


INTRODUCTION
Small cell lung cancer (SCLC), which represents 10ŌĆō15% of all lung cancer diagnoses, is known for its highly aggressive pathogenesis and fatal outcomes [1,2]. SCLC is closely associated with tobacco consumption and has a high mutation burden, with no known tumorigenic driver mutations [2,3]. In most cases, patients are diagnosed with extensive-stage SCLC (ES-SCLC), defined as tumors with distant metastasis or exceeding an area that can be treated within a single radiation field [2]. The standard chemotherapy regimen for SCLC, consisting of a platinum agent combined with etoposide, was defined several decades ago [4]. However, despite the initial chemosensitivity, therapeutic responses are not durable, and marked resistance is typically observed in patients with relapsed SCLC. This translates to a median overall survival (OS) of 14 months and 5-year survival rate of no more than 7% [1]. The addition of immune checkpoint inhibitors (ICIs) to these first-line chemotherapy regimens has constituted the first significant improvement in the clinical management of ES-SCLC over several decades [5,6]. On March 18, 2019, the U.S. Food and Drug Administration (FDA) approved atezolizumab in combination with carboplatin and etoposide for the first-line treatment of adult patients with ES-SCLC, based on an improvement in OS [7]. On March 27, 2020, the FDA approved durvalumab in combination with etoposide and either carboplatin or cisplatin as first-line treatment for patients with ES-SCLC [7].
To our knowledge, only two real-world studies have confirmed the beneficial effects of adding atezolizumab to chemotherapy in the treatment of ES-SCLC [8,9]. Given this paucity of data, we believe that the evaluation of retrospective data may help further evaluate immunotherapy in patients with ES-SCLC.
The Korean National Health Insurance Service has included coverage for the use of first-line atezolizumab for the treatment of ES-SCLC since April 2020. Here, we evaluated the clinical characteristics and outcomes of a Korean cohort known to receive a combination of chemotherapy and atezolizumab and compared these with those of an ES-SCLC cohort treated with chemotherapy alone.
METHODS
Collection of patient data
We collected data from all patients treated with first-line atezolizumab, etoposide, and carboplatin from the tumor registry at Pusan National University Hospital, Busan, South Korea (atezolizumab group) from April 2020. Furthermore, we analyzed the data obtained from a cohort of patients with ES-SCLC treated with chemotherapy alone (chemo-only group) between January 2018 and March 2020. Eligible patients included those who had been diagnosed with ES-SCLC in accordance with the Veterans Administration Lung Cancer Study Group. Patients with previous definitive concurrent chemoradiation therapy for limited-stage SCLC were also excluded. The study protocol was approved by the Institutional Review Board (IRB) of Pusan National University Hospital (IRB no. 2208-016-118). Moreover, the study was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the IRB of Pusan National University Hospital because of the retrospective nature of the study, and the analysis used anonymous clinical data.
Treatment and response evaluation
Baseline demographic characteristics (age, sex, body mass index, and Eastern Cooperative Oncology Group performance status [ECOG PS]) were recorded. Smoking status was categorized as never, former, or current according to the classification established in the National Health Interview Survey [10]. The date of diagnosis, initiation of first-line chemotherapy, number of metastatic organs, presence of specific organ metastases, and subsequent first-line treatment were recorded.
Efficacy outcomes included objective response rate (ORR), disease control rate, progression-free survival (PFS), and OS. Tumor response was assessed using computed tomography; however, all decisions concerning follow-up intervals and radiological tools were entirely at the discretion of the physician. The response to treatment was calculated based on the response evaluation criteria in solid tumors (RECIST) version 1.1. PFS was calculated from the start of first-line treatment to disease progression according to the RECIST version 1.1 or clinically by the treating physician or death, whichever occurred earlier. OS was defined as the time from the start of the first-line treatment to death from any cause.
