


INTRODUCTION
Despite the increase of procedural volume of chronic total occlusion (CTO) percutaneous coronary intervention (PCI), CTO PCI is still considered one of the most challenging procedures, even with the development of new devices and advanced techniques [1]. In fact, the unique and complex features of CTO lesion, such as severe and diffuse plaque burden, negative remodeling of the vessel, and heavy calcification, are major obstacles for successful CTO PCI [2].
Due to the innate limitations of invasive coronary angiography, intravascular imaging (IVI) devices that can provide continuous cross-sectional image of a vessel, such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), were introduced to complement the procedure and improve clinical outcomes [3]. The use of IVI in CTO PCI, along with technical advancements, is acknowledged as a key contributor to recent progress and increased success rate of CTO PCI. Despite the potential advantages of IVI in CTO PCI, the prognostic impact of IVI-guidance and optimization in CTO PCI has been unclear due to limited evidence from randomized controlled trials (RCTs). Although several RCTs demonstrated the prognostic benefit of IVI in complex coronary artery lesions other than CTO [4ŌĆō7], only limited evidence exists regarding the prognostic benefit of IVI in CTO PCI [8ŌĆō10]. Therefore, the current review consists of three parts: 1) Potential benefit of IVI in CTO Interventions, 2) Current evidences, and 3) Future perspectives and ongoing trials.
POTENTIAL BENEFIT OF IVI IN CTO INTERVENTIONS
The fundamental purpose of IVI in PCI is for procedural optimization [3]. For this purpose, IVI can be used in both pre- and post-PCI phases [11]. In pre-PCI phase, IVI is used to assess lesion characteristics and to determine strategy of lesion preparation, stent size, and landing zone accordingly. In post-PCI phase, IVI is used to check whether stent is optimally implanted and for the presence of acute complications such as edge dissection or plaque/thrombus protrusion in the stented