


INTRODUCTION
Rheumatoid arthritis (RA) is a chronic, inflammatory autoimmune disease that primarily affects the joints [1]. Recent improvements in the understanding of RA pathogenesis have led to the development of targeted disease-modifying antirheumatic drugs (DMARDs) for modifying inflammatory cells and cytokines [2]. These include biologic DMARDs (bDMARDs), such as tumor necrosis factor inhibitors (TNFi), non-TNF inhibitors (non-TNFi) including abatacept and tocilizumab; and targeted synthetic DMARDs (tsDMARDs), including Janus kinase inhibitors (JAKi) [3]. With these various targeted DMARDs, treatment strategies suggest early diagnosis and early initiation of effective therapy aimed at remission or, at the least, low disease activity (LDA) [4].
The 2019 European Alliance of Associations for Rheumatology (EULAR) recommendations and 2021 American College of Rheumatology (ACR) guidelines for RA treatment place JAKi at the same level as the bDMARDs, being used for patients who experienced treatment failure with csDMARDs, and no preference is given to any of these agents [4,5]. Previous clinical trials have shown that tofacitinib is effective and generally well tolerated in the treatment of active RA, both as monotherapy and in combination with methotrexate (MTX) [6–8] or other csDMARDs [9]. Additionally, in patients naïve to bDMARDs, tofacitinib combination therapy with MTX has been shown to have similar efficacy to adalimumab and MTX combination therapy [10,11].
There are many factors to consider when selecting drugs in the real world, unlike in clinical trials wherein drug selection is randomized. These factors include patient characteristics (demographic and clinical characteristics, for example), as well as information about side effects, drug effectiveness, and medication logistics (such as frequency and route of administration) [12]. In terms of these aspects, compared with bDMARD, JAKi have a different route of administration and different supporting evidence regarding safety issues: bDMARDs are injectable (subcutaneous or intravenous), while JAKi is an oral medication, and there is more long-term information about the safety in bDMARDs. The latter consideration is because JAKi has only been recently approved for use. Furthermore, physician seemed to consider patients’ disease severity and comorbidities [13], as well as facility-related factors, such as the presence of space or assistants to explain medications to patients. Furthermore, shared decision-making (SDM) for the choice of treatment between patients and their physicians has been emphasized. Given the growing number of treatment options, recent guidelines have recommended the treat-to-target strategy and SDM as the first principles for creating RA treatment plans [5]. Therefore, a comparative effectiveness study between JAKi and bDMARDs–considering various factors for drug selection in clinical practice–is needed.