Statistical analysis
All baseline characteristics of the patient cohorts were descriptive, and both chi-square and FisherŌĆÖs exact tests were used to compare the differences between categorical variables. PFS and OS were estimated using the Kaplan-Meier method, and differences in time distributions were compared using the log-rank test; the estimated median time (months) and 95% confidence interval (CI) are presented. All p values were two-sided, and statistical significance was set at p < 0.05. All statistical analyses were performed using the IBM SPSS Statistics Software for Windows (version 25.0; IBM Corp., Armonk, NY, USA).
RESULTS
Patient and treatment characteristics
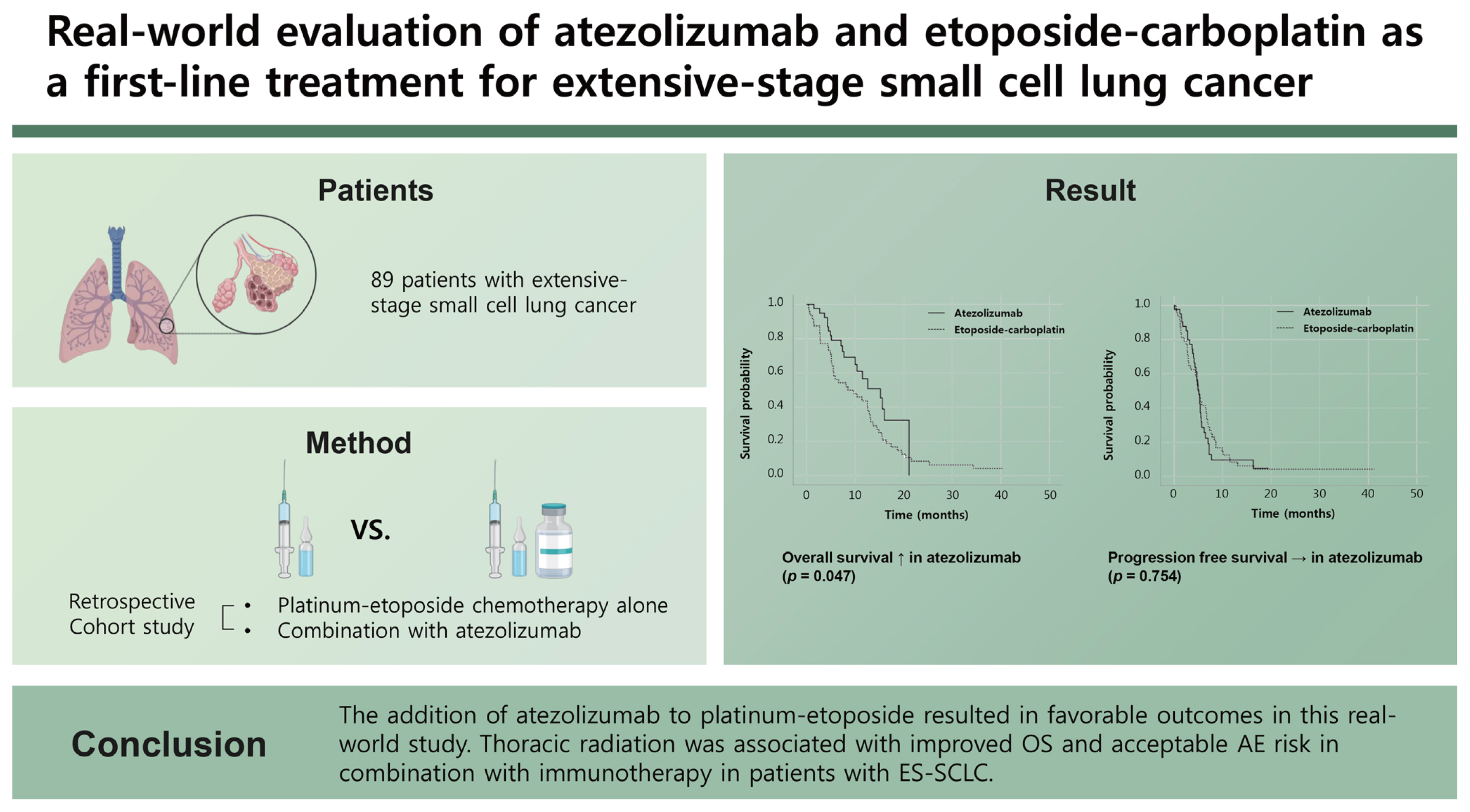
Our study included 89 patients: 41 in the atezolizumab group and 48 in the chemo-only group. Baseline characteristics were not significantly different between the two groups (Table 1), and this study population reflected real-world clinical practice and included patients with ECOG PS Ōēź 2 (23%) and those with brain metastases (33%). The median age of the atezolizumab group was 66 years (range, 36ŌĆō82), and the majority of the patients were men (90%). In addition, 84% (n = 32) of the patients in the atezolizumab group completed four cycles of atezolizumab, etoposide, and carboplatin combination chemotherapy, with a median number (range) of maintenance atezolizumab cycles of 2 (0ŌĆō18).