segment. Considering the complexity of CTO lesions, the use of IVI for these general purposes is even more emphasized. In addition, IVI can be used for identifying entry of CTO lesions, IVUS-guided puncture in case of angiographically ambiguous proximal cap, guidance in retrograde re-entry attempts, and confirmation of wire location (intraplaque vs. extraplaque tracking) after crossing [12]. Since OCT requires injection of contrast agents for image acquisition, which may extend dissection planes, IVUS is the preferred modality in the pre-PCI phase [13]. However, OCT can be useful to assess stent-related problems such as underexpansion, malapposition, or edge dissection and to optimize the stented segment(s).
Guiding wire crossing
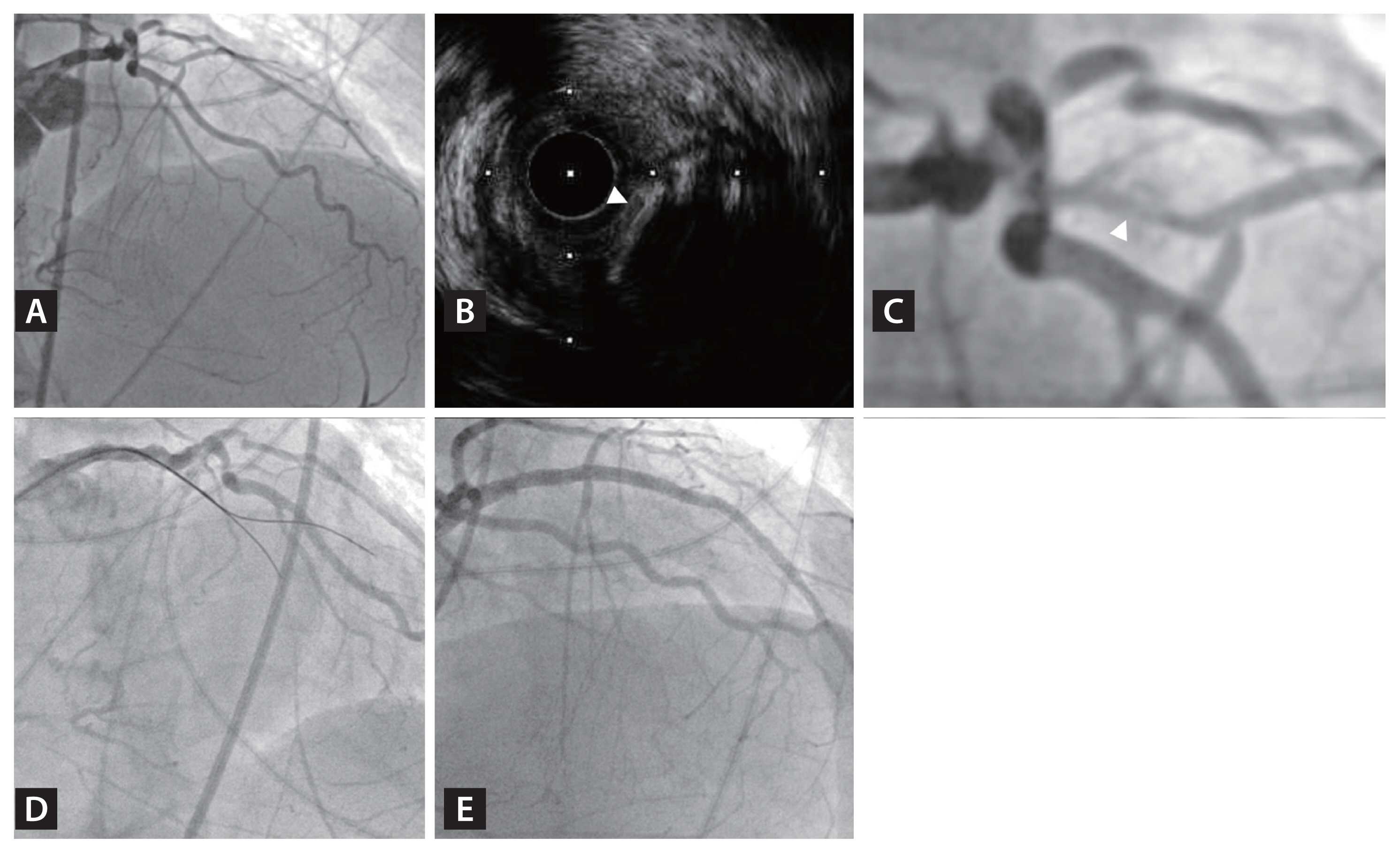
Ambiguous proximal cap in CTO lesion is estimated to account for approximately 30% of CTO PCI and is one of the major causes of wire crossing failure [14]. The low success rate in wire crossing through ambiguous proximal cap can be overcome through IVUS guidance. IVUS catheter is advanced to the side branch that diverges at the site of proximal cap of CTO lesion (Fig. 1). IVUS imaging can be obtained simultaneous real-time or intermittently to guide the location of proximal cap and guide wire [12]. Furthermore, IVUS image can provide additional information about plaque characteristics of the proximal cap, which can influence the choice of guide wire.
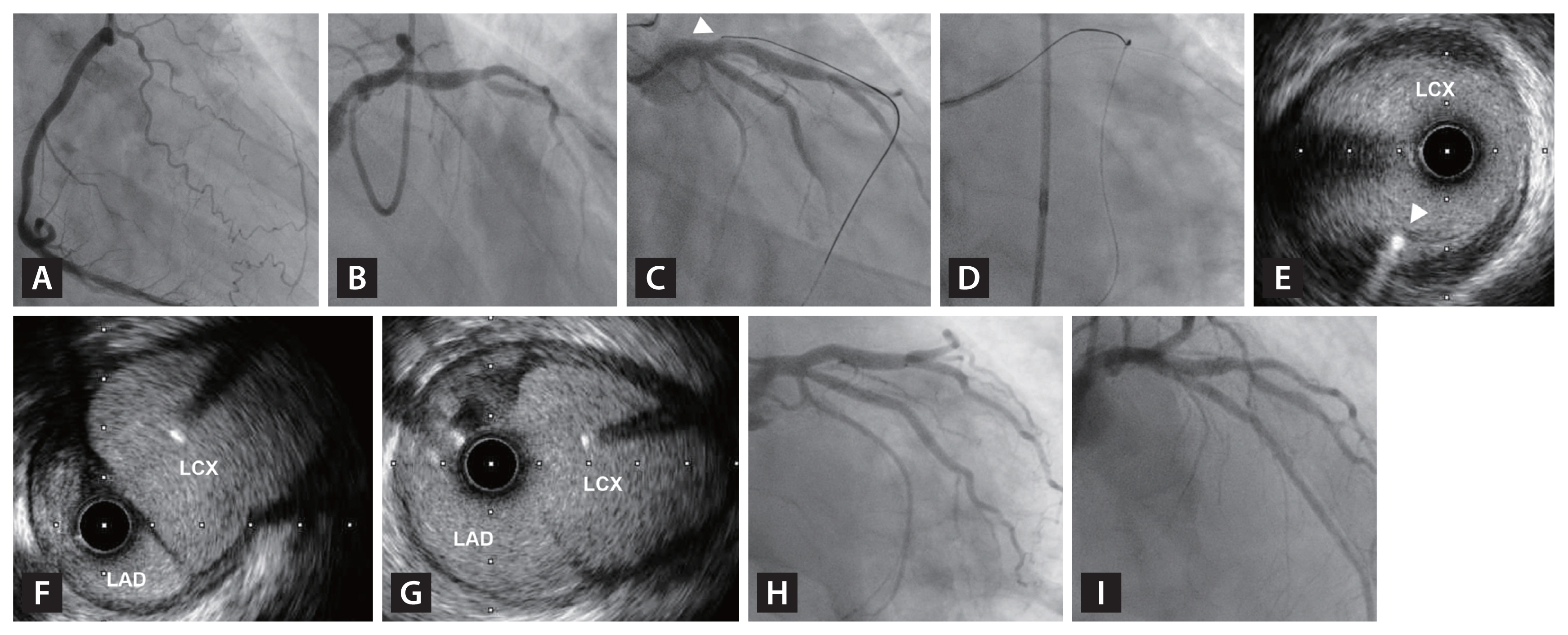
IVUS can also facilitate CTO lesion crossing in re-entry techniques (Fig. 2). With the emergence of advanced wire crossing techniques such as subintimal tracking and re-entry (STAR) and reverse controlled antegrade and retrograde tracking (CART), IVUS can play a key role in these techniques [13]. In these crossing techniques, IVUS can confirm the position of the guide wire (intraplaque vs. extraplaque) and provide information about vessel size to determine the appropriate balloon size in reverse CART to increase successful wire crossing and reduce the risk of perforation [15].
