A case of blue rubber bleb nevus syndrome
Article information
Abstract
Blue rubber bleb nevus syndrome is a rare disorder that is characterized by multiple recurrent vascular malformations, such as hemangioma, and these primarily involve the skin and the gastrointestinal tract. It may also involve the brain, liver, lungs, and skeletal muscles. A 14-year-old female visited our hospital with a chief complaint of dizziness; upon examination, we found multiple recurrent hemangiomas on the skin and gastrointestinal tract. We were able to diagnose her as suffering from blue rubber bleb nevus syndrome and we treated her with methylprednisolone (2 mg/kg/day for 1 month and 1 mg/kg/day for additional 3 months). We report on this case along with a review of the literature.
INTRODUCTION
Blue rubber bleb nevus syndrome (BRBNS) is a rare disorder which is characterized by multiple recurrent vascular malformations, such as hemangioma, and these primarily involve the skin and gastrointestinal tract1). BRBNS may also involve the brain, liver, lung and skeletal muscles1, 2).
The most common clinical presentation of BRBNS is iron deficiency anemia which is caused by bleeding from a vascular malformation in the gastrointestinal tract. There was occult bleeding In most of the reported cases, but bleeding that presented in the form of melena or hematochezia has also been noted3). Although about 200 cases of BRBNS have been reported in the English literature, there are currently no reports of any cases of BRBNS reported in the Korean literature, although there have been two cases reported in the English literature3, 4).
We report here of a 14-year-old patient with multiple recurrent hemangiomas on her skin and gastrointestinal tract; she was diagnosed with BRBNS and treated with methylprednisolone. We also include a review of the literature.
CASE REPORT
A 14-year-old female patient visited the Department of Gastroenterology at our hospital as an outpatient in October, 2005; her chief complaint was dizziness that had initially developed 18 months ago. She was hospitalized for evaluation in December, 2005. She denied having melena, hematochezia, menorrhagia or recurrent epistaxis. The patient did not have any medical history of non-steroidal anti- inflammatory drug use, peptic ulcer or chronic liver disease. Since infancy, the patient had repeatedly suffered from the recurrence of soft, compressible bluish nodules in the skin, and these nodules tended to refill with blood after compression. In order to treat these lesions, the patient had undergone a total of at least eight operations at our hospital and other hospitals. However, the nodules recurred on the patient's toe, right arm and the left hand in May, 2004 (Figure 1). Consequently, she was hospitalized in the Department of Orthopedics at our hospital, where excision and biopsy were performed, and the biopsy results revealed hemangioma. However, she had no family history of any recurrent skin lesions or gastrointestinal bleeding. At the outpatient clinic before admission, she had appeared pale with anemic conjunctivae; she had a blood pressure of 90/60 mmHg, a heart rate of 70/min and a body temperature of 36℃. There were no skeletal deformities. A digital rectal examination showed negative results. According to the laboratory examinations performed at the outpatient clinic, her hemoglobin was 5.9 g/dL and her hematocrit was 22.7%. In response to these values, we administered iron replacement therapy and transfusion of packed red cell at an outpatient clinic. After hospitalization, the hemoglobin was 13.2 g/dL, the hematocrit 38.6%, the white blood cell count was 7,700/mm3 and the platelet count was 322,000/mm3. The serum blood urea nitrogen was 8.9 mg/dL, the creatinine 0.57 mg/dL, AST 17 IU/L, ALT 14 IU/L, sodium 138 mEq/L, potassium 3.8 mEq/L and chloride 104 mEq/L. The serum iron was 7 ㎍/dL, the ferritin was 2.2 ㎍/dL and the TIBC was 379 ㎍/dL. A fecal occult blood test was positive. The chest X-ray and abdomen computed tomography were all negative for any abnormalities. In order to detect the cause of her iron deficiency anemia, we performed endoscopy, a small bowel series and colonoscopy. Endoscopy showed seven polyp-like mass lesions with abundant vasculature at the greater curvature of the body and fundus, the posterior wall of the gastro-esophageal junction and the anterior wall of the gastric angle (Figure 2). However, no active bleeding was observed. Hemangioma was diagnosed via a biopsy that was performed at this time (Figure 3). The small bowel series revealed several small intra-luminal nodular filling defects in the distal jejunal loops and ileum (Figure 4). In addition, eight multiple polypoid mass lesions with abundant vasculature were seen from the ascending colon to the rectum during colonscopy (Figure 5).