This study aimed to evaluate the effectiveness and safety of JAKi compared with bDMARDs in patients with RA in real-world practice.
METHODS
Protocol of the full study
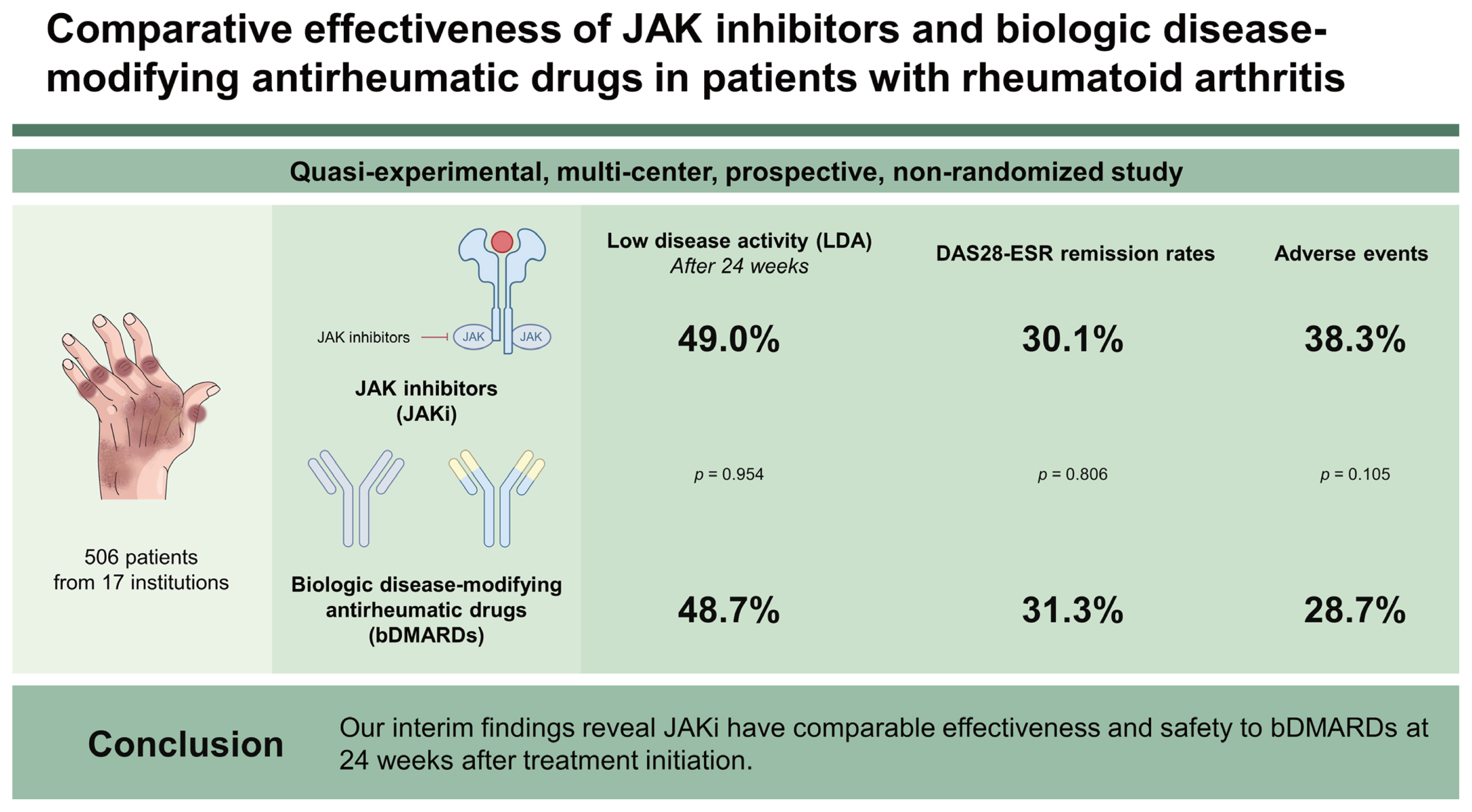
A quasi-experimental, multicenter, prospective, nonrandomized study of RA patients initiated on targeted therapy was conducted to compare the effectiveness and safety of two treatments. RA patients who started JAKi or bDMARDs were recruited by rheumatologists from 17 centers across the Republic of Korea, including 15 tertiary academic hospitals and 2 primary/secondary hospitals from April 2020 through August 2022. Disease activity is being assessed by well-trained health professionals, and participants completed patient-reported outcomes (PROs) at weeks 0, 12, 24, and 48 (Supplementary Fig. 1). All data are being entered into web-based case report forms.
The primary endpoint is the proportion of patients achieving LDA based on disease activity score (DAS)–28–erythroid sedimentation rate (ESR) (DAS28-ESR, <3.2) at 24 weeks after treatment initiation. The secondary endpoints are the proportion of patients achieving remission rate at 24 weeks, as well as the LDA and remission rates at 48 weeks. Disease activity is also being assessed using the DAS28–C-reactive protein (DAS28-CRP), Simplified Disease Activity Index (SDAI), Clinical Disease Activity Index (CDAI), and EULAR response criteria. The EULAR response criteria classify individual patients as nonresponders, moderate responders, or good responders, depending on the extent of change and the level of disease activity reached. Quality of life (QOL) and disability are being assessed using the EuroQol-5 dimension (EQ-5D) and Health Assessment Questionnaire–Disability Index (HAQ-DI) tools, respectively. Global Health assessment using Visual Analogue Scale (GH VAS) data are being collected by patients and their physicians.
The safety assessment includes capturing data on the development of adverse events (AEs) and abnormal laboratory tests for 52 weeks after treatment initiation. Severe AEs (SAEs) are also being identified. AE severity is being classified according to a five-grade scale (mild, moderate, severe, life-threatening, or death) according to definitions from the Common Terminology Criteria for Adverse Events. Serious AEs are defined as grade-3 to grade-5 AEs.
To participate in the study, RA patients must have met all of the following inclusion criteria: (1) > 19 years old; (2) moderate to severe active RA with an inadequate response or intolerance to MTX; (3) started on JAKi such as baricitinib, tofacitinib, or upadacitinib; or bDMARDs, including TNFi (etanercept, adalimumab, golimumab) or non-TNFi (abatacept, tocillizumab); (4) provided written informed consent to participate. Patients who did not provide written informed consent to participate were excluded.