Intraplaque vs. extraplaque tracking
After successful wire crossing, IVI provides information about wire location (Fig. 3). Previous study presented that operator-reported tracking showed discordance with IVUS-detected actual wire tracking [16]. When interrogated with IVUS, unintended extraplaque tracking was noticed in nearly 90% in re-entry techniques and about 30% in antegrade or retrograde wiring in this study [16]. Extraplaque tracking may lead to vessel injury such as intramural hematoma and dissection, and side branch occlusion after recanalization [12,16]. Consequently, accurate identification of wire tracking has the possibility to reduce complications and improve clinical outcomes.
Lesion preparation, stent planning, and post-stent optimization
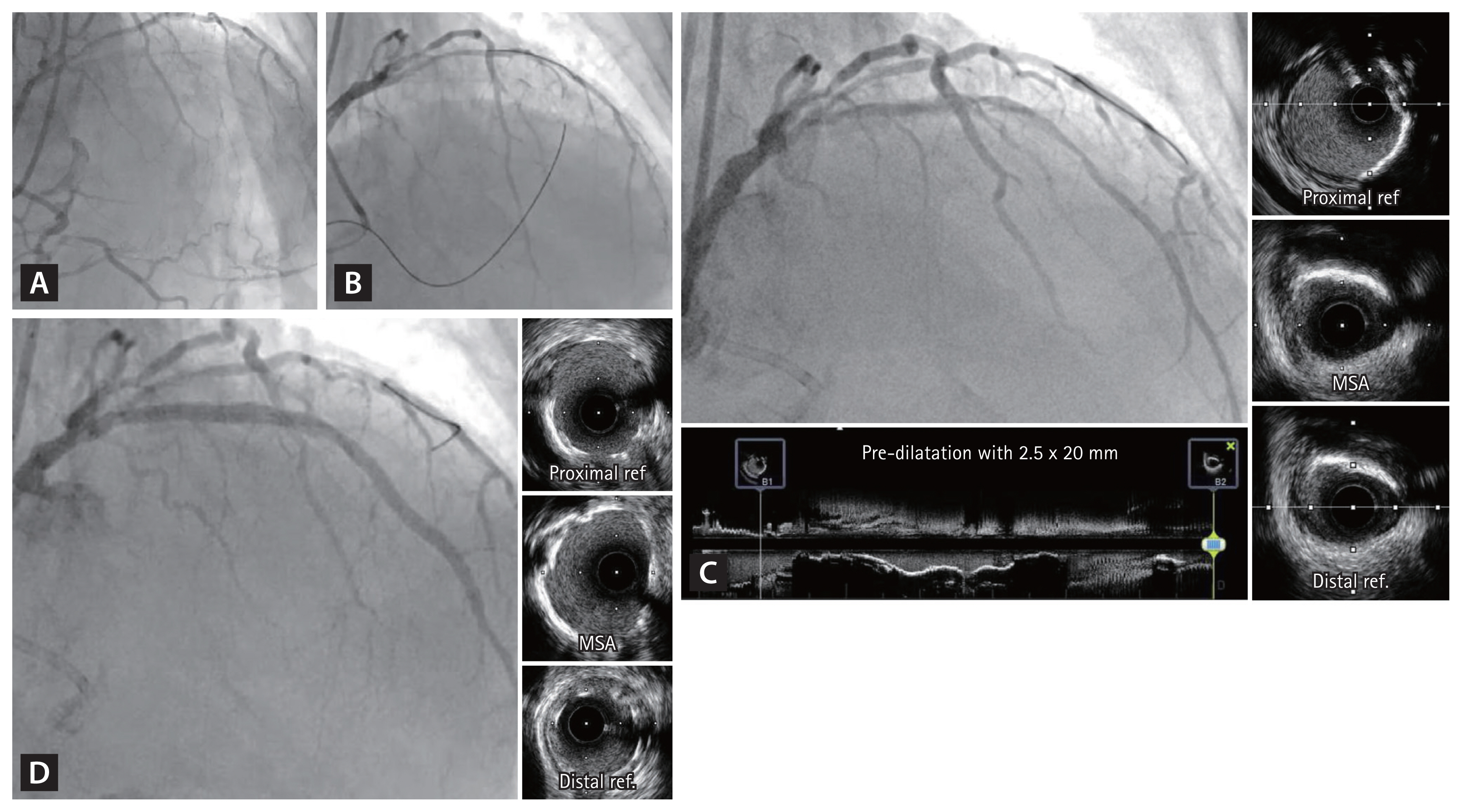
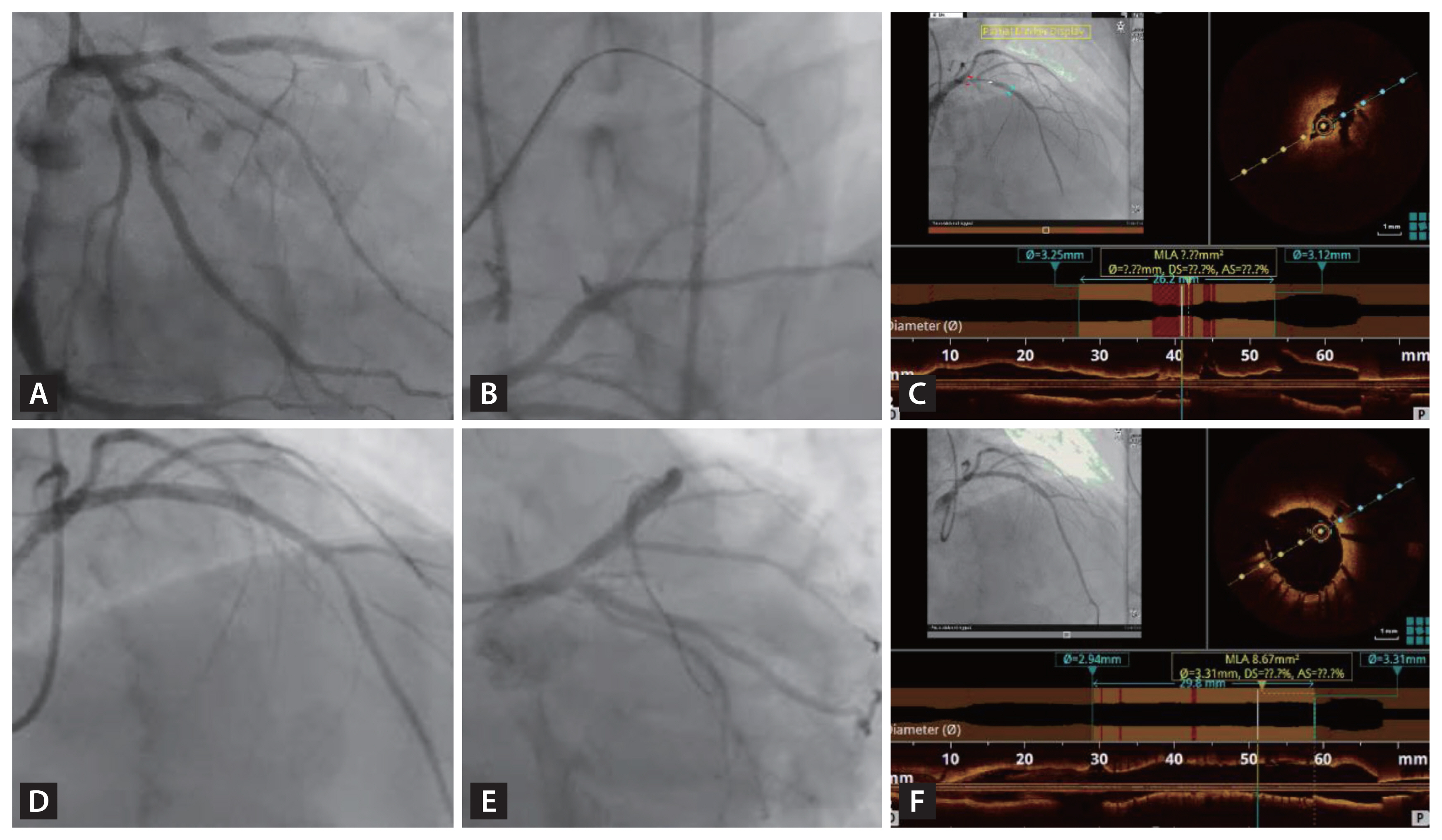
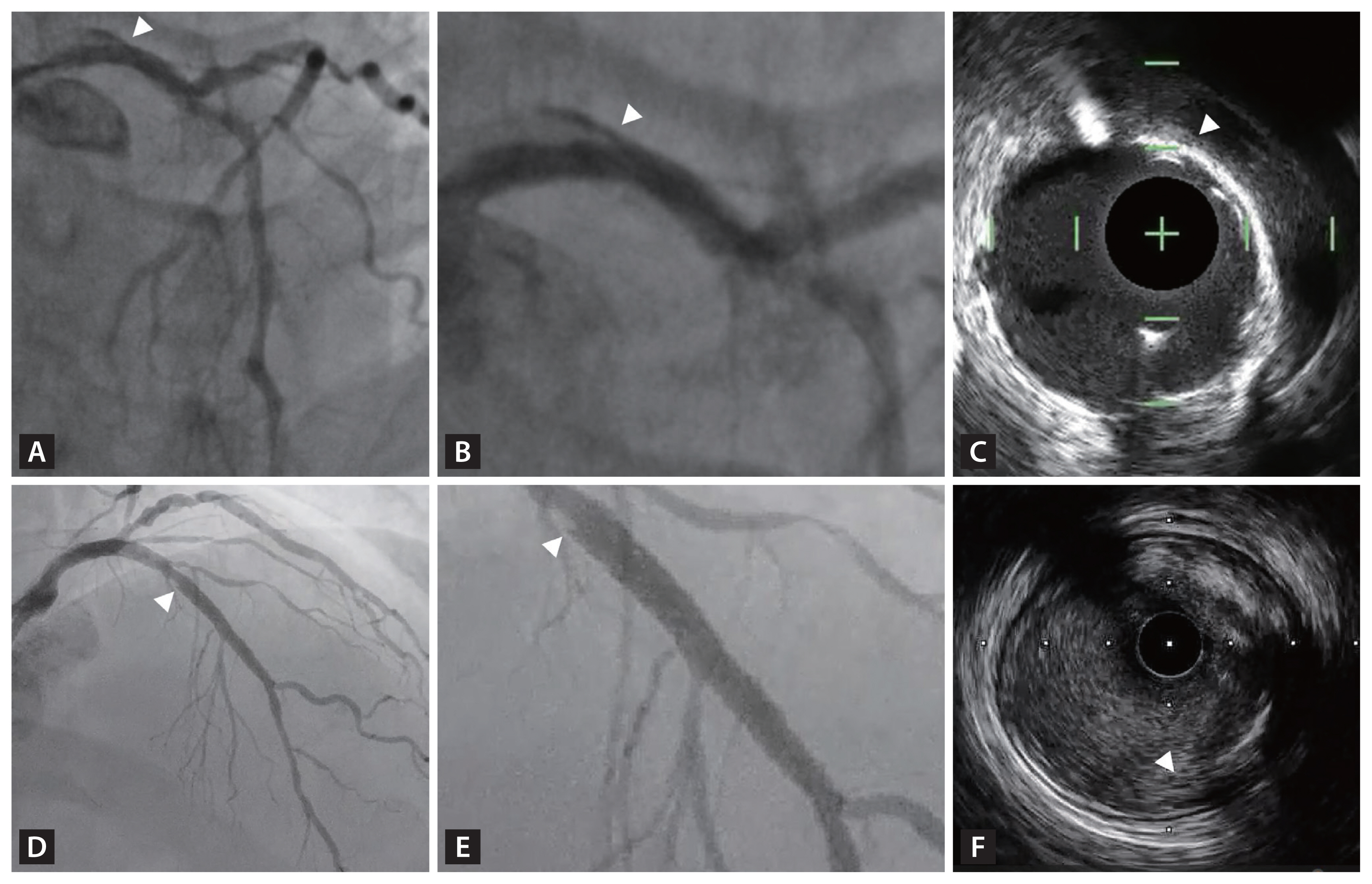
Principal roles of IVI during PCI of complex coronary artery lesions can also be applied to CTO PCI [11]. Prior to stent deployment, IVI is crucial to assess reference vessel size, lumen area, lesion length, and plaque characteristics, including composition and negative or positive remodeling [17]. This information can influence lesion preparation and plaque modification strategy. In addition, it can be used to determine the optimal stent size, length, and appropriate landing zone (Fig. 4). After stent implantation, IVI can be used to check for stent