A Clinical Consideration of Systemic Embolism Complicated to Infective Endocarditis in Korea*
Article information
Abstract
Objectives
Infective endocarditis is still one of the important fatal diseases in Korea, especially when systemic embolisms are supervene. So, identification of patients who are in the high risk of embolism and who can be helped by early surgical intervention is very important. Considering these, we tried to elaborate the risk factors for the systemic embolism in patients with an infective endocarditis and the influence of systemic embolism on the mortality and morbidity in patients with an infective endocarditis.
Methods
We retrospectively reviewed the clinical records of 97 patients who were admitted with the infective endocarditis between January 1983 and October 1993.
Results
Among 97 patients, 80 patients met our diagnostic criteria. The mean age of patients was 38 years old. There were 43 males and 37 females. The mean duration of fever since the fever developed by history was 38 days. Valvular heart disease was the most frequent underlying heart disease. Mitral regurgitation and aortic regurgitation were the most common among valvular heart diseases. Pneumonia and acute pharyngotonsillitis were the most frequent predisposing factors of infective endocarditis. Blood cultures were positive in 51 patients (63.8%). Streptococcus viridans was the organism isolated most frequently, and Staphylococcus aureus was the second most frequently isolated one. Vegetations were detected in 58 patients (76.3%) by an echocardiography. Mitral valve and aortic valve were the most frequently involved. Incidence rate of embolism was 50% and the most frequent embolism site was the central nervous system and extremities were the next. Embolism occurred at the mean of 37 days after onset of fever. Overall in-hospital mortality rate was 26.3% and a cardiac-origin was the major cause of death. The only statistically significant risk factor for mortality was systemic embolism. The analysis of the relation between an incidence of embolism and the multivariables (age, presence of vegetation, location of vegetation, size of vegetation, causative organisms) showed that only the growth of Staphylococcus aureus had a significant trend toward a risk of subsequent systemic embolism.
Conclusion
This study suggests that systemic emboli increases the mortality rate in patients with infective endocarditis. Age of patients, presence of vegetation, size and location of vegetation are not the risk factors for embolism, while certain organism, especially Staphylococcus aureus, could be a risk factor for the systemic embolism.
INTRODUCTION
In recent years, the prognosis of patients with an infective endocarditis has improved as a result of advanced diagnosis, better antimicrobial therapy, earlier detection and surgical management of complications. In Korea, however, the infective endocarditis is one of the important fatal diseases1), and especially systemic embolism is one of the common and serous complications associated with the infective endocarditis18). Because embolisms can result in an irreversible organ dysfunction or death, prevention of embolisms and elective valve replacement in patients at high risk of embolism has been recommended. But which patients are more susceptiable to the embolism and which patients are at the high risks of systemic embolism are the questions which need further investigation. So, identification of patients who are at the high risk of systemic embolism is very valuable to prevent an irreversible organ damage or death from the infective endocarditis.
Echocardiography, particulary two dimentional echocardiography with color flow image and Doppler study, is useful in diagnosing an infective endocarditis. These methods help to detect vegetations on the heart valves or other lesions and also to demonstrate, without invasive investigation, serious hemodynamic alternations and serious structural damage requiring surgical treatment. Valvular vegetations are visualized by echocardiography in 42% to 86% of cases2, 3, 15–17), the prescence or larger size of vegetation has been considered to increase the risk for embolic events4–6, 19).
We did a retrospective study to determine the risk factors for the development of systemic embolism in patients with an infective endocarditis and also to assess the influence of the systemic embolism on the mortality and the morbidity in patients with an infective endocarditis.
MATERIALS AND METHODS
1. Study Groups
We retrospectively reviewed the medical records of 97 patients who had bean admitted with an infective endocarditis in Kangnam St. Mary’s Hospital, St. Mary’s Hospital and St. Paul’s Hospital from January 1983 to October 1993. Among 97 patients, 80 patients met at least one of the following diagnostic criteria for an infective endocarditis.
1) a direct evidence of an infective endocarditis at surgery or culture of embolus(14 patients).