A tiny bluish subcutaneous nodule is seen on the toe of the left foot.

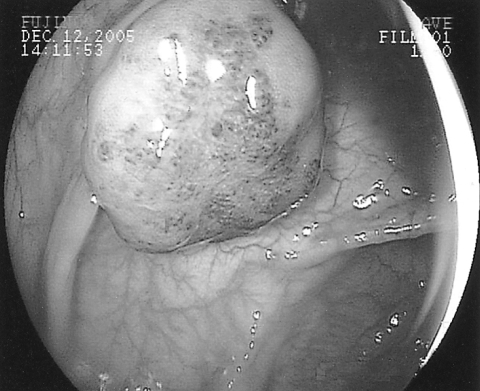
Endoscopy shows multiple polypoid mucosal nodules with abundant vasculature, and these nodules are centrally located at the greater curvature of the stomach's body and fundus, the posterior wall of the gastro-esophageal junction and the anterior wall of the gastric angle.
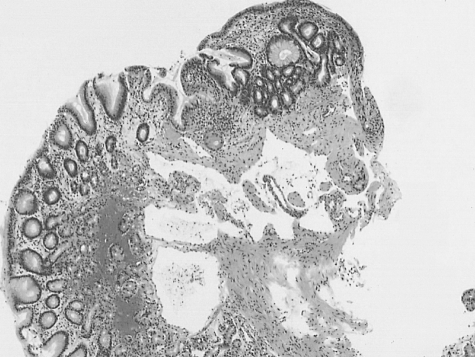
Endoscopic biopsy. It reveals several dilated, irregular endothelial cell that lined the cystic spaces; these cystic spaces contained scattered red blood cells within the mucosa. These findings are consistent with hemangioma.
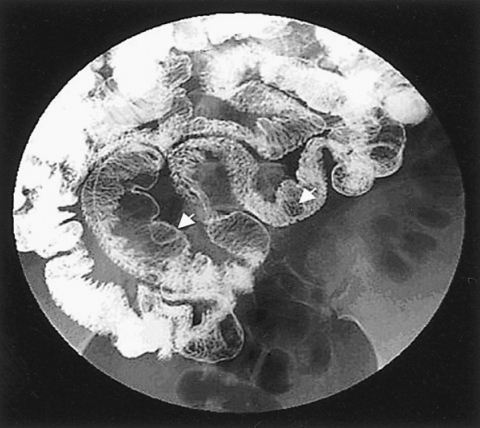
Small bowel series. It shows several small intra-luminal nodular filling defects (arrows) in the distal jejunal loops and the ileum.
Colonoscopy shows eight multiple polypoid mass lesions with abundant vasculature and these lesions are centrally located from the ascending colon to the rectum.
We were able to diagnose the patient with BRBNS due to the facts that the biopsies of both the recurrent nodules on the skin and the gastrointestinal mass lesions revealed hemangiomas, there were no recurrent episodes of epistaxis, no family history of any recurrent skin lesions or gastrointestinal bleeding, and her physical examination showed no skeletal deformity. On the 7th day after hospitalization, the patient's hemoglobin and hematocrit had decreased slightly to 12.1 mg/dL and 35.7%, respectively. However, melena or hematochezia was not noted. Methylprednisolone (2 mg/kg/day) was given orally starting at the 8th day of hospitalization, and there was no decrease in the hemoglobin and hematocrit values until the 17th day. On the other hand, a follow-up endoscopy performed on the 21st day showed no changes in size or number of the multiple polypoid mass lesions. The patient was able to maintain a hemoglobin level of 11.7 mg/dL and a hematocrit of 34.2% until the 22nd day, and it was then decided to discharge her with plans for her to undergo 4 months of methylprednisolone treatment (2 mg/kg/day for 1 month and 1 mg/kg/day for an additional 3 months). This was followed by a period of close observation at the outpatient clinic.