optimization and for the presence of acute procedure-related complications. Stent optimization is composed of sufficient stent expansion, absence of major stent malapposition to the vessel wall, and absence of major edge dissection (Fig. 5, 6) [7,11]. Successful achievement of stent optimization has been reported to be associated with better clinical outcomes [7,18].
CURRENT EVIDENCE
Several non-randomized studies and RCTs have evaluated the effectiveness of IVI compared to angiography alone in CTO PCI. In this section, results of previous studies are summarized. Although there have been limited number of RCTs, study-level meta-analysis revealed the prognostic benefit of IVI-guided PCI than angiography-guided PCI in CTO procedure.
Non-randomized study for prognostic benefit of IVI-guided CTO PCI
Non-randomized studies that evaluated the role of IVI in CTO PCI are summarized in Table 1 [16,19ŌĆō26]. Most studies were retrospective analyses. In terms of IVI modality, 6 studies used IVUS, 1 study used OCT, and the 2 remaining studies used both IVUS and OCT. In these retrospective studies, clinical outcomes assessments were limited to index hospitalization and showed no significant differences in in-hospital mortality between the IVI-guided and angiography- guided PCI groups. Maknojia et al. analyzed 33,345 patients from Nationwide Inpatient Sample (NIS) database who underwent CTO PCI from 2015 to 2018 [25]. In this study, only 8.8% of