Reversible dilated cardiomyopathy caused by idiopathic hypoparathyroidism
Article information
Abstract
Dilated cardiomyopathy (DCM) is usually an idiopathic disease with a poor prognosis. Hypocalcemia is a rare and reversible cause of DCM. Here, we report a 50-year-old female with DCM, induced by idiopathic hypoparathyroidism, that improved after treatment with calcium.
INTRODUCTION
Dilated cardiomyopathy (DCM) is a heart muscle disorder often associated with enlargement of one or both ventricles and systolic dysfunction [1]. There is no identifiable cause in the majority of patients with DCM, leading to a diagnosis of idiopathic DCM. However, DCM may be associated with a variety of pathologies [2].
Hypocalcemia is a rare and reversible cause of DCM [3]. Here, we report a patient with severe left ventricular systolic dysfunction that was induced by idiopathic hypoparathyroidism and improved after treatment with calcium.
CASE REPORT
A 50-year-old female suffering from dyspnea (New York Heart Association class IV) and orthopnea was admitted to our cardiology clinic at Hallym University Kangdong Sacred Heart Hospital, Seoul, Korea. She had been treated with neurotonics due to dizziness for 2 months, and dyspnea had developed 5 days before admission.
On admission, the patient's blood pressure was 100/60 mmHg, and her pulse rate was 82 beats per minute. No heart murmur was detected, but rales were heard on both sides of the lung field. Physical examination did not reveal neurological dysfunction with regard to muscle tone and sensitivity. Neither pitting edema nor neck vein distension was observed. Electrocardiography showed a prolonged QT interval (432 ms) with nonspecific ST-T changes. Chest X-ray revealed prominent cardiomegaly with pulmonary congestion (Fig. 1). Echocardiography indicated decreased left ventricular function.

Chest radiography (A) on admission and (B) after 4 months of treatment. Cardiomegaly and pulmonary congestion were improved after correction of hypocalcemia.
The ejection fraction of the left ventricle (LV) was 36.5%, and the diastolic and systolic dimensions of the LV were 59 and 47 mm, respectively. Moderate mitral and tricuspid valvular regurgitations were identified with global hypokinesia. Serum levels of creatine kinase-MB and troponin-I were within the respective normal ranges, whereas the brain natriuretic peptide level was 1,855.1 pg/mL (reference range, 0 to 100).
Based on her symptoms and the results of several previous studies, we made a diagnosis of congestive heart failure and began initial treatment with furosemide injection. The patient had no history of hypertension, diabetes mellitus, or smoking. In addition, we could not find any influence of neurotonics taken before admission on the patient's heart.
Additional studies were performed to determine the etiology of congestive heart failure. Laboratory studies revealed reduced total serum calcium of 3.7 mg/dL (reference range, 8.4 to 10.2), magnesium of 1.7 mg/dL (reference range, 1.9 to 2.5), and ionized calcium of 0.6 mmol/L (reference range, 1.12 to 1.3). The phosphorus and creatinine levels were 8.5 mg/dL (reference range, 2.5 to 4.6) and 1.5 mg/dL (reference range, 0.6 to 1.2), respectively. Hormone analysis was performed and showed free T4 and thyroid stimulating hormone to be within the respective normal ranges, while intact parathyroid hormone (PTH-intact, terminal) level was 8.17 pg/mL (reference range, 15 to 68). The vitamin D level was 10.1 ng/mL (reference range, 11 to 70). Coronary angiography did not detect significant stenotic lesions on the coronary arteries.
We made a diagnosis of DCM caused by severe hypocalcemia, and treatment was started with intravenous calcium and oral vitamin D3 and calcitriol. Concurrently, we sought to determine the cause of severe hypocalcemia, and a neck sonogram was ordered to rule out parathyroid infiltrating disease. However, no abnormalities were observed. Rheumatoid factor and fluorescent antinuclear antibody test were also assessed to rule out autoimmune disease; their serum levels were within the respective normal ranges (Table 1).
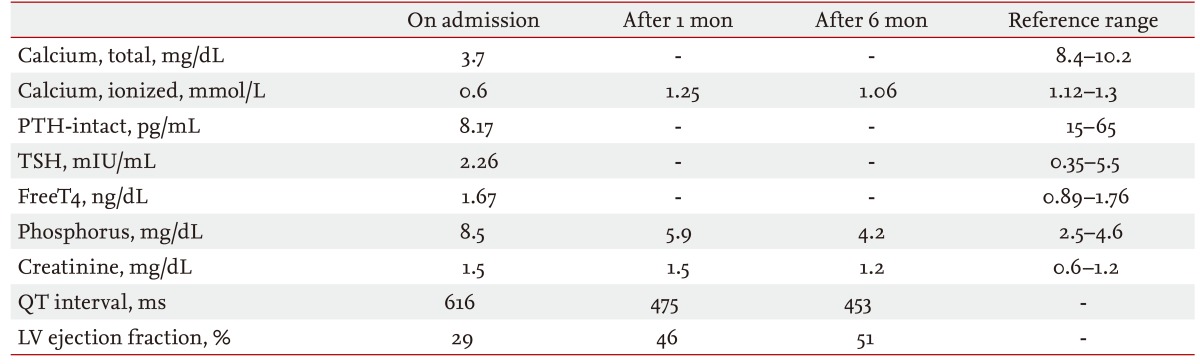
Laboratory findings of the patient
The patient was finally diagnosed with idiopathic hypoparathyroidism-induced DCM, and the treatment described above was continued in addition to conventional heart failure management. The patient responded to this regimen with remarkable improvement of dyspnea, and chest X-ray showed a reduction of cardiomegaly with clearance of pulmonary edema (Fig. 1). Calcium levels reached the normal range; the initial ionized calcium level was 0.6 mmol/L, and increased to 0.89 mmol/L after 5 days of calcium supplementation. The prolonged QT interval was also reduced (Fig. 2). Discharge treatment included oral calcium, vitamin D3, and congestive heart failure medications.

