Can proton pump inhibitors reduce rebleeding following Histoacryl sclerotherapy for gastric variceal hemorrhage?
Article information
Abstract
Background/Aims:
To evaluate the efficacy of proton pump inhibitors (PPIs) in reducing rebleeding and bleeding-related death rates after endoscopic gastric variceal obliteration (GVO) using N-butyl-2-cyanoacrylate (NBC).
Methods:
This study enrolled 341 patients who were consecutively diagnosed with and treated for bleeding gastric varices. The patients were divided into PPI and non-PPI groups, and their endoscopic findings, initial hemostasis outcomes, rebleeding and bleeding-related death rates, and treatment-related complications were analyzed.
Results:
The rate of initial hemostasis was 97.1%. rebleeding occurred in 2.2% of patients within 2 weeks, 3.9% of patients within 4 weeks, 18.9% of patients within 6 months, and 27.6% of patients within 12 months of the GVO procedure. A previous history of variceal bleeding (relative risk [RR], 1.955; 95% confidence interval [CI], 1.263 to 3.028; p = 0.003) and use of PPIs (RR, 0.554; 95% CI, 0.352 to 0.873; p = 0.011) were associated with rebleeding. Child-Pugh class C (RR, 10.914; 95% CI, 4.032 to 29.541; p < 0.001), failure of initial hemostasis (RR, 13.329; 95% CI, 2.795 to 63.556; p = 0.001), and the presence of red-colored concomitant esophageal varices (RR, 4.096; 95% CI, 1.320 to 12.713; p = 0.015) were associated with bleeding-related death.
Conclusions:
The prophylactic use of PPIs reduces rebleeding after GVO using NBC in patients with gastric variceal hemorrhage. However, prophylactic use of PPIs does not reduce bleeding-related death.
INTRODUCTION
The prevalence of gastric varices (GVs) in patients with portal hypertension varies from 18% to 70% [1,2]. Although gastric variceal hemorrhages (GVHs) are less common than esophageal variceal hemorrhages (EVHs), they tend to be more severe and associated with higher rates of mortality and rebleeding compared with EVH [3,4].
The current first-line treatment for GVH is endoscopic gastric variceal obliteration (GVO) using N-butyl-2-cyanoacrylate (NBC; Histoacryl, B. Braun-Melsungen AG, Melsungen, Germany) [5,6]. NBC is liquid glue that polymerizes as a plastic cast upon contact with blood in the varix, which effectively controls active variceal bleeding. The initial use of NBC for GVO resulted in hemostasis in 70% to 100% of patients with acute GVH and was associated with a low complication rate [6-8]. However, the rebleeding rate was reported to range from 14% to 35% once acute GVH was controlled by GVO using NBC [6,9,10].
Mucosal ulceration is one of the delayed complications associated with sclerotherapy for variceal hemorrhages [11]. A small retrospective cohort study reported that NBC injections induced ulcers at a rate of 15.1% and caused recurrent bleeding [8,12]. Previous studies have reported on the efficacy of acid suppression for esophageal ulcer prophylaxis following endoscopic variceal ligation (EVL) and injection sclerotherapy in cases of EVH [13-15]. Some studies have shown that proton pump inhibitors (PPIs) reduce EVH and the size of post-banding ulcers following EVL [14,15]. However, data that describe the relationship between GVO-induced ulcers and rebleeding are scarce. Moreover, the efficacy of PPIs in prophylaxis of GVO-induced ulcers and rebleeding has not been evaluated for GV. The aim of this study was to assess the efficacy of PPIs in cases of rebleeding and bleeding-related death rates after GVO using NBC in patients with GVH.
METHODS
Patients
This was a retrospective case-control study conducted in 341 patients who were diagnosed with bleeding GV and had undergone GVO using NBC at Chonnam National University Hospital (Gwangju, Korea) from January 2004 to July 2013. Patients who were diagnosed with bleeding GV and treated at other institutions before being referred to our center were excluded from the study. We also excluded isolated GV bleeding. Patients were followed up until death or until July 2013. The patients were divided into two groups: the PPI and non-PPI groups. Patients in the PPI group (n = 219) had received 40 mg pantoprazole daily for at least 1 month from the day of hospital admission. Patients in the non-PPI group (n = 122) had not received any anti-secretory treatment. All patients had received intravenous third-generation cephalosporins and vasoactive drugs, such as terlipressin or somatostatin, immediately before endoscopy or during endoscopy, and these medications were continued for up to 5 days afterwards, in accordance with published guidelines [16]. The dose of a non-selective β-blocker was titrated according to the patient’s heart rate (55 to 60 beats per minute) and systolic blood pressure (90 to 100 mmHg) if possible.
