A combination of early warning score and lactate to predict intensive care unit transfer of inpatients with severe sepsis/septic shock
Article information
Abstract
Background/Aims
The modified early warning score (MEWS) is used to predict patient intensive care unit (ICU) admission and mortality. Lactate (LA) in the blood lactate (BLA) is measured to evaluate disease severity and treatment efficacy in patients with severe sepsis/septic shock. The usefulness of a combination of MEWS and BLA to predict ICU transfer in severe sepsis/septic shock patients is unclear. We evaluated whether use of a combination of MEWS and BLA enhances prediction of ICU transfer and mortality in hospitalized patients with severe sepsis/septic shock.
Methods
Patients with severe sepsis/septic shock who were screened or contacted by a medical emergency team between January 2012 and August 2012 were enrolled at a university-affiliated hospital with ~2,700 beds, including 28 medical ICU beds.
Results
One hundred patients were enrolled and the rate of ICU admittance was 38%. MEWS (7.37 vs. 4.85) and BLA concentration (5 mmol/L vs. 2.19 mmol/L) were significantly higher in patients transferred to ICU than those in patients treated in general wards. The combination of MEWS and BLA was more accurate than MEWS alone in terms of ICU transfer (C-statistics: 0.898 vs. 0.816, p = 0.019). The 28-day mortality rate was 19%. MEWS was the only factor significantly associated with 28-day mortality rate (odds ratio, 1.462; 95% confidence interval, 1.122 to 1.905; p = 0.005).
Conclusions
The combination of MEWS and BLA may enhance prediction of ICU transfer in patients with severe sepsis/septic shock.
INTRODUCTION
The modified early warning score (MEWS) is calculated based on physiologic variables and facilitates early identification of hospitalized patients at high risk of clinical deterioration. Two studies have reported that MEWS can predict intensive care unit (ICU) admission and in-hospital mortality [12]. Severe sepsis/septic shock is a life-threatening condition that, in 1995, accounted for the hospitalization of at least 750,000 people in the United States [3], and rates of hospitalization and mortality due to severe sepsis continue to increase rapidly [4]. In South Korea, the prevalence of severe sepsis in patients admitted to the ICU is ~7.3% and the mortality rate of these patients is 64.6%. Admittance to the ICU from a general ward is a prognostic factor for patients with severe sepsis [5]. Because ICU facilities are limited, patients with severe sepsis/septic shock are sometimes treated in general wards. Whether a patient with severe sepsis/septic shock should be moved to ICU or should remain in the general ward is difficult to judge, and is generally decided by the treating physician.
The medical emergency team (MET), including physicians and nurses, screens and detects clinically deteriorated hospitalized patients at early stages and manages patients who require acute care in general wards [6]. Several studies have reported that METs reduce the rate of ICU admission, the number of patients who suffer a cardiac arrest, and mortality rate [78]. Severe sepsis/septic shock in patients in general wards is the most common reason for transfer by METs of hospitalized patients in general wards to the ICU [9]. In the Surviving Sepsis Campaign guidelines, the MEWS is recommended as a screening tool to identify and manage sepsis [10]. However, strong evidence of the value of MEWS for determining which severe sepsis/septic shock patients in general wards should be transferred to the ICU is lacking. Lactate (LA) in the blood lactate (BLA) is measured to guide the evaluation and management of patients with sepsis and is associated with clinical outcomes [11]. Although a few reports have showed that the combination of early warning score (EWS) and BLA predict mortality better than EWS alone in critically ill patients admitted to the ICU [12], whether measuring BLA improves the ability of MEWS to predict ICU transfer remains unknown. Therefore, in this study, we evaluated whether there was a significant difference in MEWS between hospitalized patients with severe sepsis/septic shock who were transferred to the ICU and those treated in general wards, and whether the combination of MEWS and BLA improves the ability of MEWS to identify sepsis/septic shock patients who should be transferred to the ICU. We also assessed the ability of the MEWS and BLA to predict the 28-day mortality rate of sepsis/septic shock patients.