the total population used IVI for CTO PCI, and in-hospital mortality was similar between patients who did and did not receive IVI during CTO PCI (1.5% vs. 1.3%, p = 0.195). Another study from the PROGERSS-CTO registry which enrolled 8,771 patients from 39 centers in a retrospective manner, the use of IVUS was associated with higher technical (99% vs. 96%, p < 0.001) and procedural success rates (96% vs. 95%, p = 0.002). Unfortunately, these results did not translate into better prognosis, and in-hospital major adverse cardiovascular events (MACE) were comparable (2.04% vs. 1.62%, p = 0.176) between the IVI-guided PCI group and angiography-guided PCI group [26]. Similarly, Kalogeropoulos et al. [24] compared a composite endpoint of all-cause death, myocardial infarction, and target-vessel revascularization during median follow-up of 49 months among propensity matched 364 patients, but there was no significant difference in the risk of the composite endpoint between IVUS-guided and angiography-guided PCI group (13.7% vs. 15.9%, log-rank p = 0.67). However, as these studies had non-randomized design with short follow-up duration, the results should be interpreted with caution. Indeed, patients with more complex CTO lesions were more likely to use IVI in these studies. For example, patients in the IVI-guided PCI group had higher J-CTO score than angiography-guided PCI group, which limits the interpretation of these results [21,26].
