


INTRODUCTION
Asthma is a heterogenous, chronic inflammatory disease of the airways, which affects approximately 339 million patients worldwide [1]. In South Korea, the prevalence of asthma has steadily risen over the past decade [2], with approximately 2.9% of the population diagnosed with asthma in 2017 [3]. Despite recent advances in asthma management and the availability of international evidence-based treatment guidelines, asthma remains poorly controlled across the world, including Asia [4–6]. This is likely due to, in part, a long-held paradox of asthma management, whereby for over 20 years, the Global Initiative for Asthma (GINA) recommended as-needed short-acting β2-agonists (SABAs) as the preferred reliever for patients with mild asthma, even though they have no inherent anti-inflammatory activity [7]. However, with accumulating evidence that SABA overuse (≥ 3 canisters/year) is associated with an increased risk of exacerbations, hospitalizations, and mortality [8,9], GINA no longer recommends as-needed SABAs without concomitant inhaled corticosteroid (ICS) and instead recommends as-needed low-dose ICS-formoterol as the preferred reliever for adults and adolescents with mild asthma (GINA treatment steps 1–2) and for those with moderate-to-severe asthma (GINA treatment steps 3–5) who are prescribed ICS-formoterol maintenance therapy [10].
Insights on asthma medication prescribing patterns, particularly for SABA prescriptions, will provide clinicians and healthcare policymakers with a better understanding of the extent of SABA use and ensure that treatment practices align with the latest evidence-based treatment recommendations. However, although South Korea has several well-established databases, such as the National Health Insurance Service (NHIS) [11] and the Health Insurance Review & Assessment Service (HIRA), there is a paucity of data on potential SABA overuse across the country, with only one previous study examining trends of annual SABA use and overuse and the impact of SABA overuse on mortality [12].
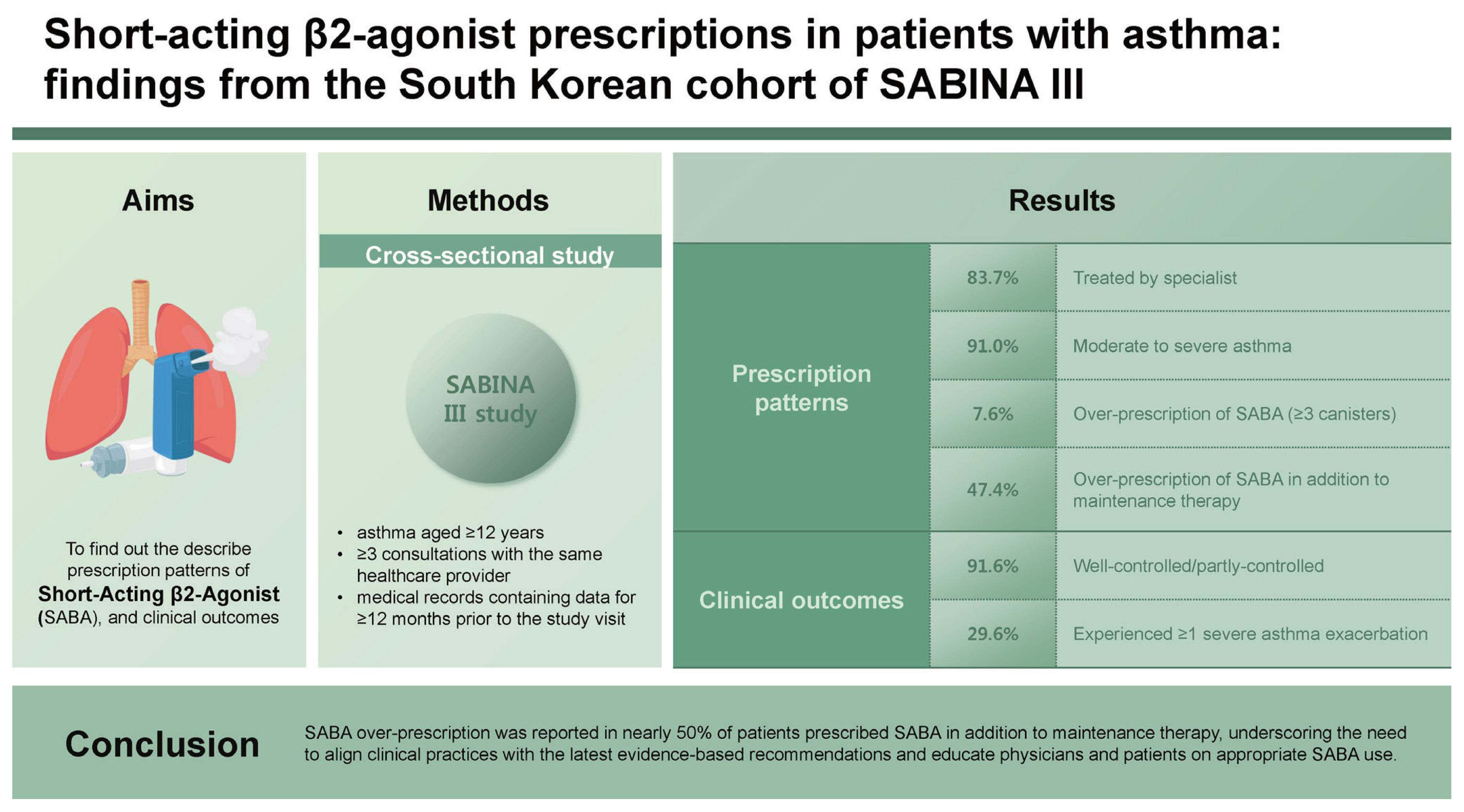