METHODS
Study design and subjects
Patients with severe sepsis/septic shock who were screened or contacted by medical alert team (MAT) between January 2012 and August 2012 were enrolled. This study was conducted in Asan Medical Center, a university-affiliated, urban, tertiary-care hospital in South Korea with ~2,700 beds, including 28 medical ICU beds. The medical records of the enrolled patients were reviewed retrospectively, and demographic, clinical, and laboratory data were collected.
Severe sepsis/septic shock developing during hospitalization was screened or identified by automatic activation of an MET in our center by electronic medical record-based monitoring as reaching a threshold for a relevant vital sign or laboratory measurement (based on the medical emergency system criteria used in Asan Medical Center) [13] or by calling by nurses or physicians.
MEWS was calculated at the time at which the MET was contacted. The MEWS consists of blood pressure, pulse rate, respiratory rate, body temperature, and mental status [1].
Patients with severe sepsis/septic shock were eligible if they were aged ≥ 18 years, had been in the general ward for more than 24 hours, and their systolic blood pressure was less than 90 mmHg at the time at which the MAT was contacted, in accordance with the diagnostic criteria defined by the American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Committee [14].
Patients were excluded if they did not fulfill all of the inclusion criteria or if they fulfilled one or more of the following exclusion criteria: (1) MEWS could not be calculated due to omission of a measurement; (2) patients with a 'do-not-resuscitate' status; and (3) a MAT was contacted to perform cardiopulmonary resuscitation because the patient had suffered a cardiac arrest caused by septic shock.
BLA concentrations were measured at the time at which the MET was contacted. LA concentration in arterial blood was measured routinely if sepsis was suspected. After assessing all clinical, physiological, and laboratory findings, the decision regarding ICU transfer of inpatients with severe sepsis/septic shock was made by the attending physician or a member of the ICU staff.
The criteria for ICU transfer in patients with severe sepsis/septic shock were as follows: (1) sustained shock requiring norepinephrine ≥ 0.1 µg/kg/min despite adequate fluid resuscitation; (2) acute respiratory failure (respiratory rate > 30/min, PaO2 < 60 mmHg in room air or PaCO2 > 50 mmHg); (3) acute heart failure or pulmonary edema; (4) acute renal failure requiring hemodialysis; and (5) drowsy mentality. ICU transfer was indicated when at least one of the above mentioned developed in hospitalized patients with severe sepsis/septic shock.
The enrolled patients were divided into two groups: one treated in general wards and the other transferred to the ICU. Variables such as MEWS and BLA were compared between these groups. In addition, the 28-day mortality rate was evaluated. Models for prediction of ICU transfer and 28-day mortality rate were assessed.
This study protocol was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB No. 2013-0776). The requirement for informed consent was waived by the IRB due to minimal harm and general impracticability. The study was conducted in accordance with the established ethical standards of the medical center and with the principles of the Declaration of Helsinki.
Statistical analysis
Categorical data are expressed as numbers (percentages) and continuous data as means ± standard deviations. Comparisons were performed using the chi-square test for categorical variables and the Mann-Whitney U test for continuous variables. Univariate and multivariate logistic analyses were performed to evaluate factors associated with ICU admission and 28-day mortality rate of patients with severe sepsis/septic shock. Two logistic regression models were compared: the EWS model and the combination of the EWS model and BLA level. The predictive accuracy of the models was quantified by calculating the C-statistics. A p value < 0.05 was considered to indicate significance. All analyses were performed using SPSS version 18 (SPSS Inc., Chicago, IL, USA) and R 2.12.5 (R Development Core Team, GNU General Public License, www.r-project.org).