All data, including patient demographics, etiology of GVs, Child-Pugh scores, endoscopic findings, the effectiveness of endoscopic treatments, and clinical and endoscopic follow-up data, were recorded and analyzed. After GVO, follow-up endoscopies were performed before the patients were discharged from the hospital, if possible (Fig. 1). All patients provided written informed consent to undergo endoscopy.
Flow chart showing study recruitment and follow-up. GV, gastric varice; PPI, proton pump inhibitor; EGD, esophagogastroduodenoscopy.
Endoscopic GVO using Histoacryl
Patients who had upper gastrointestinal (UGI) bleeding and features indicative of cirrhosis had undergone upper endoscopy within 12 hours after admission to the hospital. Endoscopy was performed using a forward-viewing endoscope (Olympus GIF Q 260, Olympus, Tokyo, Japan).
Histoacryl was prepared as described below. The injection needle was primed with distilled water, followed by a 1:1 mixture of Histoacryl and Lipiodol (iodized oil, Laboratoire Guerbet, Roissy-Charles-de-Gaulle Cedex, France) injected as a bolus dose of 1 to 4 mL, depending on the size of the gastric varix. Sclerotherapy was performed using a disposable 2.3-mm diameter sclerotherapy needle (MTW, Endoskopie, Wesel, Germany). The catheter was introduced into the working channel of the endoscope and advanced. Once the bleeding varix was located, the needle was exposed and inserted into the base of the varix and the Histoacryl-Lipiodol mixture was injected by an endoscopy assistant. Upon removal of the needle from the varix, the assistant injected normal saline to flush the remaining glue from the catheter. Injections were repeated until GVs appeared to occlude, as judged by probing using a blunt probe. Both the endoscopist and assistant wore safety spectacles to comply with safety guidelines and to reduce the likelihood of accidentally spraying NBC into the eyes, which could cause glue-induced damage.
Definitions
GVs were grouped into two categories using the classification of Sarin and Kumar [1]. In this classification, type 1 gastroesophageal varices (GOV1) appear as a continuation of esophageal varices (EVs) and extend 2 to 5 cm below the gastroesophageal junction (GEJ), while type 2 GOV (GOV2) extend beyond the GEJ into the fundus of the stomach [1]. GVs were classified into three types, tortuous (F1), nodular (F2), and tumorous (F3), using the system proposed by Hashizume et al. [17]. Active GV bleeding was defined as blood actively spurting or oozing from a varix, and evidence of recent bleeding was defined as the presence of a white nipple or red plugs.
The efficacy of Histoacryl in successful GVO was assessed by probing the varix with the injection catheter. If it remained soft, an additional injection was initiated to achieve complete obliteration, defined as absolute firmness of the injected varix. Initial hemostasis was considered successful when bleeding had been arrested and no recurrence was observed for 2 days [10]. Rebleeding was defined as a new onset of hematemesis and the presence of coffee-ground vomitus, hematochezia, or melena accompanied by an increased pulse rate of > 100 beats per minute and a decrease in blood pressure to < 90 mmHg, following a 24-hour period of stable vital signs and hemoglobin levels after endoscopic treatment [18]. Bleeding-related death was defined as death within 6 weeks of the index bleed [19]. A Histoacryl-induced ulcer was defined as a mucosal break ≥ 3 mm deep at a site where Histoacryl had been injected previously (Fig. 2).
Endoscopic gastric variceal obliteration (GVO) using Histoacryl (B. Braun-Melsungen AG). (A) Bleeding gastric varix before GVO. (B) GVO-induced ulceration.