To bridge this gap and provide a global view of SABA prescriptions, the SABA use IN Asthma (SABINA) program was initiated to describe asthma treatment prescription patterns, the extent of high SABA prescription, and its impact on asthma-related clinical outcomes through a series of global studies [13]. Results from SABINA I and II, retrospective observational studies conducted in the United Kingdom and Europe, respectively, demonstrated that SABA overprescription (≥ 3 canisters/year) was common and associated with poor clinical outcomes [8,14]. The SABINA III arm of the program, conducted in 23 countries across Asia-Pacific, Africa, the Middle East, Latin America, and in Russia, used electronic case report forms (eCRFs) to overcome the lack of robust national healthcare databases in many of the participating countries [15]. Here, we report results from the South Korean cohort of the SABINA III study, to provide real-world evidence on asthma treatment practices in this country.
METHODS
Study design and population
Detailed methodology for SABINA III has been published previously [15]. In brief, this observational, cross-sectional study was conducted at 16 sites (6 primary, 1 secondary, and 9 tertiary care sites) across South Korea, with patient recruitment between July 2019 and November 2019 (Supplementary Table 1). The primary and specialist care study sites were selected using purposive sampling with the aim of obtaining a sample representative of how patients with asthma were being treated in their country.
Retrospective data were obtained from existing medical records, and patient data were collected during a study visit and entered into an eCRF. The study was conducted in compliance with the Declaration of Helsinki and Good Clinical Practice guidelines, and each study site received approval from the Institutional Review Board (Clinical Trial Center, Konkuk University Hospital; IRB reference number: KUMC 2019-06-017).
Patients aged ≥ 12 years with a documented diagnosis of asthma, ≥ 3 recorded consultations with their healthcare provider, and medical records containing data for ≥ 12 months prior to the study visit were enrolled [15]. Patients with other chronic respiratory diseases or limiting acute or chronic conditions were excluded. Signed informed consent was obtained from all patients.