RESULTS
Patient characteristics
During the study period, 186 patients were referred to the MET because they developed septic conditions, and 100 of these patients were enrolled in the study (Fig. 1). Of these enrolled patients, 62 (62%) were managed in general wards and 38 (38%) were transferred to the ICU. The baseline characteristics of these patients are described in Table 1. The mean patient age was 57.3 ± 15.9 years and more than half of the patients were male. Neoplasm was the most common comorbidity. Intra-abdominal infection was the most common source of severe sepsis/septic shock, followed by pneumonia. There were more patients with septic shock in the ICU transfer group than the general ward-managed group. There were no significant differences in mean age, gender, comorbidities, or source of infection between the general ward group and the ICU group.
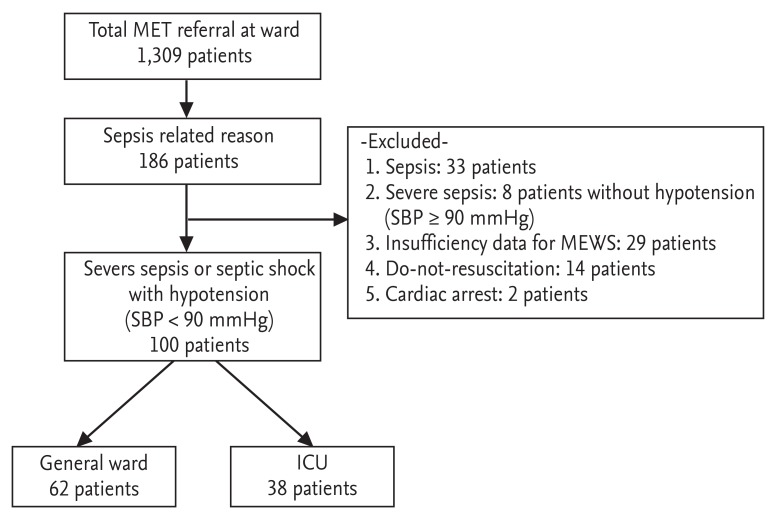
Diagram of patient enrollment in the study. MET, medical emergency team; MEWS, modified early warning score; SBP, systolic blood pressure; ICU, intensive care unit.
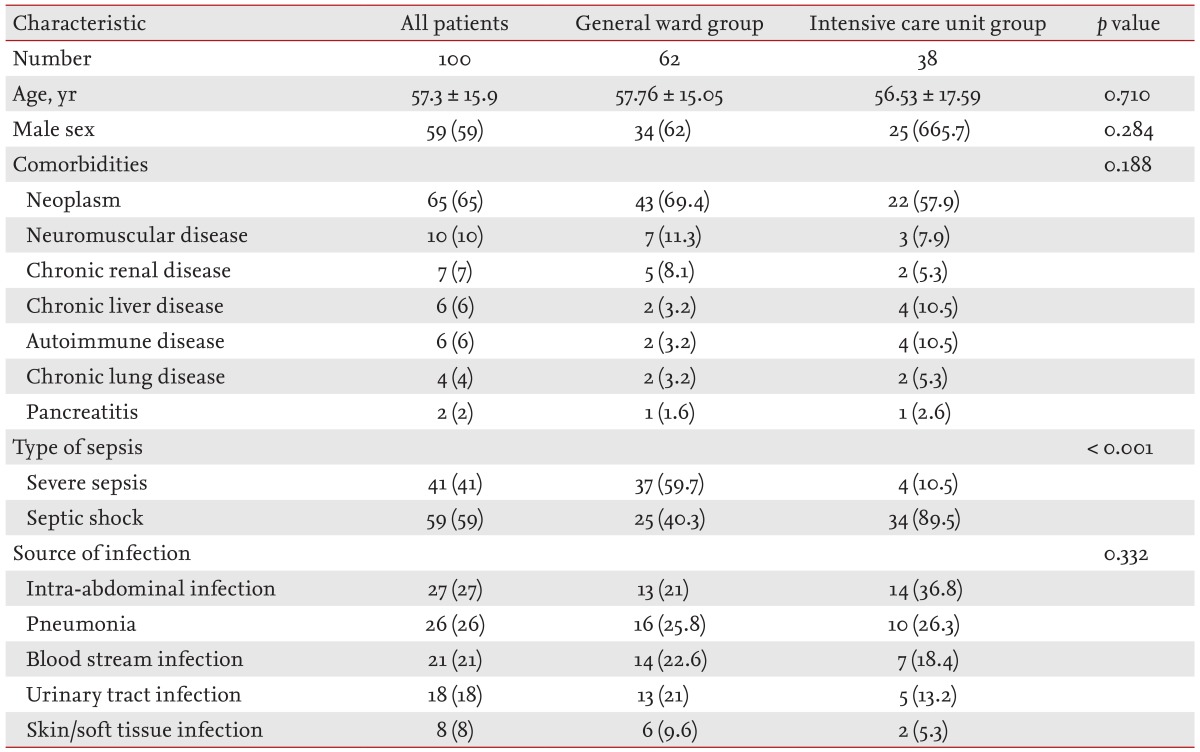
Baseline characteristics of the enrolled patients
Physiologic parameters, laboratory data, and warning scores of patients
