The Pulmonary Embolism Severity Index in Predicting the Prognosis of Patients With Pulmonary Embolism
Article information
Abstract
Background/Aims
Many prognostic models have been developed to help physicians make medical decisions on treating patients with pulmonary embolism. Among these models, the Pulmonary Embolism Severity Index (PESI) has been shown to be a successful risk stratification tool for patients with acute pulmonary embolism. The PESI, however, had not been applied to patients with pulmonary embolism in Korea.
Methods
The patients included in this study were diagnosed by computed tomography at Inje University's Ilsan Paik Hospital between December 1999 and March 2007. Risk stratification for the patients was performed using the PESI. The mortality rate was calculated according to each PESI risk class.
Results
Of the 90 patients enrolled in this study, ten were assigned to PESI class I, 29 to PESI class II, 22 to PESI class III, eight to PESI class IV, and ten to PESI class V. The mortality rate after 30 days in each class was 0, 10.3, 9.1, 0, and 50% (p=0.0016), respectively, whereas the respective hospital mortality rate was 4.8, 13.8, 13.6, 12.5, and 50% (p=0.0065). The overall mortality was 9.5, 27.6, 31.8, 50.0, and 60%, respectively (p=0.0019). The mortality rate was significantly associated with the PESI class.
Conclusions
The PESI class was found to be significantly correlated with the 30-day mortality rate, hospital mortality, and overall mortality. Our data indicate that the PESI can be used to predict the prognosis of patients with pulmonary embolism and in making medical decisions regarding the treatment of patients with pulmonary embolism.
INTRODUCTION
Pulmonary embolisms occur relatively frequently, with 23 cases per 100,000 annually in the United States [1]. However, since its clinical features are nonspecific, a diagnosis of pulmonary embolism is not easy to make. Furthermore, without appropriate treatment, a pulmonary embolism can be fatal. Therefore, suspecting such a condition and evaluating it appropriately is important in making a prognosis. Once a prognosis has been made, the mortality rate can be lowered through proper treatment.
However, while significant effort has been made to clarify the risk factors and treatment of pulmonary embolism, relatively little data are available regarding a prognostic index. Nevertheless, since the development of the Geneva score [2] in 2000 and the Pulmonary Embolism Severity Index (PESI) [3] in 2005, two models have been introduced as prognostic-predictive indexes. Of these, the PESI has been shown to have higher predictive accuracy [4].
Ostensibly, Koreans may appear to have fewer risk factors for pulmonary embolism, such as obesity or deep vein thrombosis, compared to people in the West, and may thus be expected to suffer from pulmonary embolisms less often and have a better prognosis than Westerners. [5,6] However, at present few data exist to support this assertion or the utility of the PESI for Korean patients with pulmonary embolism. For this reason, we analyzed the usefulness of the PESI as presented by Aujesky et al [3] with regard to predicting the prognosis of Korean patients with pulmonary embolism.
METHODS
Patient Enrollwent
Between December 1999 and March 2007, we enrolled 195 hospitalized patients or outpatients at Inje University's Ilsan Paik Hospital diagnosed with acute pulmonary embolism according to the Korean Classification of Diseases (KCD). Of these patients, 84 with an inadequate diagnosis (i.e., pulmonary embolism was not confirmed by computed tomography (CT)) and 21 for whom survival or mortality could not be established through medical records or a phone call or whose preserved medical records were not sufficiently substantial to apply the PESI were excluded. Thus, 90 patients were evaluated in this study.
Study Design
In December 1999, we identified those patients for whom pulmonary embolism was confirmed by chest CT and analyzed their medical records. The age, sex, past medical history, combined disease, and clinical symptoms of the patients were considered in addition to the 11 indices included in the PESI [3].
According to the method suggested by Aujesky et al [3], points were given as follows: 1 for each year of age, 10 for male sex, 20 for a heart rate >110 beats/min, 30 for cancer, 10 for heart failure, 10 for chronic lung disease, 30 for a systolic pressure <100 mmHg, 20 for a respiratory rate >30 times/min, 20 for a body temperature <36℃, 60 for an altered mental state, and 20 for an arterial oxygen saturation value <90%. Based on the point distribution, a score below 65 was classified as PESI class 1, 66-85 as class II, 86-105 as class III, 106-125 as class IV, and over 126 as class V [3].
Among the items included in the PESI, arterial oxygen saturation was measured with an arterial blood gas analysis or a pulse oximeter. For those cases in which no actual measurement was made, a case of respiratory distress requiring oxygenation was recorded.
The subjects were reviewed on the basis of their past history and combined disease, such as diabetes, hypertension, or cerebral hemorrhage, as well as a history of surgery requiring general anesthesia. For the clinical symptoms, we examined four vital signs to assess whether the patient had respiratory distress altering his/her consciousness and required oxygenation.
Survival was confirmed through the use of medical records or a phone call. Patients with unknown survival were excluded from the subject group.