Ethics statement
Written informed consent was obtained from all the patients regarding the nature and purpose of the treatment, and this study was approved by the Institutional Review Board of Chonnam National University Hospital (CNUH-2013-191).
Statistical analysis
Statistical analyses were performed using SPSS version 20.0 (IBM Co., Armonk, NY, USA). Continuous variables are expressed as means ± standard deviation. Student t test and Pearson chi-square test were used to compare baseline characteristics of the patients. Significant factors identified by univariate analysis were entered into a stepwise multivariate logistic regression analysis to distinguish the risk factors that retained statistical significance from those that merely depended on other factors. The rebleeding rate was estimated using Kaplan-Meier curves and compared using the log-rank test. The null hypothesis of no difference was rejected if p < 0.05, or if the 95% confidence intervals (CI) of the odds ratio (OR) estimates excluded one.
RESULTS
Baseline characteristics
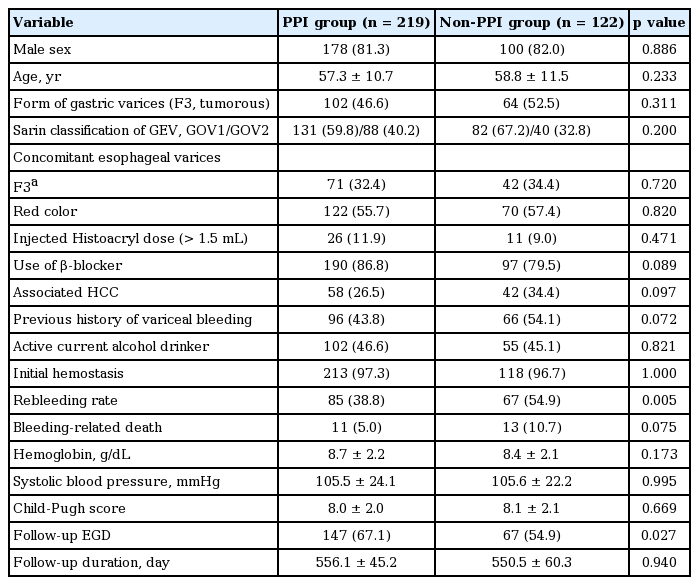
The baseline demographic and clinical characteristics of the patients are shown in Tables 1 and 2. There were no significant differences in the baseline clinical characteristics between the PPI and non-PPI groups except the follow-up esophagogastroduodenoscopy (EGD) rate, which was higher in the PPI groups than the non-PPI group (p = 0.027).
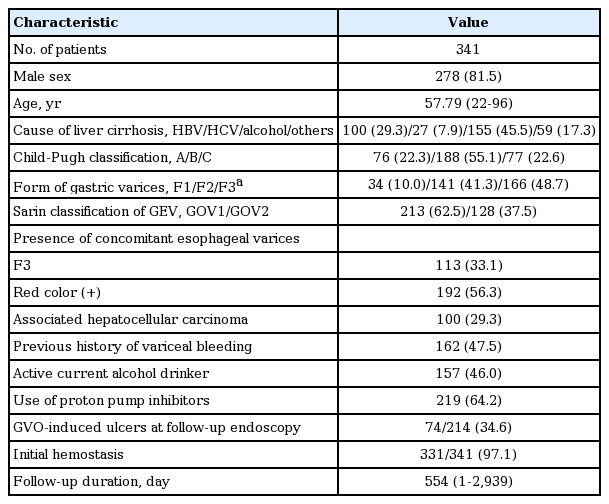
Baseline clinical characteristics of the patients enrolled in the study
Clinical characteristics of the patients at study initiation
A total of 341 patients were enrolled in this study. Of these, 219 (64.2%) in the PPI group received 40 mg pantoprazole daily for at least 1 month from the time of hospital admission, and 122 (35.8%) in the non-PPI group did not receive any anti-secretory treatment. The mean age of the patients was 57.8 years (range, 22 to 96), with 278 males (81.5%) and 63 females (18.5%). Of the patients evaluated, 100 (29.3%) were positive for the hepatitis B surface antigen, 27 (7.9%) were positive for hepatitis C virus antibodies, 155 (45.5%) were chronic alcohol drinkers and 59 (17.3%) had a combined etiology.