Table 2 shows the physiologic parameters, laboratory data, and warning scores of the patients at the time of MET activation. Compared to the general ward group, the ICU group had lower systolic pressures, and higher heart and respiratory rates. BLA and procalcitonin concentrations were significantly higher in the ICU-transferred group than in the general ward-managed group. MEWS was significantly higher in the ICU-transferred group than in the general ward-managed group. MEWS-LA was significantly higher in the ICU transferred group than in the general ward-managed group.
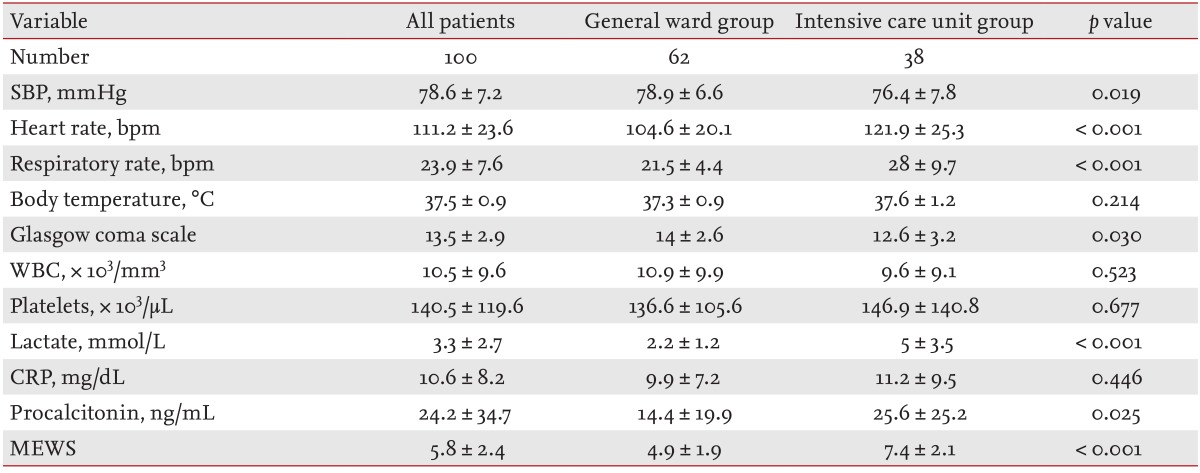
Physiologic parameters, laboratory data, and warning scores of patients at the time of activation of the medical alert team
Comparison of MEWS alone and the combination of MEWS and BLA for predicting ICU transfer
Table 3 shows two models for the prediction of ICU transfer of inpatients with severe sepsis/septic shock. To compare the accuracy of the two models, multivariate logistic regression models were used and C-statistics of each group were compared.

Comparison of models for predicting intensive care unit transfer of inpatients with severe sepsis/septic shock
C-statistic for MEWS alone and the combination of MEWS and BLA were 0.816 and 0.898, respectively; this difference was significant. The cut-off values for prediction of ICU transfer of MEWS and BLA concentration were 5.5 (81.6% sensitivity and 66.1% specificity) and 3.05 (73.7% sensitivity and 87% specificity), respectively.