Data analysis and statistics
The data were analyzed using basic technological statistics. Our results indicated that the higher the class, the higher the mortality rate. This tendency was measured using the chi-square test for trends, and a significance level of 0.01 was applied. For the statistical management of the data, we used SPSS for Windows (version 11.0) and MedCalc (version 9.5.1).
RESULTS
Basal Characteristics
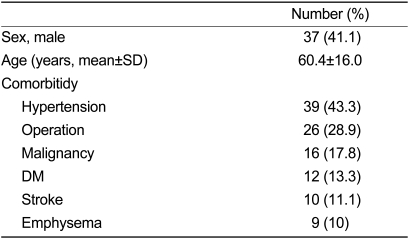
Of the 90 patients included in this study, 37 (41.1%) were men and 53 (58.9%) were women, resulting in a male-to-female ratio of 1:1.4. The average age of the patient group (±standard deviation) was 60.4 (±16.0) years of age (Table 1). None of the patients was between the ages of ten and 20, whereas five were in their 20s (5.6%), ten were in their 30s (11.1%), 11 were in their 40s (12.2%), ten were in their 50s (11.1%), 22 were in their 60s (24.4%), 29 were in their 70s (32.2%), and three were in their 80s (3.3%).
Baseline characteristics
Comorbidities of the Subjects
Thirty-nine patients (43.3%) had hypertension, 12 (13.3%) had diabetes, and 16 (17.8%) had either been diagnosed with cancer or were being treated for cancer. Nine patients (10%) were confirmed as having emphysema through chest CT, while ten patients (11.1%) had a cerebral hemorrhage and cerebral infarction, and 26 (28.9%) had a surgical history (Table 1).
PESI Classificatich
With regard to the distribution of the patients according to their PESI risk class, 21 (23%, 34-65 points, average: 49.9 points) patients were in class I (<65 PESI points), 29 (32%, 67-85 points, average: 77.6 points) were in class II (66-85 PESI points), 22 (25%, 88-105 points, average: 77.6 points) were in class III (86-105 PESI points), eight (9%, 106-121 points, average: 71.1 points) were in class IV (106-125 PESI points), and ten (11%, 145-245 points, average: 187 points) were in class V (>126 PESI points); thus, most of the patients were in class II while the smallest number were in class IV (Fig. 1).

Patients distribution according to PESI risk class.
Mortality rate base on the PESI
The mortality rate after 30 days, mortality rate during hospitalization, and total mortality rate were compared according to the PESI risk classes of the patients. At 30 days, the mortality rate was 11.1%. When this result was analyzed according to PESI class, a significant trend toward increased mortality with a higher class was detected (p=0.0016), with 0% in class I, 10.3% in class II, 9.1% in class III, 0% in class IV, and 50% in class V. In considering the 0% mortality rate detected for class IV, note that the average hospital stay for this group was 10 days shorter than that for the other groups; thus, the possibility of underestimation exists. In comparison, the hospital mortality rate was 15.6%; when it was analyzed according to PESI class, a significant trend (p=0.0065) was observed, with 4.8% in class I, 13.8% in class II, 13.6% in class III, 12.5% in class IV, and 50% in class V (Fig. 2). The total mortality rate was 30%; when it was analyzed according to PESI class, an increasing tendency toward the higher class was observed, with 9.5% in class I, 27.6% in class II, 31.8% in class III, 50% in class IV, and 60% in class V (p=0.0019) (Fig. 3).
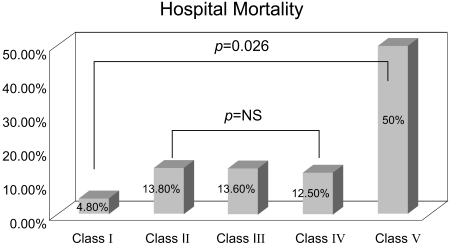
Hospital mortality according to PESI risk classification.
PESI, pulmonary embolism severity index; NS, not significant.
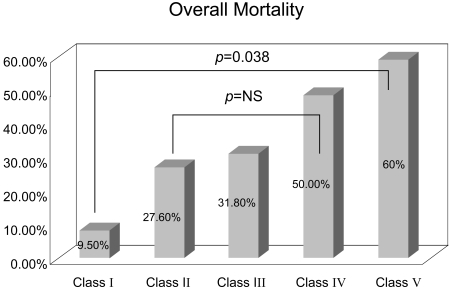
Overall mortality according to PESI risk classification.
PESI, pulmonary embolism severity index; NS, not significant.
Mortality rate of the redistri-buted PESI
Grouping of the PESI classes into low- (class I), intermediate- (classes II-IV), and high-risk (class V) groups produced a 30-day mortality rate of 0, 8.2, and 50%, respectively. Compared to the results before the redistribution, the tendency was quite clear (p=0.0016→0.0003). The mortality rate during hospitalization was 4.8, 13.1, and 50% for the low-, intermediate-, and high-risk groups, respectively, and the tendency was much clearer (p=0.0065→0.0038), as was the 30-day mortality rate. The total mortality rate was 9.5, 31.1, and 60% for the low-, intermediate-, and high-risk groups, respectively, with a weakened tendency (p=0.0019→0.0034) (Table 2).

