


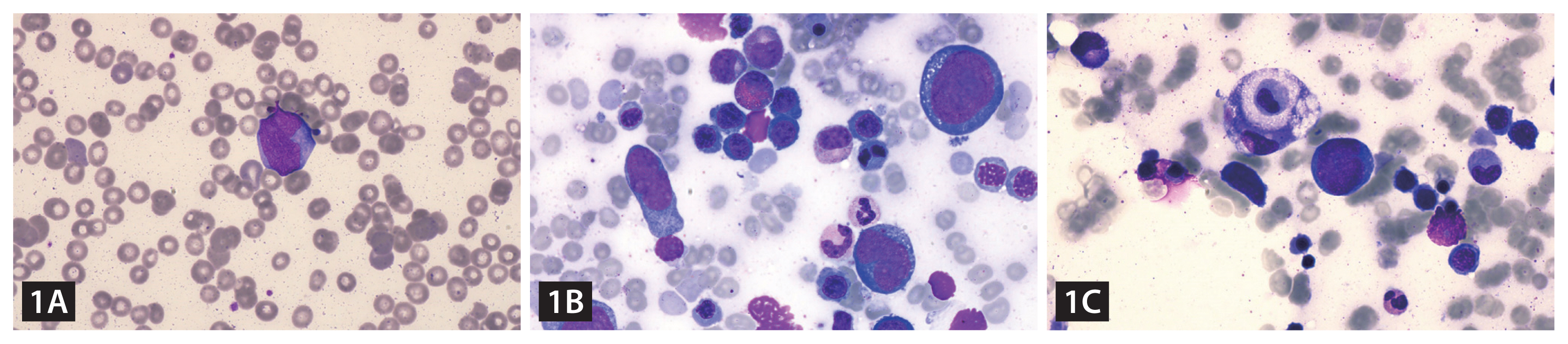
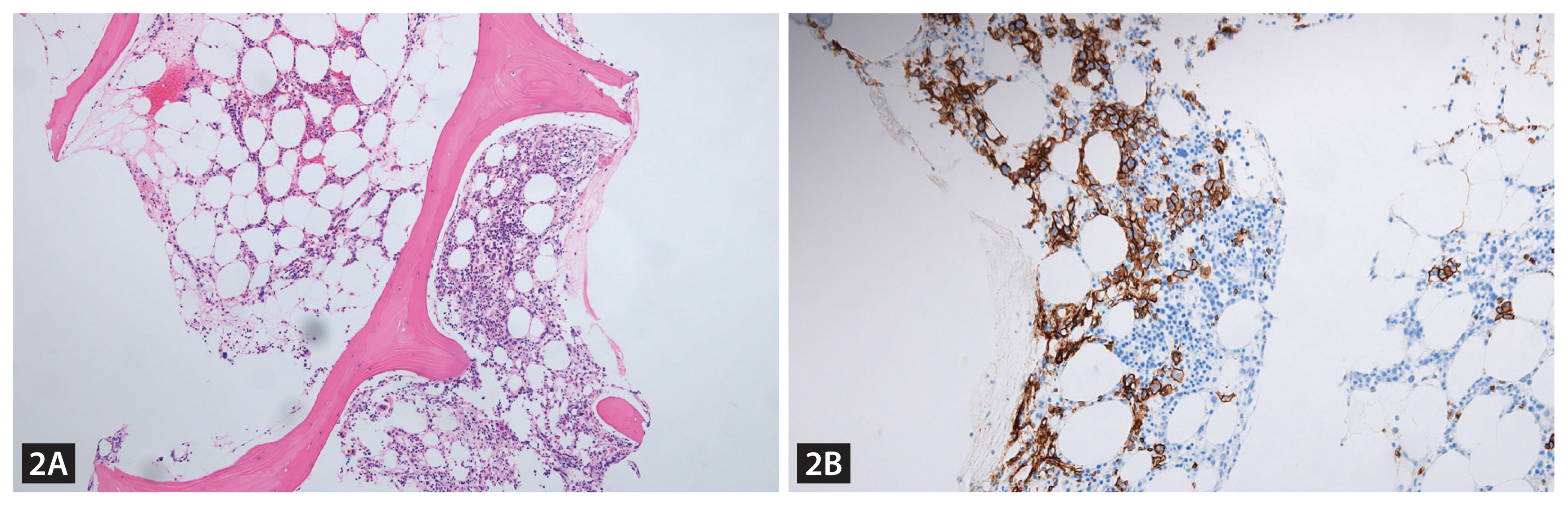
A 72-year-old woman was referred to a tertiary hospital with a high fever. The complete blood count showed pancytopenia (hemoglobin, 8.0 g/dL; white blood count, 2.97 ├Ś 109/L; and platelet count, 30 ├Ś 109/L). Her serum level of fibrinogen was normal, but that of triglyceride was 453 mg/dL (reference range 0ŌĆō200 mg/dL), and ferritin was 904.0 ng/mL (reference range, 13ŌĆō150 ng/mL). There was no splenomegaly or enlarged lymph nodes in the computed tomography scans. On the peripheral blood (PB) smear, leukoerythroblastosis and circulating neoplastic lymphoid cells (1%) were found (Fig. 1A). A bone marrow (BM) study was performed, and there was a significant number of neoplastic lymphoid cells (21.6%), which showed large sizes, indented nuclei with a clumped chromatin pattern, and a basophilic cytoplasm with cytoplasmic vacuoles (Fig. 1B). The number of histiocytes was also increased (3.4%), with the presence of hemophagocytic histiocytes engulfing nucleated cells (Fig. 1C). The neoplastic lymphoid cells showed strong positivity for CD20 (Fig. 2). An additional laboratory workup for hemophagocytic lymphohistiocytosis (HLH) was performed, and the results were as follows: NK-cell activity, 18 pg/mL (reference range Ōēź 500 pg/mL), and soluble interleukin-2 receptor level, 7,500 U/mL (reference range, 220ŌĆō530 U/mL). Based on these findings, she was diagnosed with HLH due to the BM involvement of diffuse large B-cell lymphoma. After one cycle of rituximab, cyclophosphamide, doxorubicin hydrochloride, vincristine and prednisone, the fever was reduced, and pancytopenia was normalized. The follow-up PB smear and BM study showed no evidence of lymphoma involvement. Therefore, the patient reached complete remission status.
The frequent clinical features of HLH are fever, hepatosplenomegaly, and lymphadenopathy. Sometimes an underlying malignancy might be masked by HLH due to the similarity of clinical signs. Therefore, the diagnosis and evaluation of the cause of HLH should be made carefully.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