2) two or more positive blood culture with three or more of the following conditions: presence or fever(â38°C), underlying heart disease, new regurgitant murmur, systemic embolism, vegetations(31 patients).
3) positive blood cultures with fever, underlying heart disease or new regurgitant murmur(23 patients).
4) negative blood cultures with fever, underlying heart disease, vegetations or systemic embolism(12 patients).
2. Echocardiography
Among 80 patients, 76 patients went through technically adequate echocardiographic examinations. M-mode and two-dimentional echocardiography with Doppler study was performed using Hewrett-Packard SONOS 1000 and 2.5 MHz transducer. Images were recorded on strip chart papers, pictures or videotape. A definite valvular vegetation was defined as a distinct echogenic mass associated with a valvular leaflet or supporting valvular structure. Maximal length and width of vegetations were measured by either freeze-frame videotape analysis or the picture analysis with a ruler. Valvular regurgitation was assessed by Doppler pulsed wave mapping.
3. Embolisms
An embolic event was defined as the acute onset of organ system dysfunction consistent with ischemia, based on objective changes found during physical examination or on serial laboratory and radiologic studies. Cerebral embolisms were confirmed by brain CT; peripheral embolisms by arterial angiography, pulmonary embolisms by serial chest PA and lung perfusion scan, kidney and splenic infarctions by sonography. But immune complex phenomena, microvascular emboli such as cutaneous microinfarctions and embolisms occurred before admission were not included.
4. Data Analysis
Factors associated with the embolism and the mortality were determined using chi-square test and Fisher’s exact test(two-tail). Stepwise multiple logistic regression analysis was used to determine the risk factors for mortality. Significant statistical analysis was established at P-value less than 0.05.
RESULTS
The patients’ clinical characteristics are summarized in Table 1. The age range of 80 patients was 11 to 73 years(mean age ± SD: 38 ± 17 years). There were 5 patients aged below 15 years and 24 patients aged above 50 years. There were 43 males and 37 females. The mean duration of fever was 38 ± 31 days(range: 3 to 130 days). The embolic events occurred at the mean of 37 days after fever had developed. The most frequent subjective symptoms were fever, chilling, dyspnea and cough, while the most frequent physical signs were murmur, fever, hepatosplenomegaly and rale. In laboratory findings on admission, leukocytosis, hematuria, proteinuria and anemia were the most frequent ones(Table 2).

Clinical Characteristics of 80 Patients
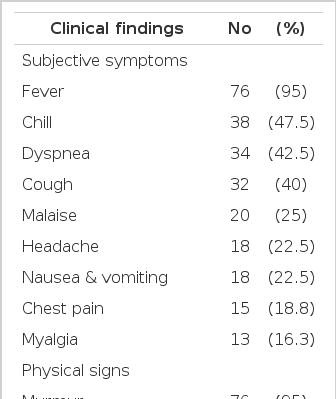
Symptoms, Signs and Laboratory Findings on Admission
Valvular heart disease(50 cases, 62.5%) was the most frequent underlying heart lesion and, among them, 12 cases were confirmed to rheumatic origin and 38 patients had either mitral regurgitation(n=20) or aortic regurgitation(n=18). 16 cases(20%) had congenital heart diseases, of which the most common cause was ventricular septal defect(9 cases, 11%). 7 cases(8.8%) had mitral valvular prolapse, while 2 cases had endocarditis on the prosthetic valve, and 2 patients had had an endocarditis in the past(Table 3).

Underlying Heart Disease
The definite predisposing factors could be identified in 44 patients(55%). Of these, pneumonia and acute pharyngotonsillitis accounted for a large number of cases(11 and 10 respectively). A history of dental manipulation or periodontitis was associated in 8 patients(18.2%) and postabortal sepsis or puerperal sepsis accounted for only 2 cases(4.5%). Otitis media, chronic renal failure with hemodialysis, aplastic anemia, and pyoarthritis were revealed to be a predisposing factor of infective endocarditis, respectively (Table 4).