Randomized trials for prognostic benefit of IVI-guided CTO PCI
Of the 3 RCTs that compared the effectiveness of IVI in CTO PCI to date, 2 RCTs showed that IVI-guided PCI improved clinical outcomes than angiography-guided PCI, and the other trial showed significantly better angiographic results with comparable clinical outcomes between the 2 groups (Table 2) [8ŌĆō10].
In the AIR-CTO (Angiographic and clinical comparisons of intravascular ultrasound-versus angiography-guided drug-eluting stent implantation for patients with chronic total occlusion lesions) trial, 230 patients were randomly assigned to either IVUS-guided or angiography-guided PCI groups [8]. IVUS-guided PCI significantly reduced in-stent late lumen loss compared to angiography-guided PCI (0.28 ┬▒ 0.48 mm vs. 0.46 ┬▒ 0.68 mm, p = 0.025), however, the rates of MACE (a composite of all-cause death, myocardial infarction, repeat revascularization, or stent thrombosis) at 2 years were only numerically lower in the IVUS-guided PCI group than the angiography-guided PCI group without statistical significance (21.7% vs. 25.2%, p = 0.641). However, it should be noted that this trial was not powered to show differences in clinical endpoint. In the CTO-IVUS (Chronic Total Occlusion InterVention with drug-eluting Stents guided by IVUS) trial, 402 patients were randomly assigned to IVUS-guided PCI or angiography-guided PCI groups. At 1 year, the risk of MACE (a composite of cardiac death, myocardial infarction, and target-vessel revascularization) was significantly lower in the IVUS-guided PCI than the angiography-guided PCI (2.6% vs. 7.1%; hazard ratio [HR] 0.35; 95% confidence interval [CI] 0.13ŌĆō0.97; p = 0.035) [9].
The recently published RENOVATE-COMPLEX-PCI (The Randomized Controlled Trial of Intravascular Imaging Guidance versus Angiography-Guidance on Clinical Outcomes after Complex Percutaneous Coronary Intervention) demonstrated for the first time that IVI-guided PCI for complex coronary artery lesions is superior to angiography-guided PCI in reducing the risk of target vessel failure (a composite of cardiac death, target-vessel myocardial infarction and target-vessel revascularization) among 1,639 patients with complex coronary artery lesions [7].
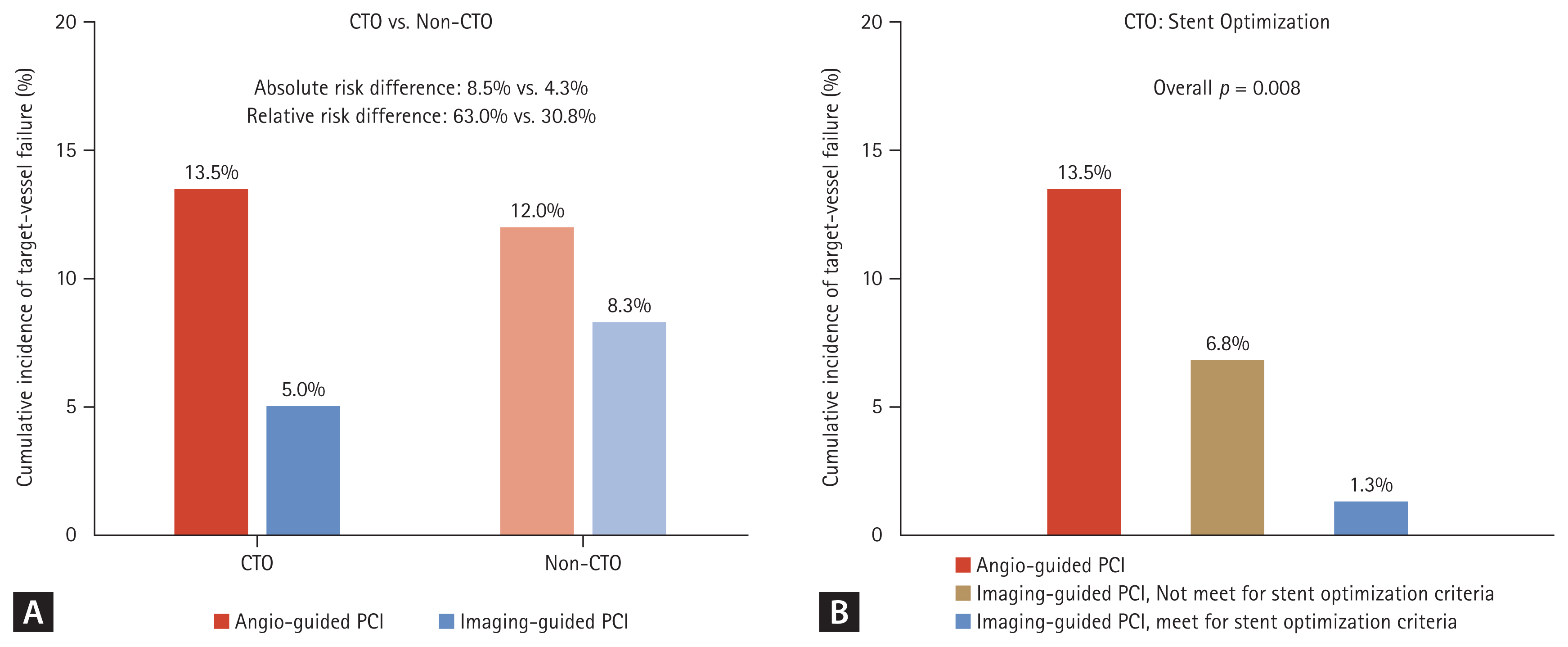
