


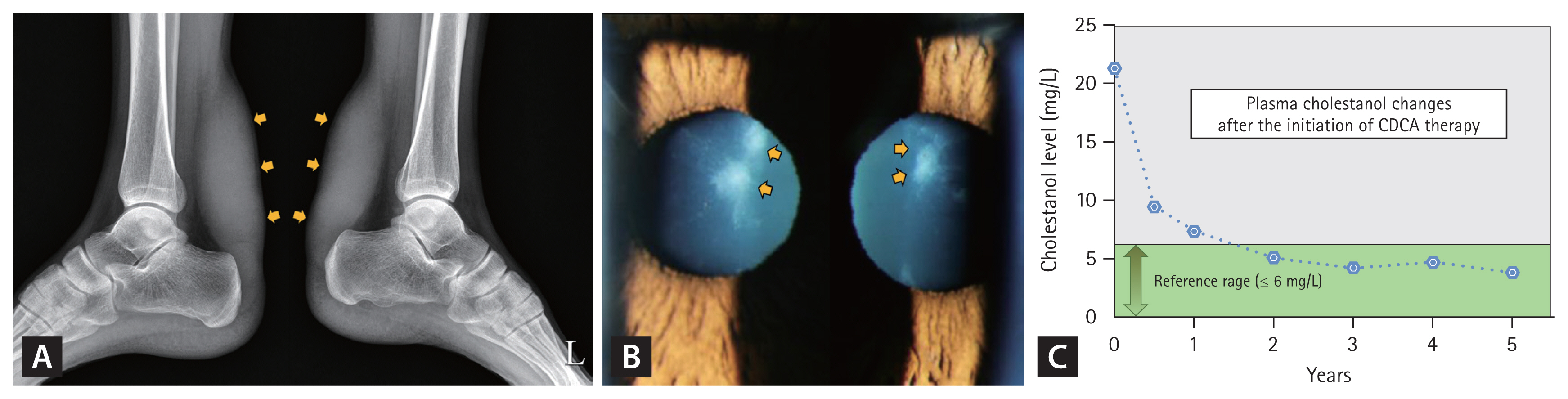
A 24-year-old man presented for lipid disorder evaluation before a repeat surgery for recurrent bilateral Achilles tendon xanthomas, which caused pain during walking (Fig. 1A). The patient underwent surgery for the same condition 3 years earlier. His lipid profile was total cholesterol, 195 mg/dL; low-density lipoprotein cholesterol, 130 mg/dL; triglyceride, 158 mg/dL; and high-density lipoprotein cholesterol, 59 mg/dL. Cataracts were detected during a consultation for corneal refractive surgery a year earlier. This history prompted a referral to the ophthalmology department, where a slit-lamp examination revealed premature bilateral anterior (Fig. 1B) and posterior subcapsular cataracts, raising suspicions of cerebrotendinous xanthomatosis (CTX). CTX was confirmed by an elevated plasma cholestanol level (21.33 mg/L, reference value ≤ 6.0 mg/L) and a homozygous missense mutation in the mitochondrial sterol 27-hydroxylase (CYP27A1) gene. Chenodeoxycholic acid (CDCA) therapy at 250 mg thrice daily, along with the use of an HMG-CoA reductase inhibitor, resulted in a gradual reduction of cholestanol levels to normal levels over 2 years (Fig. 1C). No xanthoma recurrence, cataract progression, or other CTX-related neurologic manifestations were observed in the following 6 years. CTX results from CYP27A1 gene mutations, reducing CDCA production and increasing plasma cholestanol levels. Untreated CTX can significantly shorten life expectancy, limiting it to the 5th and 6th decades, with progressive neurological issues such as dementia and spinal cord paresis. The absence of cholestanol in routine lipid profile may hinder accurate CTX diagnosis even when xanthomas are present. Bilateral cataracts, which occur in over 80% of patients with CTX in their 20s, provide a crucial diagnostic clue, aiding the selection of the right medication and improving patient care. Additional evaluations are necessary when a routine lipid profile does not explain why clinical signs of a lipid disorder (e.g., xanthoma) are present. Early CTX diagnosis through an ophthalmologic examination enables effective CDCA treatment and prevents irreversible damage.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




 |
 |