


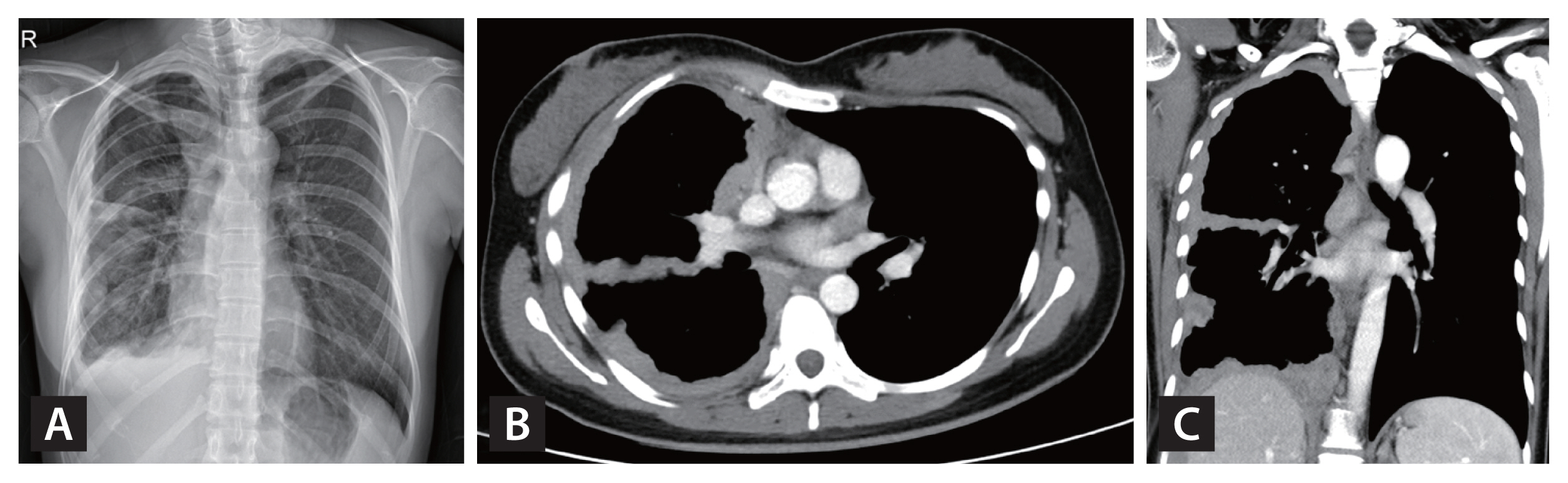
A 26-year-old woman presented to our hospital f or radiologically abnormal pleural lesions at a health check-up. She was asymptomatic with normal laboratory findings. A chest X-ray showed diffuse nodular pleural thickening in the right hemithorax (Fig. 1A). On computed tomography (CT), the extensive pleural thickening involved interlobar fissures and the diaphragmatic pleura, combined with multiple lymphadenopathies in the mediastinum and the anterior diaphragmatic area (Fig. 1B and 1C). These lesions had increased 18F-fluorodeoxyglucose (FDG) uptake on positron emission tomography-computed tomography (PET-CT) (Fig. 2AŌĆō2C), suggesting pleural malignancy such as mesothelioma. Chest magnetic resonance imaging (MRI) with enhancement revealed that the pleural lesions showed moderate enhancement after contrast infusion and diffusion restriction on diffusion-weighted images (Fig. 2D and 2E). For a definite diagnosis, video-assisted thoracoscopic pleural biopsy was done. The lesion had chronic granulomatous inflammation with multi-nucleated giant cells with a negative PCR result for Mycobacterium tuberculosis/ non-tuberculous mycobacterium and a few acid-fast bacilli in Ziehl-Neelsen stain. Finally, M. tuberculosis was cultured in bronchial specimens.
The common manifestation of pleural tuberculosis (TB) is unilateral effusion with corresponding symptoms such as cough or chest discomfort. Pleural thickening or fibrothorax usually develops in progression or as a sequelae of TB effusion. The fact that our patient had no symptoms and the peculiar chest lesions of nodular and circumferential pleural thickening without effusion involving the mediastinal pleura and interlobar fissures on CT pointed to pleural malignancy rather than pleural TB. Diffusion restriction on chest MRI and increased FDG uptake on PET-CT further supported malignant disease in this case. After standard anti-TB treatment, the pleural lesions gradually improved. Clinicians should consider the possibility of pleural TB, even in cases of diffuse nodular thickening mimicking pleural malignancy, especially in a situation relevant to TB.
Informed consent for publication was obtained from the patient.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