Furthermore, 30 patients (88.2%) from the atezolizumab group and 21 (45.7%) from the chemotherapy-only group received subsequent anticancer therapy after discontinuation of first-line treatment (p < 0.001). Follow-up data are available from April 2022. The median follow-up period was 8.3 months (range, 0.4ŌĆō40.3) and, at the time of the analysis, 20% of the patients (n = 8) were still undergoing treatment with atezolizumab. Only five patients (12%) presented with a time to treatment failure (TTF) of < 2 months, which was not significantly different from that in the chemo-only group (n = 9 [19%]; p = 0.561).
Treatment and survival outcomes
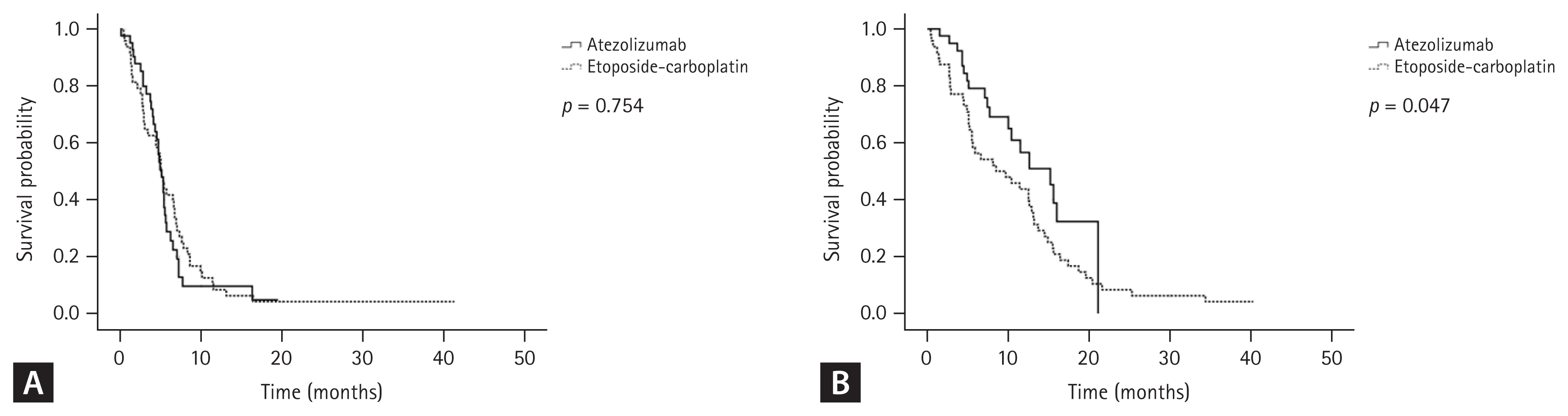
At the time of data collection, 81% and 96% of patients in the atezolizumab and chemo-only groups, respectively, had developed progressive disease, as defined by the RECIST criteria or via clinical identification by the treating physician or death. Median PFS was 5.1 months (95% CI, 4.384ŌĆō5.816) in the atezolizumab group and 5.0 months (95% CI, 4.208ŌĆō5.792) in the chemo-only group (Fig. 1A; p = 0.754). The ORRs were 65.9% and 44.2% for the atezolizumab and chemo-only groups, respectively (p = 0.052), and 10 patients (27%) in the atezolizumab group had a PFS of over 6 months. These patients also presented with low carcinoembryonic antigen (CEA) levels (p = 0.009), small primary masses (p = 0.029), low incidence rates of malignant pleural effusion (p = 0.033), and brain metastasis (p = 0.014). Median OS was 15.2 months (95% CI, 10.788ŌĆō19.612) in the atezolizumab group and 8.5 months (95% CI, 2.276ŌĆō14.724) in the chemo-only group (Fig. 1B; p = 0.047). In addition, multivariate analysis (Table 2) identified atezolizumab (hazard ratio [HR], 0.350; 95% CI, 0.184ŌĆō0.668; p = 0.001) and thoracic radiation therapy (HR, 0.223; 95% CI, 0.092ŌĆō0.537; p = 0.001) as favorable prognostic factors for OS. In contrast, the M1c stage was identified as a poor prognostic factor (HR, 1.856; 95% CI, 1.037ŌĆō3.321; p = 0.037) for OS.