The sample size was calculated for performing noninferiority testing of JAKi vs. bDMARDs using the proportion of patients achieving LDA based on DAS28-ESR at 24 weeks. The noninferiority margin was set to 13%, which is estimated by 50% of the effect of bDMARDs, i.e., 50% of the difference in the proportions of LDA achievement between bDMARD (36%) and placebo groups in previous studies [14–17]. With an assumption of a 1:1 allocation between the JAKi and bDMARD groups, the sample size was calculated as 215 patients for each group at a significance level, α, of 0.025 to acquire more than 80% of test power. Finally, with a predicted dropout rate of 15%, the total sample size was calculated as 506 patients for both groups.
Study population and outcomes of interim analysis
For this interim analysis, out of all the recruited patients, patients enrolled between April 2020 and October 2021 were extracted to evaluate outcomes at 24 weeks.
We evaluated the patients achieving LDA and remission at 12 weeks and 24 weeks after treatment with JAKi or bDMARDs. PROs at 12 weeks and 24 weeks were also compared between the two treatment groups. Additionally, the frequency of AEs at 24 weeks was determined.
Statistical analysis
Demographic and clinical features of JAKi and bDMARD users were compared using the chi-square analysis or Fisher’s exact test for categorical variables and the Mann–Whitney U test for continuous variables.
As the primary analysis, noninferiority testing using the proportion of patients achieving LDA based on DAS28-ESR at 24 weeks was performed, with a noninferiority margin of 13% representing 50% of the effect of bDMARDs, which is the active control. If the entire 95% confidence interval (CI) of the difference in proportions of LDA patients between the JAKi and bDMARD groups is above ~13%, we can conclude that JAKi is noninferior to bDMARDs.