Study variables and outcomes
Patients were characterized based on practice type (primary or specialist care) and investigator-classified asthma severity (guided by GINA 2017 treatment steps: steps 1–2, mild asthma and steps 3–5, moderate-to-severe asthma) [16]. Sociodemographic characteristics and disease characteristics were recorded during the study visit. Sociodemographic characteristics included age, sex, body mass index (categorized according to the Asia-Pacific classification [17]); education (primary and/or secondary school, high school, or university and/or post-graduate education); healthcare reimbursement (not reimbursed, partially reimbursed, or fully reimbursed); and smoking history (active smoker, former smoker, or never smoker).
Asthma medication prescriptions in the preceding 12 months, including SABA, ICS, ICS–long-acting β2-agonist (LABA) fixed-dose combinations, oral corticosteroid (OCS) burst treatment (defined as a short course of intravenous corticosteroid or OCS administered for 3–10 days or a single dose of an intramuscular corticosteroid to treat an exacerbation), long-term OCS treatment (defined as any OCS treatment for > 10 days), and antibiotics prescribed for asthma (regardless of duration of use), were recorded. SABA prescriptions were categorized as 0, 1–2, 3–5, 6–9, 10–12, or ≥ 13 canisters, with over-prescription defined as ≥ 3 canisters in the 12 months before the study visit [8–10]. ICS prescriptions were categorized by prescribed average daily dose (low, medium, or high) [16].
Severe asthma exacerbations in the 12 months before the study visit were defined based on the European Respiratory Society/American Thoracic Society guidelines as a worsening of asthma symptoms requiring hospitalization, an emergency room visit, or the need for OCS burst treatment [18]. During the study visit, patients were questioned about their level of asthma control, which was evaluated using the GINA 2017 assessment for asthma control and categorized as well-controlled, partly controlled, or uncontrolled by the investigator [16].
Statistical analysis
Descriptive analyses characterized patients according to sociodemographic and clinical characteristics. Continuous variables were described as number (%), mean (standard deviation [SD]), and median (minimum, maximum). Categorical variables were summarized by frequency counts and percentages.
RESULTS