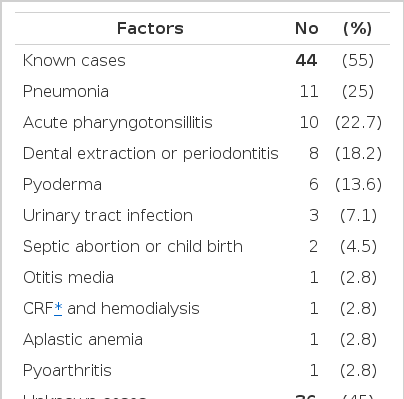
Predisposing Factors
Blood cultures were positive in 51 patients (63.8%), and streptococcal species constituted the largest number of isolates(25 cases, 50%), followed by staphylococcal species(17 cases, 34%). Streptococcus viridans(20 cases) and Staphylococcus aureus(12 cases) were the major isolated organisms. Gram negative organisms were isolated in 8 cases(16%), of which Klebsiella and Salmonella were isolated in 2 cases each(Table 5).

Causative Organisms
Technically adequate echocardiogram, were obtained in 76 of 80 patients. Vegetations were detected in 58(76.3%) out of 76 patients, and there was a total of 83 vegetations. Of involved valves of vegetations, mitral valves and aortic valves were the most frequently involved valve and 6 patients had both aortic and mitral valve involvement. There were 6 extravalvular vegetations (2 in the right ventricular outflow tract and 2 in the interventricular septum) (Table 6).

Sites of Vegetations
Among 58 patients who had the vegetations through the echocardiogram, 37 patients had the measurable vegetations of 52. Of these, size of vegetations ranged from 5 to 25 millimeter and 17 patients had vegetations with a long diameter below 10 millimeter, while 20 patients had vegetations larger than 10 millimeter in diameter (Table 7).

Size of Vegetations
Embolic events occurred at 50 sites in 40 patients(50%). The locations of embolisms were central nervous system(26 cases), lower extremity(11 cases), kidney(4 cases), lung(3 cases), upper extremity(2 cases), spleen(2 cases) and coronary vessel(2 cases)(Table 8).
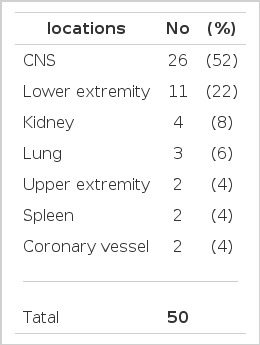
Locations of Embolism
There were 21 deaths which resulted in overall in-hospital mortality of 26.3%. Cardiac-origin secondary to congestive heart failure, acute myocardial infarction and conduction block were the major cause of deaths in 8 patients(38%). 3 patients had ventricular tachyarrhythmias. Cerebral hemorrhage, including mycotic aneurysmal rupture, cerebral infarction, sepsis and multiorgan failure, was found to be the cause of the deaths of 2 patients. 2 patients died suddenly(Table 9).
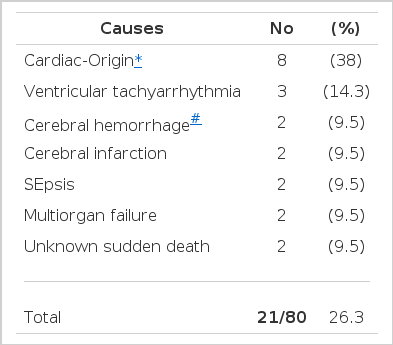
Causes of Death
Table 10 shows that the embolism was the only statistically significant risk factor related to mortality and it’s relative risk was 3.2. Presence of vegetation, locations of vegetation, size of vegetation, causative organisms and operation were not associated with an increased Table 11 shows the relation of multivariables(age, presence of vegetation, location of vegetation, size of vegetation, and causative organisms) to incidence of embolism. Of 40 patients with systemic embolisms, 11 patients’ age was over 50 years, 30 patients had one or more vegetations. 21 patients had vegetations on mizal valve, 9 patients on aortic valve; 11 patients had vegetations with size over 10 millimeter in diameter. Streptococcus viridans were isolated in 10 patients and Staphylococcus aureus in 9 patients. There was a trend toward a greater risk of subsequent systemic embolism in patients with Staphylococcus aureus infection. However, this trend was not statistically significant.