DISCUSSION
In this case, the patient had suffered from recurrent hemangiomas in the skin. In the process of evaluating the cause of the patient's iron deficiency anemia by performing endoscopy, a small bowel series and colonoscopy, multiple hemangiomas were found in the gastrointestinal tract.
Diseases that involve recurrent vascular malformation of the skin and gastrointestinal tract include BRBNS, Mafucci's syndrome, Rendu-Osler-Weber syndrome. However, the patients with Mafucci's syndrome also have dyschondria, and Rendu-Osler-Weber syndrome often involves recurrent episodes of epistaxis, the pathologic findings of telangiectasia and this disease is inherited in an autosomal dominant pattern. Therefore, we were able to diagnose our patient with BRBNS5, 6).
BRBNS (or Bean's syndrome) is a rare disorder that is characterized by multiple recurrent vascular malformations such as hemangiomas, and these primarily involve the skin and the gastrointestinal tract1). Gascoyen7) reported the disease's association with hemagniomas in the skin and gastrointestinal tract for the first time in 1860; Bean1) was the first to call it BRBNS in 1958. About 200 cases of BRBNS has been reported in the English literature, and with the exception of two Korean cases reported in the English literature, there have been no cases reported in the Korean literature3, 4).
The vascular malformations that appear in BRBNS include telangiectasia, capillary hemangioma, cavernous hemangioma, venous angioma and on rare occasion arteriovenous fistula8). They may involve the brain, liver, lung or muscle in addition to the skin and gastrointestinal tract1, 2). The most common clinical manifestation of BRBNS is iron deficiency anemia which is caused by bleeding of vascular malformations in the gastrointestinal tract. In most cases, the cause is occult bleeding, but there have been cases where the bleeding presented as melena or hematochezia. Intussusception, hemothorax, hemopericardium, pulmonary hypertension, dementia, paraparesis, ataxia, cortical blindness. Chronic consumption coagulopathy may also occur on ocassion8-13).
The skin lesions of BRBNS mainly appear in the trunk and upper extremities and these are characterized by their small size, bluish color, softness, absence of pain and bleeding, and the tendency to refill with blood after compression14, 15). The skin lesions in this case were also small, bluish, soft and compressible, and they occurred in the upper extremities; these are the typical features of BRBNS. The gastrointestinal lesions of BRBNS are usually distributed throughout the gastrointestinal tract and mostly in the small bowel and distal colon2, 16). Upon endoscopy, the mucosal nodules are either flat, polypoid or they have central bluish nipples. Also, some of these nodules showed evidence of recent or active bleeding. In our case, the gastrointestinal lesions were distributed from the stomach to the distal colon.
Although BRBNS develops sporadically in most cases, it is sometimes inherited in an autosomal dominant pattern and its association with chromosome 9p has already been established 17). In the light of the patient's lack of a family history of BRBNS, this case seems to have developed sporadically.
Several therapeutic modalities have been attempted to date for treating BRBNS. Medical treatment consists of iron supplementation for anemia2), steroids, interferon α-2a and octreotide to reduce the frequency and severity of bleeding episodes. However, in most cases, discontinuing administration of these medical treatments has led to recurrence of the disease18, 19). New therapeutic modalities for treating the gastrointestinal lesions have recently been attempted such as endoscopic laser photocoagulation, sclerosis, band ligation and polypectomy3, 20). In the event that any life-threatening hemorrhage occurs, either excision of the gastrointestinal lesions or segmental resection of the involved GI tract can be performed. Yet another lesion may subsequently appear that can result in rebleeding21). In a recent study performed by Fishman22) on ten patients with BRBNS, complete gastrointestinal endoscopy was conducted followed with removal of all the gastrointestinal lesions by means of wedge resection, endoscopic polypectomy, suture-ligation, segmental bowel resection and band ligation (surgical eradication), and the patients were followed up for five years on average. As a result, gastrointestinal bleeding recurred in only one patient who had received less extensive procedures. In our case, the patient's hemoglobin level has been constantly and appropriately maintained without any additional transfusions ever since the patient was started on methylprednisolone.
However, follow-up endoscopy performed on the 21st hospital day showed no interval changes in the size or number of the gastrointestinal lesions. Long term follow up is required in order to evaluate the effect of treatment with methylprednisolone on patients with BRBNS, and also to determine if surgical eradication may be needed.