Hospital mortality and overall mortality according to redistributed PESI risk class
DISCUSSION
Various mortality rates have been reported for patients with pulmonary embolism (from 2 to 95%) [7-9]. Based on our data, the 30-day mortality rate was 11.1%, whereas the mortality rate during hospitalization was 15.6% and the total mortality rate was 30.0%. We suspect that the reported mortality rates were inconsistent because each patient had several confounding factors that may have affected his/her prognosis, such as different combined diseases and different degrees of pulmonary embolism. However, few reports have addressed the factors that can affect a prognosis or the predictive factors of pulmonary embolism.
To create a prognostic-predictive system for patients with pulmonary embolism, the Geneva score [2] was developed in 2000, whereas the PESI [3] was first presented in 2005. Since that time, the PESI has been shown to be a slightly better system for making prognoses [4].
Aujesky et al. [3] reported that the 30-day mortality rate was 0.8-27.1% for PESI classes I-V, claiming that patients in a higher PESI class had a tendency toward an increased mortality rate. Thereafter, when the PESI was applied to Koreans, the 30-day mortality rate, mortality rate during hospitalization, and total mortality rate were 0-60%. Since all of the results were significant, the PESI may be useful in predicting the prognosis of Korean patients with pulmonary embolism (30-day mortality: p=0.0016, hospital mortality: p=0.0065, and overall mortality: p=0.0019).
Aujesky et al [3] asserted that the PESI could be used to identify low-risk groups and to develop a treatment plan. They reported that the 30-day mortality rate for patients in PESI classes I and II was below 1.6 and 3.5%, respectively. The risk of hemorrhage and the frequency of a recurrence of pulmonary embolism during treatment were shown to be lower. They also claimed that in class I and II patients, low-molecular-weight heparin could be used safely, even in outpatients, and that these patients were in fact a low-risk group [10]. However, when the 30-day mortality rate was examined according to PESI class in Korean patients, the value for the class I patients was 0%, while that for the class II patients was 10.3%, reflecting a significant difference between these groups. Therefore, as was determined by Aujesky et al. [3], the patients in PESI class II were difficult to treat through ambulatory care. The mortality rate during hospitalization (class I: 4.8%, class II: 13.8%) (p=0.029) and the total mortality rate (class I: 9.5%, class II: 27.6%) (p=0.115) were not statistically meaningful, but a difference was seen between the two groups. This should be considered because the number of subjects in PESI class I was 21 while the number in PESI class II was 29. Thus, regarding both PESI classes I and II as low-risk groups for outpatient treatment could be dangerous.
The patients in PESI classes II-IV, however. showed a similar 30-day mortality rate, mortality rate during hospitalization, and total mortality rate. In classes II-IV, the higher classes did not have a tendency toward an increased mortality rate (p=0.424, 0.995, and 0.281, respectively), and when PESI classes II-IV were redistributed as an intermediate-risk group, the higher classes had a clear tendency toward an increased mortality rate (30-day mortality: p=0.0016→0.0003, hospital mortality: p=0.0065→0.0038, and overall mortality: p=0.0019→0.0034).
Therefore, if the PESI classes were redistributed as low- (class I), intermediate- (class II-IV), and high-risk (class V) groups, the convenience, feasibility, and accuracy of the prognostic-predictive index would be improved. When mortality rates were compared among the groups, the 30-day mortality rate in the low-, intermediate-, and high-risk groups was 0, 8.2, and 50%, respectively, while the mortality rate during hospitalization was 4.8, 13.1, and 50%, respectively. In comparison, the total mortality rate was 9.5, 31.1, and 60%, respectively (Table 2).
To determine an appropriate treatment plan for pulmonary embolism, the most important considerations are the patient's hemodynamic stability and echocardiographic findings. In this study, right ventricular dyskinesia was observed in three of 75 patients who had taken an echocardiogram; notably, one of these patients was in PESI class III and the other two were in PESI class IV, indicating that all instances occurred in the relatively higher PESI classes. This suggests that the PESI score can be used to determine a treatment plan for those patients in high-risk groups as well as for patients in low-risk groups.
This study has the intrinsic restrictions of any retrospective study, including inconsistencies in patient selection and the treatment plan. It was also based on a relatively small number of patients (n=90) for whom the causes of death were not classified. However, to improve the accuracy of our results, only those cases in which pulmonary embolism was confirmed through chest CT were included. In addition, the use of phone calls enabled us to conduct a relatively long-term follow-up to confirm the 30-day mortality rate, as well as the mortality rate during hospitalization and the total mortality rate. This study indicates that the PESI is a helpful predictor, not just of the 30-day mortality rate but also of the mortality rate during hospitalization and the total mortality rate.
Risk group classification using the PESI can predict not only the 30-day mortality rate but also the mortality rate during hospitalization and the total mortality rate, indicating that it is a relatively accurate prognostic-predictive index. Our work suggests that the use of comparative data incorporating hemodynamic stability and echocardiographic findings in conjunction with a prospective approach can be used to develop a standard treatment plan index for pulmonary embolism.