Risk Factors for Mortality
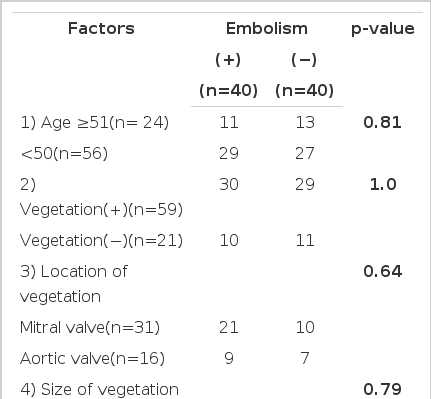
Risk of Embolism
DISCUSSION
We examined 80 consecutive cases of infective endocarditis seen over a 10 year period. Clinically our report is different from the reports from western countries, India and Taiwan. The majority of the reports from the western countries can be summarized as follows: older age of patients7), less the mortality and the incidence of infective endocardits caused by the rheumatic heart disease12) more frequent Staphylococal endocarditis8), more association with intravenous drug abuser9–11), mitral valve prolapse and prosthetic valve8,9) and so forth. According to a recent report from India(developing country), most of patients were young, and a large number of patients had underlying rheumatic heart disease, and puerperal sepsis were the most common predisposing factor. Staphylococcus aureus was the most frequent causative organism, an echocardographic detection rate of vegetation was 63%, and overall mortality rate was 25%13). Our result is similar to Taiwan in many aspects14). For example, age distribution, mean age, sex ratio, clinical features, major infecting organisms, detection rate of vegetation, ivolved valves, mortality rate, and cause of death in our study are similar to those of Taiwan’s report14), but underlying heart disease, predisposing factors, and embolic rate are different. During the analysis, there were a lot of difficulty confirming rheumatic heart disease as an underlying cause of infective endocarditis. Although infective endocarditis originated from rheumatic heart disease was confirmed at only 12 patients(15%) in our study because of poor methods to confirm, we suspect that more patients could be classified as infective endocarditis originated from rheumatic heart disease, which might be similar level to those of India and Taiwan13,14). In our study of 80 patients with infective endocarditis, 76.3% had an echocardiographic vegetation. The prevalence of vegetations detected by echocardiography in previous studies ranged from 42% to 86%15–17). The detection rate depend on the group of patients studied, the echocardiographic methods used and echocardiographic abnormalities defining a vegetation. We define vgetation when we saw specific findings of vegetation on echocandiography. All the studies regarding the relationship between echocardiographic features of vegetations and the risk of embolism are difficult to interpret because of the small number of patients in all series, the varying definition of embolism and inclusion of patients who have already had an embolism by the time echocardiography was performed because most of the hospitals were tertiary referral centers. In our analysis, however, embolic event was defined clinically and radiologically, and combolic episodes to skin and embolisms occurred before admission were excluded because they did not contribute directly to the morbidity and the mortality. Several studies have reached conflicting conclusions about the relation between the echocardiographically visualized vegetations and the frequency of embolic events in endocarditis, some suggesting an association3) but others not16,17). According to some studies, the incidence rate of embolism was at least two times as high in the group with the vegetations ≥ 10 millimeter as in the group with no vegetation or the vegetations <10 millimeter18,19), but other studies showed that echocardiographically measured size of vegetation and systemic embolisms have no relationship to each other20). Our results also did not show the significant relationship between vegetation’s presence or it’s size and systemic embolism.