Subgroup analysis based on radiation treatment
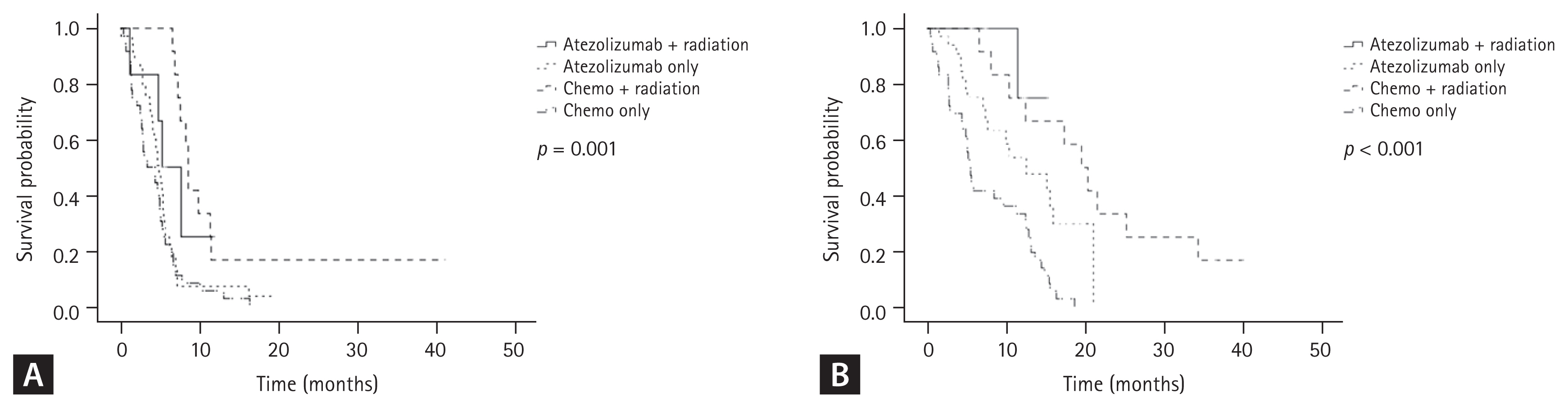
Fifteen percent of the patients (n = 6) received consolidative thoracic radiation therapy in addition to atezolizumab: five patients during maintenance atezolizumab treatment and one patient after the completion of second-line chemotherapy. A total of five patients received 52ŌĆō66 Gy, and the remaining one received 24 Gy. Furthermore, all patients (n = 12) in the chemotherapy-only group received sequential thoracic radiation therapy after completion of first-line chemotherapy. Both patient cohorts were divided into four groups based on their exposure to thoracic radiation therapy: (A) atezolizumab with thoracic radiation (n = 6), (B) atezolizumab without thoracic radiation (n = 35), (C) conventional chemotherapy with thoracic radiation (n = 12), and (D) conventional chemotherapy without thoracic radiation (n = 36). Median PFS was 5.3 months (95% CI, 2.515ŌĆō8.080) in group A, 4.9 months (95% CI, 4.079ŌĆō5.721) in group B, 8.6 months (95% CI, 8.098ŌĆō9.102) in group C, and 3.4 months (95% CI, 4.599ŌĆō5.601) in group D (p = 0.001; Fig. 2A). Median OS was not reached at the median value in group A, 12.6 months (95% CI, 6.262ŌĆō18.938) in group B, 19.6 months (95% CI, 14.508ŌĆō24.692) in group C, and 5.5 months (95% CI, 4.766ŌĆō6.234) in group D (p < 0.001; Fig. 2B). In addition, three patients from group A developed radiation pneumonitis, which was classified as grade 2 in two patients and grade 1 in one patient.
