditional risk factors who developed VF and SCD [21]. In another study, the presence of AF, particularly new-onset AF, was shown to be significantly related to an increased incidence of HCM-related events, including those that were SCD-relevant [45]. Incident AF was linked to an increased risk of both SCD- and non-SCD-relevant events [46]. The early detection and treatment of AF may lead to a more comprehensive risk assessment of SCD in patients with HCM.
ELECTROCARDIOGRAPHY PARAMETERS
The T wave amplitude on surface ECG, which is one of the repolarization parameters in lead V2, is an independent predictor of SCD risk. T wave amplitude may be of incremental predictive value in the establishment of risk factors [47]. A myocardial infarction pattern consisting of pseudo-ST-segment elevation, a QRS duration Ōēź 120 ms, and low QRS voltage were independent predictors of SCD or its surrogates, including appropriate ICD intervention and resuscitated cardiac arrest [48]. Both QRS fragmentation in Ōēź 3 territories and a heart rate corrected QT (QTc) duration Ōēź 460 ms were associated with ventricular tachyarrhythmia and SCD in HCM patients, independent of and incremental to traditional SCD risk factors [49].
Ventricular repolarization parameters, such as the interval between the peak and the end of the electrocardiographic T wave (Tpe)/QTc ratio and Tpe interval, were remarkably higher and longer in HCM patients than in controls. In a multivariate analysis, they were also significantly related to a higher risk of ventricular tachyarrhythmias [50,51].
The negativity of the electromechanical window, defined as the interval between the Q wave and aortic valve closure minus the QT interval, is an independent risk factor for life-threatening arrhythmic events [52].
LV GLOBAL LONGITUDINAL STRAIN
The global longitudinal strain (GLS) is a more sensitive sign of LV systolic dysfunction than LVEF and is decreased in patients with HCM, even in those with early-stage disease and a preserved LVEF [53]. LV-GLS is significantly related to an increased risk of SCD events [54] and is an independent predictor of appropriate ICD therapy [55]. CMR-feature tracking derived GLS is also a strong independent predictor of major adverse cardiac events, including hospitalization for heart failure, resuscitated cardiac arrest due to ventricular tachyarrhythmias, and SCD [56].
BIOMARKERS
Brain natriuretic peptide (BNP) is associated with both VO2 and the percent predicted VO2 achieved during cardiopulmonary exercise testing [57]. An increased BNP level was reported to be associated with SCD or the combination of malignant ventricular tachyarrhythmias and SCD [58]. The BNP level is also an independent predictor of morbidity and mortality in patients with HCM [57]. N-terminal pro-brain natriuretic peptide (NT-proBNP) is an independent predictor of SCD, and in HCM patients it correlates significantly with cardiac fibrosis as detected by LGE or by MassonŌĆÖs trichrome staining of the myocardium [59].
CONCLUSIONS
In HCM, the cardiovascular event rate is low and the clinical presentation highly heterogeneous. The overlapping international guideline criteria for primary prevention ICD implantation provide imperfect support in SCD discrimination, and current risk stratification strategies are limited. However, substantial complications occur after device therapy, such as inappropriate ICD therapy and other procedure-related events, thus highlighting the importance of carefully selecting patients for whom the benefits of ICD implantation outweigh the risks. Nonetheless, in the light of continued research the evaluation of SCD is evolving. In this review, we examined updated guidelines and potential prognostic factors related to SCD. According to current guidelines, ICD implantation is highly recommended in HCM patients at high-risk of SCD. Shared decision-making with patients and treatment individualization according to risk factors prior to ICD implantation are necessary, especially in patients at intermediate-risk. A periodic reassessment of the SCD risk is an integral component of the longitudinal evaluation of most patients with HCM, considering that the risk increases over many decades. A more precise and more sensitive risk assessment can be obtained by incorporating current guidelines and based on a comprehensive evaluation of other potential risk factors, beyond those in the guidelines, in individuals at intermediate-risk.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