Overall, 476 patients were analyzed; however, data on practice type were unavailable for 4 patients (Supplementary Fig. 1). Most patients were treated by specialists (83.7%) and had investigator-classified moderate-to-severe asthma (91%).
The mean ± SD age of patients was 55.4 ± 15.1 years (Table 1). The majority of patients were female (63.0%), overweight or obese (64.7%), had never smoked (66.8%), and reported partially reimbursed healthcare (90.1%). Patients had a mean ± SD asthma duration of 6.5 ± 6.1 years, with most at GINA treatment step 3 (42.4%) or 4 (38.0%). Overall, 84.7% of patients had ≥ 1 comorbidity.
Asthma treatments in the 12 months before the study visit
SABA prescriptions
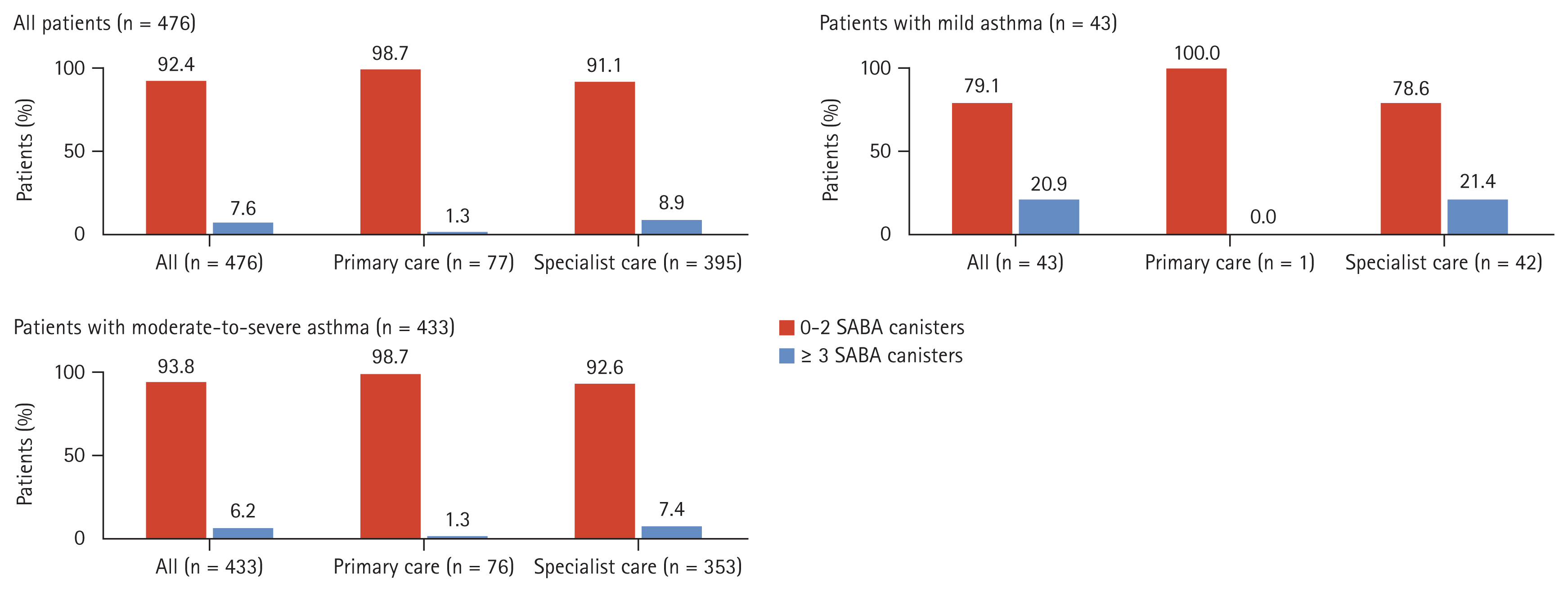
Overall, 7.6% of patients were prescribed ≥ 3 SABA canisters in the previous 12 months, defined as over-prescription (Fig. 1). However, 83.8% of patients received no SABA prescriptions. A higher proportion of patients under specialist care were prescribed ≥ 3 SABA canisters compared with those under primary care (8.9 vs. 1.3%).
Only 1 patient was prescribed SABA monotherapy, with a prescription of 1–2 SABA canisters in the previous 12 months. However, 16.0% of patients were prescribed SABA in addition to maintenance therapy, with 47.4% prescribed ≥ 3 SABA canisters (Table 2). In primary care, 5.2% of patients, all of whom had moderate-to-severe asthma, were prescribed SABA in addition to maintenance therapy. In specialist care, 18.2% of patients (21.4% with mild asthma and 17.8% with moderate-to-severe asthma) were prescribed SABA in addition to maintenance therapy; of these, all patients with mild asthma and 41.3% of those with moderate-to-severe asthma were prescribed ≥ 3 SABA canisters. Overall, only 0.6% of patients were prescribed a short-acting muscarinic antagonist.
ICS prescriptions
Overall, ICS monotherapy was prescribed to 6.3% of patients, all of whom were treated by specialists. The majority of these patients were classified with mild asthma, with 80% prescribed low-dose ICS (Table 2).
Most patients (95.4%) were prescribed an ICS-LABA fixed-dose combination as maintenance therapy, with 50.0% prescribed low-dose ICS (Table 2). With the exception of 1 patient, primary care physicians prescribed ICS-LABA to all patients with moderate-to-severe asthma, with 70.7% prescribed low-dose ICS. In specialist care, a greater proportion of patients with moderate-to-severe asthma were prescribed ICS-LABA compared with those with mild asthma (99.7 vs. 52.4%). Of these, 45.7% and 42.2% were prescribed low- and medium-dose ICS, respectively.