The overall in-hospital mortality rate of 26.3% for patients with infective endocarditis is considerably higher than that of western countries(10%)18), and almost equal to those of India, Taiwan, and the other Korean study (25%, 22%, 23.3% respectively)13,14,1). Although early diagnosis, and proper antimicrobial therapy might decrease death rate, early surgical intervention to high risk patients might be a major factor for this difference. In fact, more recent series suggested that mortality could be reduced to 10 to 13% by surgical intervention. This was specially so in patients with congestive heart failure whose survival had been shown to improve through timely valve replacement21,22).
The major risk factor for mortality was a systemic embolism and its relative risk was 3.2, and embolisms occurred an average 37 days after onset of fever in our study, those are similar to other reports18,23). The major causes responsible for the deaths in 12 patients(55%) were cardiac-origin secondary to congestive heart failure, acute myocardial infarction, conduction block and irreversible, catastrophic cerebral infarction or hemorrhage.
Infective endocarditis has changed its distribution and frequency during the last 5 decades from the viewpoint of infection organisms. Before the antibiotic era, infective endocarditis was almost universally lethal, and staphylococci were responsible for less than 10% of cases. The introduction of antibiotics changed the pattern and increased the frequency of staphylococci as a causative agent. During the last 2 decades in western countries, prosthetic hart valve and intravenous drug abuse have become common and contributing factors to the increasing proportion of patients with staphylococcal infective endocarditis8,11,24). Staphylococcal infective endocaritis frequently involves native valves, causes rapid destructive changes on valves and has metastatic foci, so it has been condisered as a malignant disease, requiring aggressive medical therapy and urgent surgical intervention. In recent papers, embolic complication is recognized in 12 to 35 percent of patients during the course of subacute bacterial endocarditis by Streptococcus viridans and in 50 to 60 percent with acute bacterial endocarditis by Staphylococcus aureus26,27). In our analysis, the relationship between growth of Staphylococcus aureus and systemic embolism was not singificant statistically, but in trend analysis using kappa method showed Staphylococcus aureus infective endocarditis had significant trend toward a systemic embolism than other organisms. So only the growth of Staphylococcus aureus was thought to be a possible risk factor for embolization. Recent another study of patients with endocarditis has reported that the observed rate of emboli was highest among patients with Staphylococcus aureus endocarditis, with an overall rate 2.4-fold greater than the rate among patients with Streptococcus viridans endocarditis, irrespective of vegetation status2). The reasons why the infective endocarditis by Staphylococcus aureus are more susceptible to embolization than that by Streptococcus viridans are not readily explained. But Staphylococcus aureus produces and secretes a number of specific enzymes and toxins, including coagulase & clumping factor, lipase, hyaluronidase, staphylokinase, and cytotoxic α-toxin, which have been variously implicated as possible pathogenic factors and never existed in Streptococcus viridans28). So these products are supposed to be the important factors responsible for bacterial adherece, invasion, destruction, interference with host defence mechanism, coagulation & fibrinolysis, and septic metastasis within the valves infected by Staphylococcus aureus. Therefore the patients who had Staphylococcus aureus infective endocarditis with definite vegetation should be considered to have early surgical intervention.
In conclusion, this study suggests that systemic emboli increases the mortality rate in patients with infective endocarditis. Age of patients, presence of vegetation, size and location of vegetation are not the risk factors for embolism, while certain organism, especially Staphylococcus aureus, could be a risk factor for systemic embolism.
Study limitation: We were able to count only those arterial emboli that resulted in clinically detectable signs and symptoms and were later confirmed by radiologic or laboratory studies. There was possibility that additional subclinical or silent emboli of small size may have occurred in some patients. There was, however, no readily apparent way to detect such emboli and, from a clinical perspective, such emboli wre inconsequential. In many studies, to exclude intra-observer and inter-observer variability, a blinded observer reviewed the echocardiograms for the presence and size of vegetations and the severity of the valvular regurgitation2,16,18). But our study could’t be confirmed by the blinded observer.
In addition, our data is to some extent biased by the referral nature of our hospital, in which patients with more complicated cases are admitted.
Acknowledgments
We would like to thank Mr. Jeon Y J and Mr. Lee JH for their assistance in statistical anlgsis.