A prespecified substudy of the RENOVATE-COMPLEX-PCI exclusively evaluated 319 patients who underwent CTO PCI [10]. Among patients with CTO, angiographic and procedural characteristics including J-score (median J-CTO score: 2.0 [1.0ŌĆō3.0] vs. 2.0 [1.0ŌĆō3.0], respectively, for IVI-guided and angiography-guided PCI; p = 0.755) were similar between the IVI and angiography-guided PCI groups. At a median follow-up of 2.1 years (interquartile range 1.1ŌĆō3.0 yr), the risk of target vessel failure was not significantly different between patients with CTO and non-CTO lesions (7.6% vs. 9.6%; HR 0.797; 95% CI 0.505ŌĆō1.258, p = 0.331). Among patients with CTO, the risk of target vessel failure was significantly lower in the IVI-guided PCI group than in the angiography-guided PCI group (5.0% vs. 13.5%; HR 0.303; 95% CI 0.130ŌĆō0.710, p = 0.006). When patients were classified according to the presence of CTO and the use of IVI, the risk of TVF was significantly different among the 4 groups, and the risk of target vessel failure was the highest in CTO patients treated by angiography-guided PCI and the lowest in CTO patients treated by IVI-guided PCI (Fig. 7). These results suggest that among various complex coronary artery lesions subsets, the efficacy of IVI-guided PCI is relatively higher in CTO intervention.
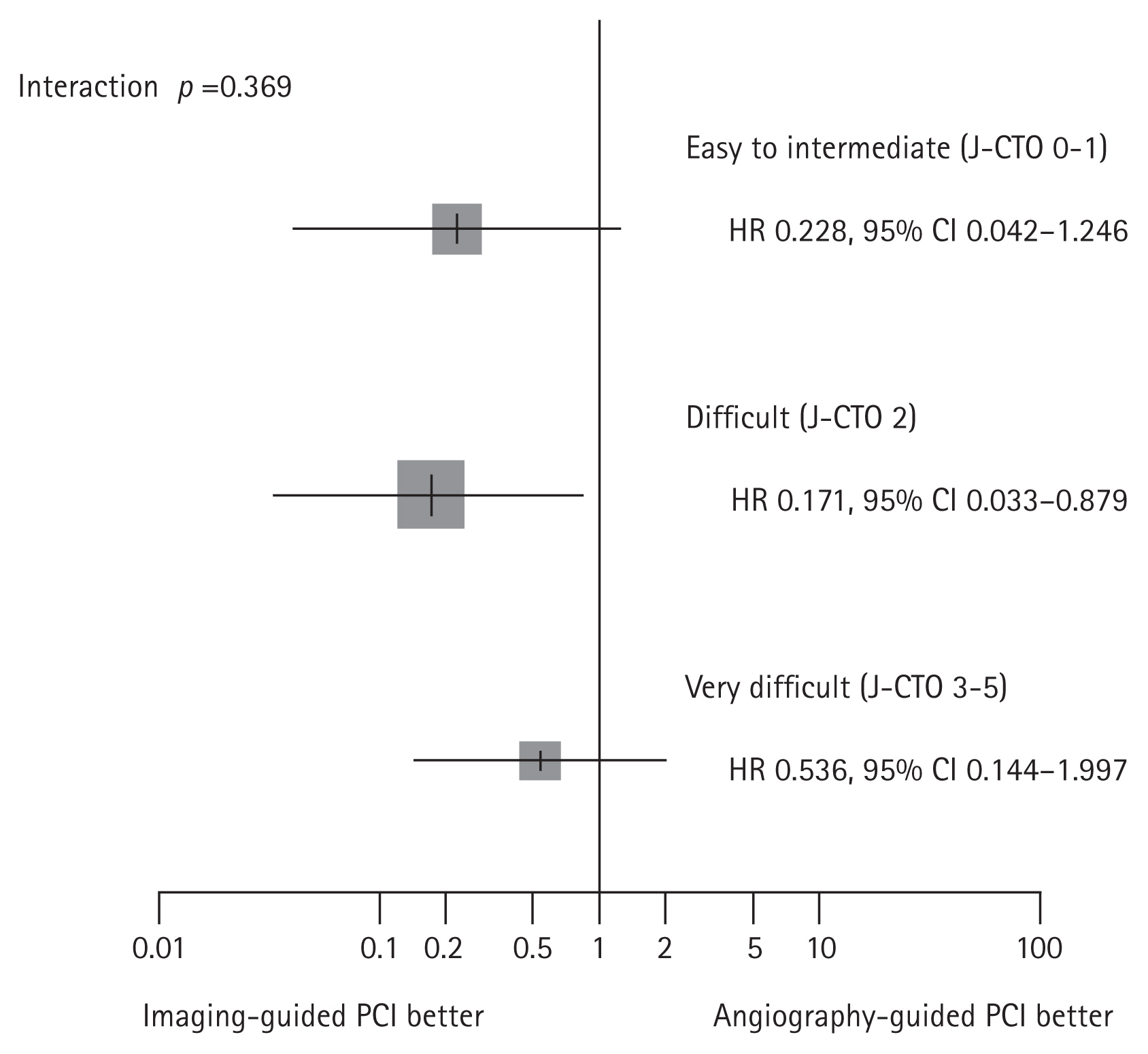
Furthermore, the risk of target vessel failure was shown to gradually increase from patients with IVIŌĆōguided PCI and stent optimization, patients with IVIŌĆōguided PCI but no stent optimization, and patients with angiography-guided PCI (1.3% vs. 6.8%, 13.5%, overall p = 0.008) (Fig. 7). These results imply that both IVI use and achieving stent optimization in CTO PCI is important for patientŌĆÖs prognosis. In addition, the benefit of IVI was consistently found in subgroups divided by lesion complexity assessed by J-CTO score (Fig. 8).
Meta-analysis of CTO PCI using RCTs
Since previous RCTs showed conflicting results regarding prognostic impact of IVI-guided PCI in CTO intervention [8ŌĆō10], study-level meta-analysis was performed by the current authors. A total of 951 patients who were randomly assigned to IVI-guided PCI (n = 536) or angiography-guided PCI (n = 415) were evaluated. In random effects model, IVI-guided PCI had significantly lower risk of a composite outcome of cardiac death, myocardial infarction, and target vessel revascularization than angiography-guided PCI in CTO intervention (relative risk 0.49; 95% CI 0.25ŌĆō0.95; p = 0.034). Individual components of the composite outcomes showed similar trends, with statistical significance only met in target vessel revascularization (Fig. 9).
FUTURE PERSPECTIVES AND ONGOING TRIALS
