


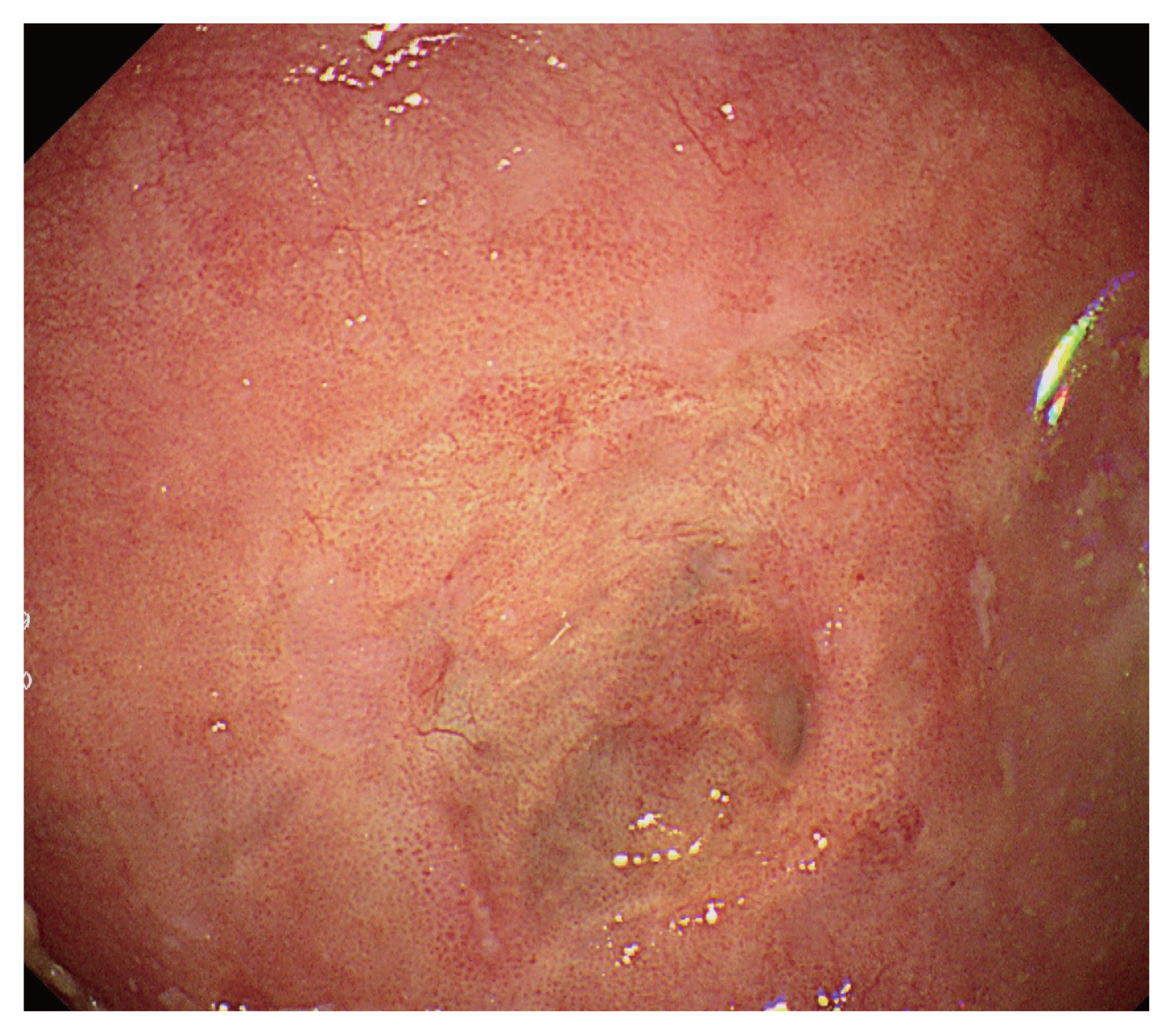
A 78-year-old male was admitted with symptoms of hematemesis and epigastric pain on the same day he visited the hospital. He had repeatedly experienced heartburn and intermittent dysphagia beginning 2 years prior. Esophagogastroduodenoscopy (EGD) showed a large epiphrenic esophageal diverticulum with a 5 cm diameter, accompanied by a bleeding ulcer and erosions in the diverticular mucosa located at 4 cm superior to the gastroesophageal junction (Fig. 1). Esophagography showed a 6 ├Ś 5 cm diverticulum that was connected to the esophagus at the approximately 2 cm-wide mouth of the diverticulum and the contrast agent traveled to the stomach after a half of its level was collected in the diverticulum (Fig. 2). Given the location of the ulcer in the epiphrenic esophageal diverticulum, we performed conservative management, such as fasting for 48 hours and administration with proton-pump inhibitor for 8 weeks instead of endoscopic therapy. For the management of symptom recurrence, the patient was provided with dietary education, including chewing foods slowly, drinking a sufficient amount of water, and not laying down immediately after a meal. The 3-month follow-up EGD showed improvement of the lesions in the diverticulum (Fig. 3). Until now, six months later, he is on outpatient follow-up without rebleeding.
Epiphrenic esophageal diverticulum rarely occurs in the distal esophagus within 10 cm from the gastroesophageal junction and is mostly a result from increased esophageal pressure [1,2]. The bleeding ulcer in the epiphrenic esophageal diverticular mucosa, a rare complication, is known to occur owing to the mucosal damage caused by chronic stimulation by bacterial overgrowth and inflammation associated with food stagnation [3]. This mechanism of bleeding is different from that in typical gastroesophageal ulcer. Accordingly, there is little literature with respect to which approach is the safest and most effective among the conservative, endoscopic, and surgical treatments [4ŌĆō6]. In this case report, a bleeding ulcer in the epiphrenic esophageal diverticulum was resolved using the conservative management.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