Other prescriptions for asthma
One or more OCS burst was prescribed to 25.0% of patients, with this occurring in more patients in primary care compared with specialist care (32.5 vs. 23.3%; Table 2). In primary care, all patients with moderate-to-severe asthma were prescribed ≥ 1 OCS burst. In specialist care, 11.9% of patients with mild asthma and 24.6% of patients with moderate-to-severe asthma were prescribed ≥ 1 OCS burst.
Long-term OCS maintenance therapy was prescribed to 6.7% of patients, with higher prescription rates observed in specialist care compared with primary care (7.3 vs. 3.9%; Table 2). All patients prescribed long-term OCS treatment in primary care had moderate-to-severe asthma. In specialist care, 2.4% of patients with mild asthma and 7.9% with moderate-to-severe asthma were prescribed long-term OCS treatment.
Additionally, 13.3% of patients were prescribed antibiotics for asthma, with higher prescription rates observed in primary care compared with specialist care (26.0 vs. 10.9%; Table 2).
Asthma-related clinical outcomes
Patients reported a mean ± SD of 0.5 ± 1.1 severe asthma exacerbations in the previous 12 months, with 29.6% experiencing ≥ 1 severe exacerbation (Table 3, Supplementary Fig. 2). The proportion of patients with ≥ 1 severe exacerbation was the lowest in those prescribed ICS-containing therapy (ICS monotherapy or ICS-LABA fixed-dose combination) and the highest in those prescribed ≥ 1 OCS burst (Supplementary Fig. 2).
Asthma symptom control was assessed as well-controlled in 61.8%, partly controlled in 29.8%, and uncontrolled in 8.4% of patients (Table 3). Almost twice as many patients treated in specialist care had well-controlled asthma compared with those treated in primary care (67.1% vs. 35.1%). In specialist care, a higher percentage of patients with mild asthma were well-controlled compared with those with moderate-to-severe asthma (83.3% vs. 65.2%).
DISCUSSION
This cross-sectional study [15] provides valuable real-world insights into asthma treatment practices in patients predominantly under specialist care in this South Korean cohort of the SABINA III study [15]. Although SABA over-prescription was observed in only 7.6% of patients, in the 16% of patients prescribed SABA in addition to maintenance therapy, almost half (47.4%) were prescribed ≥ 3 SABA canisters in the preceding 12 months (over-prescription), underscoring the need for improvements in asthma care across the country.
Compared with country-aggregated data from SABINA III [15], patients from South Korea appeared to be more effectively managed and treated, with lower rates of SABA over-prescription (38 vs. 7.6%). Furthermore, compared with the overall SABINA III cohort [15], a higher percentage of patients from the Korean cohort reported well-controlled asthma (43.3 vs. 61.8%), with a lower proportion experiencing ≥ 1 severe exacerbation in the preceding 12 months (45.4 vs. 29.6%). These differences were observed despite the relatively similar sociodemographic and disease characteristics between the overall SABINA III [15] and South Korean cohorts, with most patients from both datasets treated under specialist care and classified as having moderate-to-severe asthma. Although some differences were observed between the 2 cohorts, for example, compared with the overall SABINA III cohort [15], patients from the South Korean cohort had a lower mean asthma duration and body mass index, with a greater percentage being active and former smokers and reporting ≥ 5 comorbidities, it is unlikely that these factors contributed to the improved patient outcomes observed in the South Korean cohort.
Notably, over 80% of patients received no SABA prescriptions, with only 1 patient prescribed SABA monotherapy in the preceding 12 months. Additionally, relatively few patients (16%) were prescribed SABA in addition to maintenance therapy, of whom nearly half were prescribed ≥ 3 SABA canisters. Although limited studies to date have evaluated the extent and burden of SABA over-prescription in South Korea, our findings align with previous country-specific studies that have documented similar low rates of SABA use [12,19]. This low SABA use has been attributed to SABA being considered an “emergency medication” and not a rescue medication in Korea, with most patients only using SABA following an acute exacerbation and not for the prevention of exacerbations [12]. However, some factors specific to this study may have also contributed to the low SABA prescription rates observed. The majority of patients were treated by specialists who are generally more familiar with current asthma treatment guidelines and have the expertise and knowledge to provide optimal asthma care [20]. Additionally, most patients in this study were treated at tertiary or primary care centers, with only 1 secondary care site enrolled. This may have influenced SABA prescribing habits, with evaluation of data from the HIRA nationwide database (2013–2014) revealing lower SABA prescription rates in tertiary (41.7%) and primary (23.6%) care compared with secondary care (71.5%) [21].