Currently, there are 2 ongoing studies with a relatively large number of patients regarding the impact of IVI in CTO PCI (Table 3). CRUISE-CTO trial (To Evaluate Whether IVUS-guided Drug-eluting Stent Implantation Leads to Better Clinical Outcomes Compared to Conventional Angiography in the Treatment of Chronic Complete Occlusion Disease, NCT04944615) will enroll 1,448 patients with CTO and compare the risk of MACE (a composite of death, myocardial infarction, definite or probable stent thrombosis, and clinically-driven target vessel revascularization) between IVUS-guided PCI vs. angiography-guided PCI. FWCTO registry (CTO Registry From Insight of IVUS in Fuwai Hospital, NCT03461367) is a prospective observational study and will enroll 5,000 patients who underwent CTO PCI with or without IVUS-guidance and optimization.
In addition, there are multiple RCTs which will evaluate the prognostic impact of IVUS or OCT-guided PCI compared with angiography-guided PCI in all-comers with complex coronary artery lesions including CTO. The IMPROVE (IMPact on Revascularization Outcomes of IVUS Guided Treatment of Complex Lesions and Economic Impact, NCT04221815) and IVUS-CHIP (Intravascular Ultrasound Guidance for Complex High-risk Indicated Procedures, NCT04854070) trials will enroll all-comers with complex coronary artery lesions and evaluate IVUS-guided PCI. The OCCUPI (Optical CoherenCe Tomography-gUided Coronary Intervention in Patients With Complex lesIons: a Randomized Controlled Trial, NCT03625908) is currently ongoing and will compare OCT-guided PCI versus angiography-guided PCI in similar populations including CTO.
These trials are expected to provide more definite answers regarding the prognostic benefit of IVI in CTO PCI. Moreover, it would be a very interesting and clinically relevant topic to evaluate whether CTO PCI, when optimally performed using IVI, can improve patient prognosis compared to medical treatment alone. Simultaneously, efforts should be made to educate and train cardiac catheterization laboratory staff and physicians in the use of IVI in CTO PCI to promote broader use and improve outcomes for their patients.
CONCLUSION
IVI, especially IVUS, can be used to facilitate guide wire crossing and stent optimization in CTO PCI. Meta-analysis of RCTs conducted to date showed that IVI-guided PCI in CTO lesions significantly improves patientsŌĆÖ prognosis than angiography- guided PCI, supporting the use of IVI in CTO PCI. Further large-scaled trials are warranted to consolidate the benefit of IVI-guidance and procedural optimization in CTO PCI and to facilitate the widespread use of IVI in CTO PCI.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