In the secondary analysis, the proportions of patients achieving LDA at 12 weeks or remission at 12 weeks and 24 weeks (based on DAS28-ESR after treatment with JAKi or bDMARDs) were assessed as an intention-to-treat analysis. Proportions were compared between the two groups using the chi-square test. As a per-protocol analysis, PROs were compared between the two groups using the Mann–Whitney U test after treatment. All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Results were considered statistically significant when p values were < 0.05.
Ethical considerations
The study protocol was approved by the Institutional Review Boards of each participating hospital (IRB file No. HYUN 2019-11-031) or public IRB (https://public.irb.or.kr/). Additionally, this study is registered in the US ClinicalTrials.gov database (no. NCT04449224).
RESULTS
Baseline characteristics of the study population
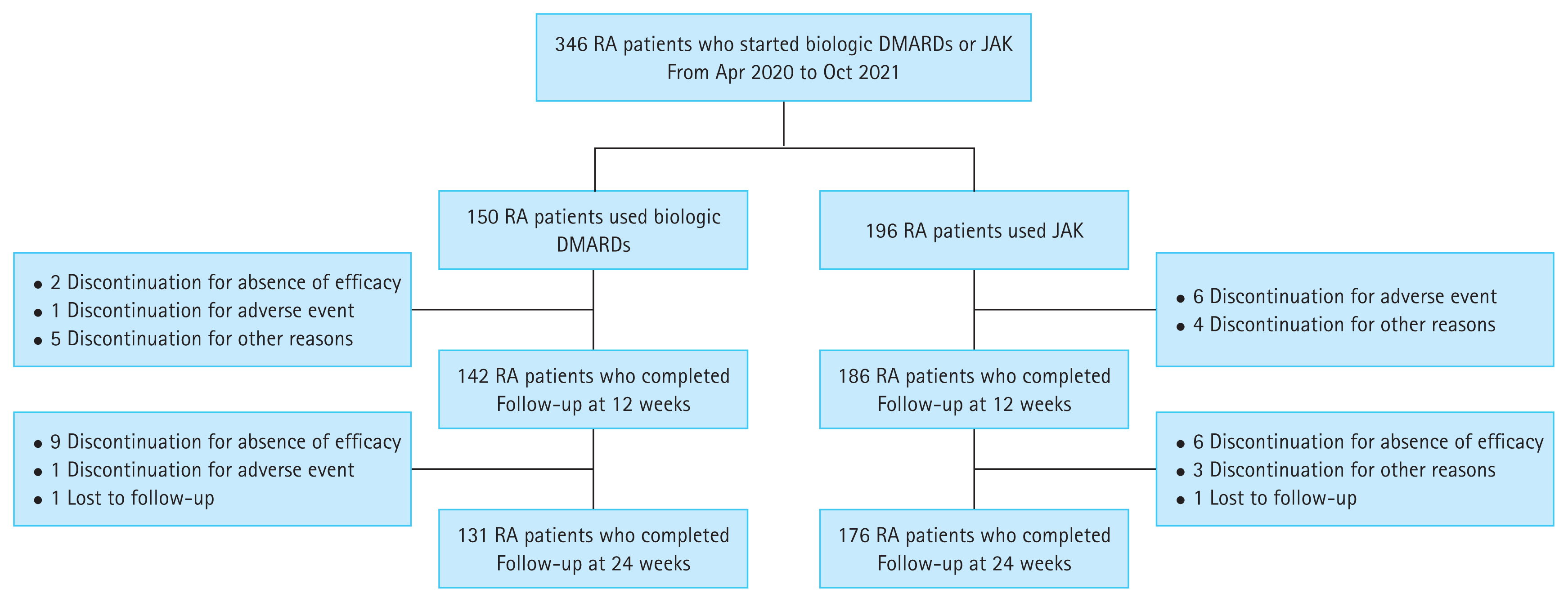
This interim analysis included 346 patients enrolled from April 2020 through October 2021 because at least 24 weeks had passed after follow-up initiation for these patients; this included patients treated with bDMARDs (n = 150) and patients treated with JAKi (n = 196) (Fig. 1). Among bDMARD users, more than half (58.2%) were treated with TNFi (n = 87), and 42.0% of patients were treated with non-TNFi (n = 63). Among JAK inhibitor users, 58.2% of patients were treated with baricitinib (n = 114), and the others were treated with tofacitinib (n = 51) and upadacitinib (n = 31) (Table 1). There were no differences in demographic characteristics between bDMARD and JAKi users. The baseline clinical characteristics of the study participants included in the interim analysis are summarized in Table 1.
Effectiveness
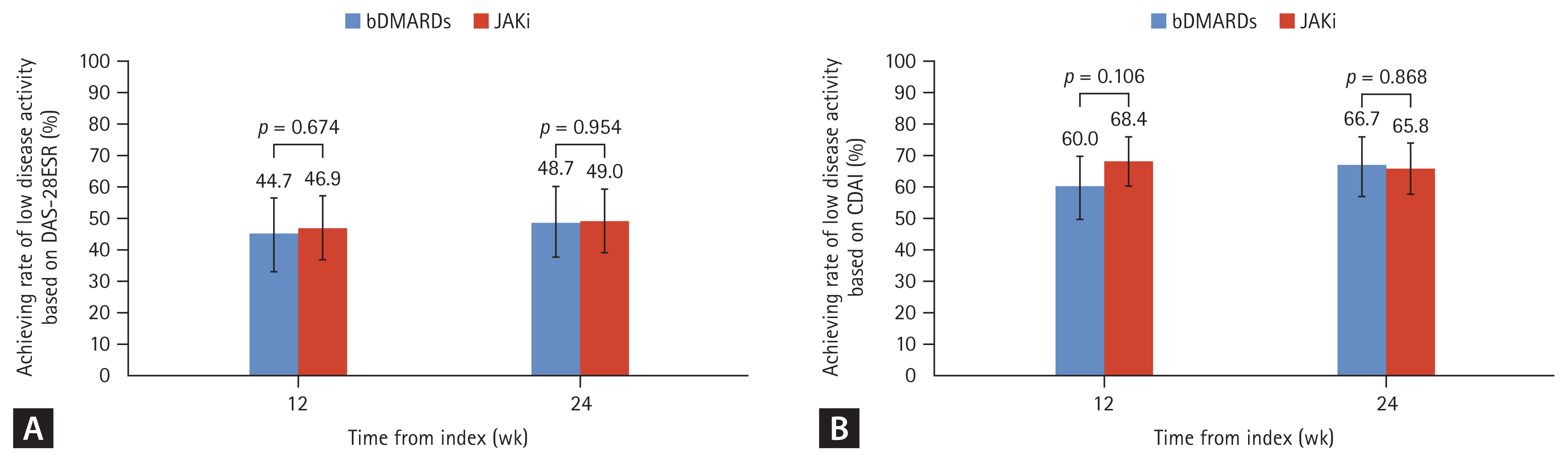
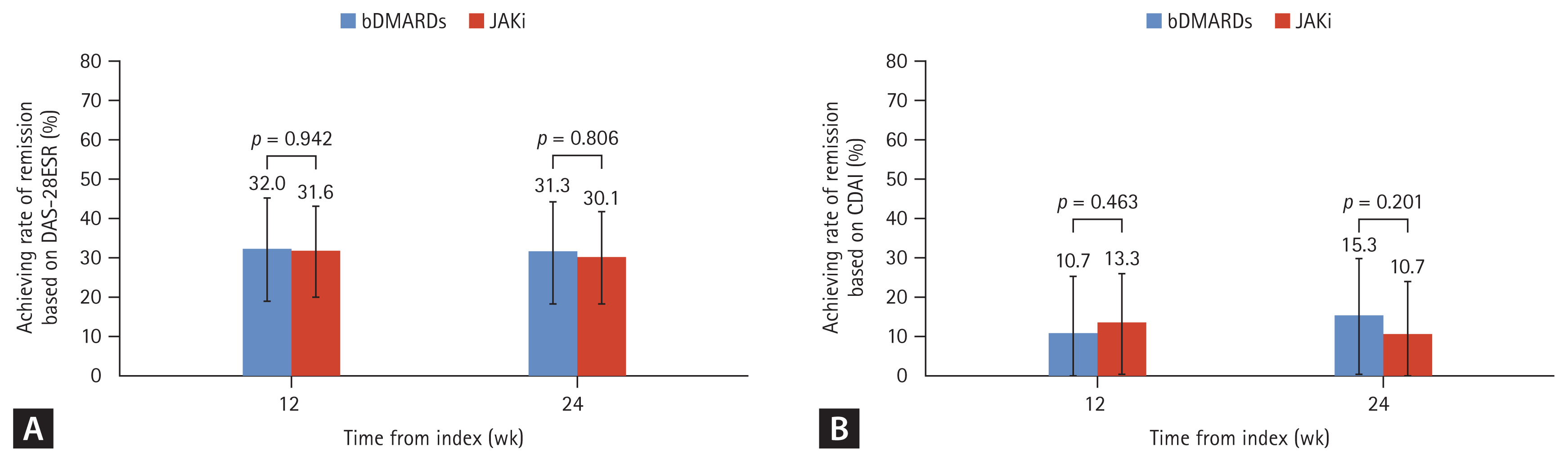