DISCUSSION
This retrospective study evaluated the clinical characteristics and efficacy of atezolizumab and etoposide-carboplatin first-line combination regimen as a new standard of care for ES-SCLC at a single Korean institution and compared the outcomes of these patients with those of a cohort treated with conventional chemotherapy alone. The overall median PFS and OS in our atezolizumab group were 5.1 (95% CI, 4.384ŌĆō5.816) and 15.2 months (95% CI, 10.788ŌĆō19.612), respectively, which is consistent with those of the previous landmark randomized trials, including the IMpower 133, CASPIAN study [5,6], and two recent real-world evaluations [8,9]. The median PFS and OS for the IMpower 133 study were 5.2 and 12.3 months, respectively [5]. Here, 62% of patients presented with poor prognostic characteristics, such as increased age (Ōēź 65 years), brain metastases, or ECOG PS Ōēź 2. Given this and the real-world settings, the observation of comparable ORRs (65.9%) and survival outcomes is encouraging.
In addition, 32 of our study patients (84%) received the planned four cycles of atezolizumab, etoposide, and carboplatin and an average of 2 (0ŌĆō18) atezolizumab maintenance cycles. This suggests that most disease progression is likely to occur immediately after completion of the cytotoxic chemotherapy combination period. PFS was longer in the CASPIAN study control group than in the IMpower133 control cohort [6], and this difference is likely to be driven by the fact that more than half of the patients in the chemo-only group in the CASPIAN study received six cycles of platinum-etoposide therapy [6]. This highlights the need to examine the value of increasing the number of cycles of cytotoxic chemotherapy to six.
Multivariate analysis of OS revealed that thoracic radiation therapy and the addition of atezolizumab were associated with increased survival in patients with ES-SCLC. This finding is consistent with a recently published study [8], in which Elegbede et al. [8] showed that thoracic radiation is associated with improved OS and acceptable adverse event (AE) risks in combination with immunotherapy in patients with ES-SCLC. Here, approximately 15% of the patients (6/41) in the atezolizumab group received thoracic radiation therapy. Most patients received thoracic radiation therapy at > 50 Gy during maintenance atezolizumab treatment. This finding supports the feasibility of thoracic radiation in the era of immuno-oncology. Furthermore, our data suggest that the chemo-only + thoracic radiation group had better OS outcomes than the atezolizumab without thoracic radiation group (median PFS: 8.6 months vs. 4.9 months, p = 0.001 and median OS: 19.6 months vs. 12.6 months, p < 0.001, respectively). Therefore, we suggest that a combination of thoracic radiation and immunotherapy should be considered when treating patients with ES-SCLC. However, the role of thoracic radiation in ES-SCLC treatment remains controversial. The CREST study, a phase 3 randomized trial, reported an overall improvement in survival in response to the addition of thoracic radiation for ES-SCLC [11], and a recent single-arm phase 1 trial reported no concerning safety profiles when evaluating combined thoracic radiation and pembrolizumab treatment in patients with ES-SCLC [12]. However, another randomized trial, NRG oncology RTOG 0937, failed to report any survival benefit with the addition of thoracic radiation [13]. However, these questions should be answered by the NRG oncology trial NRG LU007 (NCT04402788), which randomizes patients without progressive disease after 4ŌĆō6 cycles of platinum, etoposide, or atezolizumab and then compares atezolizumab only and atezolizumab and radiation (up to five sites including primary thoracic disease) based on the maintenance of ES-SCLC [14]. Therefore, this study is critical for determining the role of thoracic radiation in first-line chemo-immunotherapy.