The availability of SABA in Korea is strictly regulated [22]. Based on results from a cross-sectional epidemiologic study using the NHIS-National Sample Cohort database (2002–2012) where SABA overuse (≥ 3 canisters/year) was associated with all-cause mortality (adjusted odds ratio [OR], 1.72; 95% confidence interval [CI], 1.61–1.84) and asthma-related mortality (adjusted OR, 3.25; 95% CI, 2.72–3.89) [12], it would be advantageous for other countries to follow the lead of South Korea to drive policy changes that regulate the purchase of SABA over-the-counter (OTC) to ensure optimal asthma management.
Previous surveys and nationwide population-based studies from South Korea have reported low ICS prescription rates in patients with asthma, particularly those treated in primary care [12,20,21,23,24]. In contrast, in our study, most patients were prescribed ICS-containing therapy (ICS monotherapy, 6.3%; ICS-LABA fixed-dose combination, 95.4%), which was in alignment with over 90% being classified as having moderate-to-severe asthma. Among patients prescribed ICS-LABA fixed-dose combinations, 50.0% and 39.6% were prescribed low-and medium-dose ICS, respectively, suggestive of the use of an ICS-LABA combination inhaler as both maintenance and reliever therapy (MART), which is common practice in South Korea. In addition, over 50% of patients with mild asthma treated by specialists were prescribed an ICS-LABA fixed-dose combination, which did not conform to GINA recommendations at the time this study was conducted [16]. This observation may reflect physician preference for an ICS-LABA fixed-dose combination over ICS monotherapy, to maximize patient adherence and ensure that even those with mild symptoms receive anti-inflammatory medication to prevent exacerbations. Overall, the high rate of ICS prescribing observed in this study may be attributable to a patient population treated largely under specialist care.
Studies based on NHIS and other databases have reported high OCS prescription rates across South Korea [12,19,21,23]. Notably, annual qualitative assessments of asthma management provided by the HIRA from 2015 to 2016 consistently reported high OCS prescription rates without ICS, ranging from 28.2 to 30.4% [25]. Unsurprisingly, OCS bursts were prescribed to 25.0% of all patients in this study, with prescription rates being higher in primary care compared with specialist care. Although lower than that reported in previous reports, this remains a matter of concern, since even short dosing periods (3–7 d) of OCS are associated with an increased risk of adverse events, including decreased bone density, hypertension, and gastrointestinal ulcers/bleeds [26]. In line with the findings of previous reports from Korea [25] and considering that 10.1% of patients who were prescribed an OCS burst in this cohort did not experience severe exacerbations, OCS may have been used as a reliever medication to treat acute episodes of symptom worsening in this study. Furthermore, the high percentage of patients prescribed OCS bursts may be due to some physicians prescribing OCS as a standby medication in patients’ asthma action plans in the event of worsening asthma symptoms. However, these findings may also reflect physician beliefs and patient preferences, with both physicians at primary, secondary, and tertiary teaching hospitals in South Korea [20] and patients from South Korea [27] and other parts of Asia [28,29] reporting a preference for oral medications. Interestingly, 13.3% of patients were prescribed antibiotics for asthma, suggesting a lack of familiarity with asthma guidelines as GINA does not support the routine use of antibiotics without a strong evidence of lung infection [10].