The rate of LDA achievement at 24 weeks was not significantly different between the two treatment groups (48.7% for bDMARDs and 49.0% for JAKi, p = 0.954). The difference between the groups was estimated to be 0.3% (95% CI, −10.6% to 11.3%), which was above −13% and implied that JAKi is not inferior to bDMARDs. The LDA rates at 12 weeks were also similar between the two groups (44.7% with bDMARDs and 46.9% with JAKi, p = 0.674). There were no statistically significant differences between the treatment groups in the remission rates at 12 weeks (32.0% with bDMARDs vs. 31.6% with JAKi, p = 0.942) and 24 weeks (31.3% with bDMARDs vs. 30.1% with JAKi, p=0.806).
The LDA and remission rates, based on DAS28-CRP, CDAI, and SDAI, were not significantly different between the treatment groups (Fig. 2, 3).
We compared PROs between two groups after treatment as per protocol at 12 and 24 weeks after treatment initiation. Changes in GH VAS, HAQ-DI, and EQ5D ratings were similar between the groups (Supplementary Fig. 2).
Safety
The frequency of AEs reported in the JAKi group was higher than that in the bDMARD group, but this difference was not statistically significant (75 of 196 patients [38.3%] vs. 43 of 150 patients [28.73%], p = 0.105). In the JAKi group, gastrointestinal disorders (n = 10, 5.1%) and skin disorders (n = 9, 4.6%) were most common, while infection (n = 9, 6.0%) and skin disorders (n = 8, 5.3%) were the most common in the bDMARDs group (Table 2). In terms of infection, herpes zoster was diagnosed in 5 patients (2 in the bDMARD and 3 in the JAKigroup), and 5 patients developed respiratory tract infections (2 in the bDMARD group and 3 in the JAKi group). Tuberculosis, malignancy, and thromboembolic events were not reported in either group. Two patients in the JAKi group experienced cardiac AEs: cardiac arrest (n = 1) and palpitations (n = 1), while no patients in the bDMARD group had cardiac AEs. There was no intergroup difference in the frequencies of SAE (Supplementary Table 1) or serious AEs (SAEs, 4.0% vs. 4.6% in the bDMARD and JAKi groups, respectively, p = 0.789; serious AEs, 3.3% vs. 3.6% in the bDMARD and JAKi groups, respectively, p = 0.905) (Table 3).