Electrocardiograms recorded (A) on admission and (B) after 3 months of treatment. The original prolonged QT interval improved to within the normal range after correction of hypocalcemia; the initial QT interval was 522 ms and it reached 348 ms after 3 months.
Follow-up visits revealed progressive improvement of myocardial function; the LV ejection fraction was 46% by the first month and 51% by the third month. In addition, the LV diastolic and systolic dimensions were decreased to 53 and 37 mm, respectively (Fig. 3). Calcium and vitamin treatments were maintained, and aspirin, an angiotensin receptor blocker and statin medications were added. The patient is currently well on this therapy.
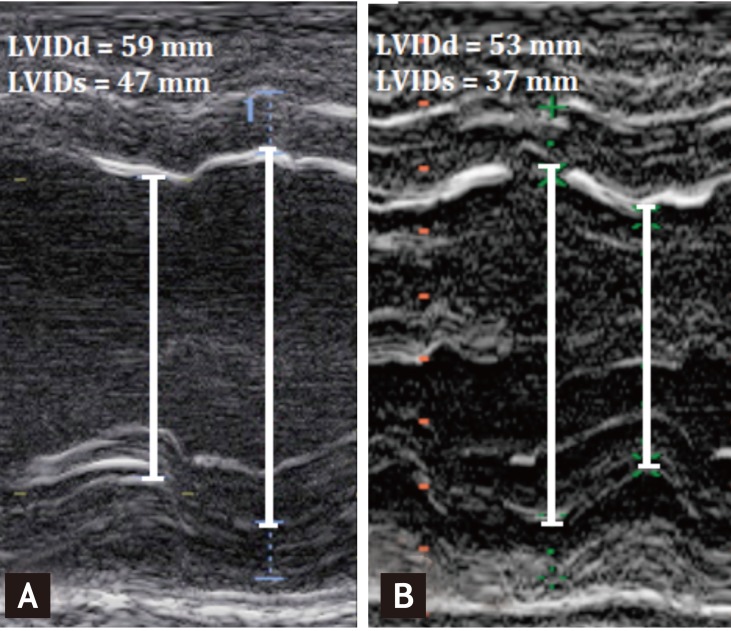
Transthoracic echocardiography, M mode (A) on admission and (B) after 3 months of treatment. Before treatment, the left ventricular diastolic internal dimension (LVIDd) was 59 mm and the left ventricular systolic internal dimension (LVIDs) was 47 mm. After 3 months of treatment, the LVIDd was 53 mm and the LVIDs was 37 mm.
DISCUSSION
We presented a case of hypocalcemia-induced cardiomyopathy that was improved by calcium and vitamin D replacement. Although reversible congestive heart failure caused by hypocalcemia has been described in previous case reports, idiopathic hypoparathyroidism-induced hypocalcemic cardiomyopathy is very rare. Idiopathic hypoparathyroidism is a relatively rare disease characterized by hypocalcemia and hyperphosphatemia due to PTH deficiency of unknown cause [4]. In our case, the patient had no history of thyroid surgery, chronic renal failure or other various factors that might lead to hypocalcemia.
Hypocalcemia as a cause of cardiac dysfunction can easily be overlooked because the clinical symptoms of hypocalcemia, such as fatigue and muscle weakness, are often regarded as subjective and ambiguous in the absence of tetany. In our patient, severe cardiac depression was present, but no signs of weakness or abnormal muscle tone were observed in the skeletal musculature. This can be explained by differences between cardiac and skeletal muscle with regard to calcium cycling during contraction and relaxation.
Cardiomyocytes exchange a larger portion of calcium with the extracellular space than skeletal myocytes. This difference is due mainly to functional differences in L-type calcium channels in skeletal muscle compared to those in the heart [5-7]. In cardiac muscle, the L-type calcium channel is a calcium-conducting ion channel that transports a small amount of extracellular calcium to the cytosol following activation by membrane depolarization. In contrast, the L-type calcium channel in skeletal muscle functions as a voltage sensor to induce calcium release from the sarcoplasmic reticulum [8,9]. Therefore, cardiac depression may be specifically induced by profound and prolonged hypocalcemia without affecting skeletal muscle function. When treating severe heart failure in patients with hypocalcemia, we should consider that furosemide may induce further hypocalcemia. Patients with heart failure caused by hypocalcemia are usually asymptomatic, and physicians initially treat them with diuretics without knowing their serum calcium levels. As clinical signs and hemodynamics may worsen rather than improve, serum calcium levels should be closely monitored in patients on furosemide.
We speculate that hypocalcemia-induced heart failure occurs more frequently than reported because of asymptomatic hypocalcemia. In our case, LV systolic function and additional symptoms were improved after calcium treatment. In conclusion, hypocalcemia should be included in the differential diagnosis of all patients with congestive heart failure as a possible cause of reversible congestive heart failure.
Notes
No potential conflict of interest relevant to this article is reported.