Overall, 61.8% of patients from this South Korean cohort of the SABINA III study had well-controlled asthma, which was higher than that observed in the overall SABINA III cohort (43.3%) [15] and in Korean patients from the multinational Asthma Insight and Management survey (27%) [27]. Several factors may have contributed to this improved level of asthma control. Although not captured in this study, most patients were treated by specialists who are more likely to prescribe MART, which may have improved asthma control and reduced as-needed medication use [30,31]. Indeed, most patients were prescribed an ICS-LABA fixed-dose combination, which is associated with positive asthma outcomes [32]. Additionally, the low level of SABA prescriptions, combined with the strict prohibition of SABA purchase OTC in South Korea [22], may possibly have further contributed to improved patient outcomes. Finally, the robust healthcare infrastructure in South Korea, in particular, the provision of compulsory health insurance and availability of medical aid may have potentially had a favorable impact on asthma control by ensuring access to essential asthma medications and optimizing patient adherence to prescribed therapies [11]. Nevertheless, even though most patients in this study had well-controlled asthma, 29.6% of patients still experienced ≥ 1 severe exacerbation in the previous 12 months [10]. Such findings may indicate potential over-estimation of disease control by both physicians and patients, leading to under-treatment of asthma [33–35]. Consequently, this study emphasizes the need for educational initiatives targeting both patients and physicians to further improve asthma care in South Korea.
There are some limitations to this study. First, prescription data may not reflect actual medication use; therefore, rates of treatment compliance or noncompliance were unknown. Second, since data entry into the eCRF relied on clinician assessment, findings may have been impacted by misinterpretation of instructions, incorrect patient classification based on asthma severity, or recall bias. Third, the majority of patients were recruited from specialist care, resulting in most patients being classified with moderate-to-severe asthma, and precluding comparisons across asthma severities. A possible explanation for this could be the lack of a well-established primary care system in South Korea [36], together with inherent challenges commonly encountered in conducting clinical trials at a primary care level. Thus, the study population represents a “better case scenario” and is not truly representative of the overall asthma patient population in South Korea. Therefore, additional studies are required to gain a more comprehensive understanding of asthma treatment patterns in both primary and specialist care across South Korea. Fourth, data on patients prescribed a MART regimen were not recorded. Finally, due to the relatively small sample size, it was not feasible to examine the association between SABA prescriptions and asthma-related clinical outcomes. However, overall findings from SABINA III indicated that ≥ 3 SABA prescriptions/year (vs. 1–2 SABA prescriptions) were associated with increasingly lower odds of controlled or partly controlled asthma and higher rates of severe exacerbations across many countries, healthcare settings, and asthma severities [15]. Nevertheless, this study provides comprehensive real-world data on current prescription patterns of asthma medications in patients in this South Korean cohort of the SABINA III study.
In conclusion, results from the South Korean cohort of SABINA III demonstrated that SABA over-prescription (≥ 3 canisters/year) occurred in < 10% of patients. However, despite treatment predominantly under specialist care, SABA over-prescription occurred in almost half of all patients prescribed SABA in addition to maintenance therapy. Although approximately 60% of patients reported well-controlled asthma, nearly 30% experienced ≥ 1 severe asthma exacerbation in the previous 12 months. These findings reinforce the need to continue aligning clinical practices with the latest evidence-based treatment recommendations to ensure further improvements in asthma management across South Korea.
KEY MESSAGE
1. Findings from this South Korean cohort of the SABINA III study revealed that SABA over-prescription (≥ 3 canisters/year) was relatively low, occurring in < 10% of all patients.
2. However, despite treatment predominantly under specialist care, SABA over-prescription was reported in almost half of all patients prescribed SABA in addition to maintenance therapy.
3. Although asthma was well-controlled/partly controlled in 91.6% of patients, 29.6% of patients experienced ≥ 1 severe asthma exacerbation in the 12 months prior to the study visit, underscoring the need for improvements in asthma care across the country.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement figure 1
Supplement figure 1 Print
Print