DISCUSSION
In the interim analysis of this ongoing quasi-experimental, multicenter, prospective, nonrandomized study, we demonstrated JAKi to have comparable effectiveness with bDMARDs at 24 weeks after treatment initiation in RA patients with inadequate responses to csDMARDs. Half of the RA patients reached LDA (49.0% with JAKi and 48.7% with bDMARDs), and a third of the patients (30.1% with JAKi and 31.3% with bDMARDs) achieved remission. For 24 weeks, there were no significant intergroup differences in the rates of overall AEs between the two treatment groups. Our results are in line with evidence from recent observational studies that have determined similar response rates between JAKi and bDMARDs [18–20]. However, some observational studies have found tofacitinib to be associated with better improvements in disease activity than those associated with bDMARDs after 6 or 12 months of treatment in bDMARD-naïve RA patients [21–23]. Notably, in one study, this difference was not observed in bDMARD-failure RA patients [21]. Moreover, early introduction of tofacitinib has been associated with similar or better survival than that associated with bDMARD administration [23]. Therefore, the drug selection order is important because previous experience with bDMARDs may be a crucial factor affecting drug responses. In our interim analysis results, the LDA achievement rate at 12 weeks was numerically higher in the JAKi group than in the bDMARD group, but there was no statistical significance. Further follow-up is needed to determine the comparative effectiveness of both treatments.
The AE profile observed with JAKi was similar to that observed with bDMARDs. There was, however, a nonsignificant trend toward a higher frequency of AEs associated with JAKi compared with bDMARDs. This could be due to heightened concerns from physicians and patients, causing them potentially to be more careful with this newer treatment. The rates of infections, including herpes zoster, associated with drug administration were similar between the two treatment groups for 24 weeks after treatments. Neither venous thromboembolism nor malignancy was reported in either group. Only one patient treated with JAKi died, with cardiac arrest reported as the cause of death. Previous observational studies have reported higher incidences of herpes zoster infection among patients treated with JAKi [24,25]. A recent large observational study conducted in the United States using claims database data found tofacitinib to be associated with an increased risk of hospitalization for serious infection compared with bDMARDs [26]. Additionally, a recent randomized controlled trial demonstrated that the risks of major adverse cardiovascular events and cancers were higher in association with tofacitinib than with TNF inhibitors among patients with cardiovascular risk factors [27]. However, United States registry data have demonstrated tofacitinib to be associated with similar major adverse cardiovascular events, serious infection, malignancy, death, and venous thromboembolism rates compared with bDMARDs [28]. Long-term follow-up studies are needed to confirm the safety of JAKi.
The strength of our study lies in the provision of information on the real-world management of patients with RA. This study has good generalizability because the patients have been enrolled from multiple healthcare facility levels: tertiary hospitals, community hospitals, and private clinics. To the best of our knowledge, this is the only data set in Korea that includes bDMARD-naïve RA patients receiving targeted therapy at multiple healthcare facility levels. Additionally, this study included three JAKi approved for the treatment of RA in Korea. Therefore, we can compare the effectiveness and safety of each drug in the final analysis, which is important because drugs of the same class may have different effects.
In conclusion, our interim findings of this ongoing real-world, pragmatic, multicenter study revealed JAKi to be comparable with bDMARDs, in terms of effectiveness and safety, at 24 weeks after treatment initiation. We hope that the final analysis will present the effectiveness and safety of the two treatments in bDMARD-naïve patients with RA, as well as provide future research directions.
KEY MESSAGE
1. Our interim findings of this ongoing real-world, pragmatic, multicenter study reveal that JAKi have had comparable effectiveness to bDMARDs at 24 weeks after treatment initiation in patients with RA naïve to targeted therapy.
2. The frequency of AEs reported in the JAKi group was numerically higher than that in the bDMARDs group, but the frequencies of serious and severe AEs were comparable between the groups.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement figure 1
Supplement figure 1 Print
Print