Here, we report that the atezolizumab group received a higher rate of subsequent therapy than the chemo-only group (88.2% vs. 45.7%; p < 0.001), suggesting that this might have contributed to the improved survival of these patients. Most patients in the atezolizumab group completed four cycles of combined atezolizumab and cytotoxic chemotherapy and showed clear signs of disease progression during the atezolizumab maintenance phase. Generally, AEs were less frequent during the atezolizumab maintenance phase than during the combination phase, which may have in turn supported an increased appetite for more therapeutic interventions in this group.
In addition, we also noted that 10 patients (27%) in the atezolizumab group presented with a PFS window of more than 6 months, low CEA levels, small primary masses, low incidence rates of malignant pleural effusion, and brain metastasis. Several landmark studies have reported long-term survival outcomes of ICIs and attempted to identify prognostic factors predicting long-term survival in response to chemo-immunotherapy. However, clearly distinguishable characteristics have not been identified. Our data suggest that serum CEA levels and specific metastatic sites may predict improved longevity in response to immunotherapy.
Hyperprogression, characterized by unexpected radiological tumor growth, has been identified in many patients since the introduction of ICIs [15,16]. Various parameters such as tumor growth rate, tumor growth kinetics, and TTF have been introduced to precisely define hyperprogression [17]. However, although we did not evaluate hyperprogression in our study, there was no difference in the < 2-month TTF between the atezolizumab and chemo-only groups (n = 5 [12%] and n = 9 [19%], respectively; p = 0.561), suggesting that in this setting, ICI therapy in combination with classic chemotherapy may achieve rapid initial disease control without inducing unwanted hyperprogression in these patients.
Despite these valuable observations, this study had several limitations beyond those normally associated with retrospective research. First, the small sample size of our cohort, random selection, and different periods of our control group may have introduced potential bias. However, patient characteristics, including age, performance status, and incidence of brain metastasis, were well-balanced across both groups. Nevertheless, we still believe that it might be meaningful to compare the standards of care for each period. Second, the number of patients in the atezolizumab group who received radiation therapy was very low, indicating that no definite conclusions could be drawn. However, our findings showed a trend toward improved outcomes and manageable AEs among real-world patients receiving atezolizumab and radiation therapy. Third, these data were all from a single institution, which means that our results may not be representative of a larger patient population with ES-SCLC.
In conclusion, this study demonstrated the real-world efficacy of atezolizumab as a first-line chemotherapy for patients with ES-SCLC. Furthermore, this study supports the value of this new treatment strategy. However, a durable response to ICIs still occurs in a small minority of patients with ES-SCLC. Our data suggest that thoracic radiation in these patients may improve clinical outcomes. Additional studies are needed to confirm the benefits of adding thoracic radiation to chemo-immunotherapy for ES-SCLC.
KEY MESSAGE
1. Real-world data on immune checkpoint inhibitors in patients with ES-SCLC remain scarce.
2. Addition of atezolizumab to platinum-etoposide resulted in favorable outcomes in this real-world study.
3. Thoracic radiation was associated with improved overall survival and acceptable AE risks in combination with immunotherapy in patients with ES-SCLC.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