Factors associated with 28-day mortality rate
The 28-day mortality rate was 19%. Only MEWS was positively associated with 28-day mortality of inpatients with severe sepsis/septic shock in univariate and multivariate analyses (Table 4).

Univariate and multivariate analyses of factors associated with 28-day mortality rate
DISCUSSION
MEWS and BLA concentration were significantly higher in inpatients with severe sepsis/septic shock who were transferred to the ICU than in those who were managed in general wards. Furthermore, MEWS alone could predict patient transfer to the ICU; the predictive power was improved when MEWS was combined with BLA concentration. The 28-day mortality rate was associated with the MEWS.
MEWS was developed using only physiologic parameters, is associated with an increased risk of death and ICU transfer [1], and has been used to recognize and respond early to deterioration of patients. Moon et al. [2] reported that the introduction of MEWS charts significantly reduced the number of cardiac arrest calls and in-hospital mortality rates. In a recent study of MET in our center, MEWS was associated with the 28-day mortality rate (odds ratio, 1.15; 95% confidence interval, 1.05 to 1.25) [13]. An elevated BLA concentration is associated with poor outcomes in patients with infection [11]. Clearance of BLA by 10% early during resuscitation is associated with improved survival in patients with sepsis [1516]. Measurement of BLA level is considered essential for predicting the prognosis of patients with sepsis.
Whether the combination of the MEWS and BLA level is a better predictor of ICU transfer has not been extensively investigated. In two recent retrospective studies, Jo et al. [1217] combined BLA concentration with the VitalPAC EWS to calculate the ViEWS-L score. The ViEWS-L score was compared to preexisting scoring systems in critically ill medical patients and blunt trauma patients. They concluded that the ability of ViEWS-L to predict the mortality of critically ill or blunt trauma patients admitted to the ICU via emergency departments is identical or superior to that of the existing scoring systems. About two thirds of these critically ill patients were diagnosed with sepsis; however, there is insufficient evidence to extrapolate these findings to all patients with sepsis, especially those with severe sepsis or septic shock. Indeed, only patients admitted to the ICU via emergency departments were included; those admitted to the ICU via other routes were not considered. Therefore, the ability of MEWS together with BLA concentration to predict ICU admission and in-hospital mortality rate of patients with sepsis requires further investigation. The MET monitors hospitalized patients at our center, and early goal-directed therapy was introduced to treat patients with severe sepsis/septic shock in general wards. The decision regarding whether a patient with sepsis should be transferred to the ICU or kept in the general ward is always difficult, and an improved scoring system is required to guide such decisions. We investigated whether addition of BLA concentration improved the ability of MEWS to predict the ICU transfer of hospitalized patients with severe sepsis/septic shock. In terms of ICU transfer, the combination of MEWS and BLA was a superior predictor than MEWS alone. Our data suggest that MEWS-LA is a candidate scoring system for the identification of severe sepsis/septic shock patients in general wards who should be transferred to the ICU.
This study had several limitations. First, because it was performed at a single center and patients were analyzed retrospectively, it is difficult to extrapolate the findings to other hospitals. Second, the sample size was relatively small; therefore, prospective randomized trials are required to validate the usefulness of MEWS-LA. Third, only patients with severe sepsis/septic shock and a systolic blood pressure less than 90 mmHg were enrolled, and it is unknown whether a combination model of MEWS and BLA is similarly useful in patients with sepsis or normotensive severe sepsis.
In conclusion, compared to MEWS alone, the combination of MEWS and BLA concentration was a predictor of which severe sepsis/septic shock patients in general wards should be transferred to the ICU.
KEY MESSAGE
1. Modified early warning score-lactate can facilitate the determination of patients who develop severe sepsis/septic shock in general wards who should be transferred to the intensive care unit.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.