Patients were grouped according to the Child-Pugh classification to assess the prognosis of chronic liver disease. There were 76 class A patients (22.3%), 188 class B patients (55.1%), and 77 class C patients (22.6%). Of the patients evaluated, 100 (29.3%) had concomitant hepatocellular carcinomas, and 162 (47.5%) had a previous history of variceal bleeding. Patients were also classified based on the type of GV. There were 213 patients (62.5%) classified as GOV1, 128 (37.5%) as GOV2, 34 (10.0%) had an F1 form of GV, 141 (41.3%) had an F2 form of GV, and 166 (48.7%) had an F3 form of GV. The rate of initial hemostasis was 97.1%. The mean follow-up duration was 554 days (range, 1 to 2,939).
Clinical outcomes after GVO using NBC
Kaplan-Meier analysis demonstrated that rebleeding occurred in 0.3% of patients within 1 week, 2.2% of patients within 2 weeks, 3.9% of patients within 4 weeks, 18.9% of patients within 6 months, and 27.6% of patients within 12 months (Table 3, Fig. 3A). The probability of rebleeding in the PPI group was lower than that in the non-PPI group (log rank test, p = 0.009) (Fig. 3B). Bleeding-related death occurred in 7% of patients. There were also 123 (36.1%) adverse events during the study, including the follow-up period. These adverse events included GVO-induced ulceration in 74 of 214 patients (34.6%), fever in 26 (7.6%), abdominal pain in 13 (3.8%), diarrhea in four (1.2%), bacteremia in two (0.6%), spontaneous bacterial peritonitis in two (0.6% ), embolism in one (0.3%), and pseudomembranous colitis in one (0.3%) (Table 3).
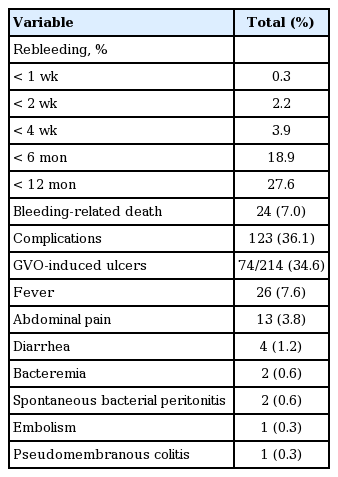
Clinical outcomes after gastric variceal obliteration using N-butyl-2-cyanoacrylate (n = 341)

(A) Cumulative probability of no rebleeding. (B) Kaplan-Meier analysis demonstrates that the rebleeding rate was lower in the proton pump inhibitor (PPI) group than the non-PPI group (log rank test, p = 0.009).
Risk factors for rebleeding
Univariate analysis showed that use of PPIs (relative risk [RR], 0.496; 95% CI, 0.307 to 0.801; p = 0.004) and a previous history of variceal bleeding (RR, 1.918; 95% CI, 1.195 to 3.078; p = 0.007) were associated with rebleeding. Multivariate analyses of the risk factors for rebleeding are shown in Table 4.

Multivariate analysis of potential risk factors for rebleeding
Risk factors for rebleeding in the follow-up EGD group
Univariate analysis showed that use of PPIs (RR, 0.436; 95% CI, 0.222 to 0.857; p = 0.016) and a previous history of variceal bleeding (RR, 3.257; 95% CI, 1.701 to 6.25; p < 0.001) were associated with rebleeding in the follow-up EGD group. Multivariate analyses of risk factors for rebleeding were use of PPIs (RR, 0.487; 95% CI, 0.262 to 0.903; p = 0.022) and a previous history of variceal bleeding (RR, 3.067; 95% CI, 1.742 to 5.405; p < 0.001). However, GVO-induced ulcer was not associated with rebleeding (p = 0.799).
Risk factors for bleeding-related death
Univariate analysis showed that Child-Pugh class C (RR, 16.564; 95% CI, 4.764 to 57.594; p < 0.001), failure of the initial hemostasis (RR, 15.027; 95% CI, 2.318 to 97.408; p = 0.004), use of a β-blocker (RR, 0.153; 95% CI, 0.040 to 0.584; p = 0.006), and presence of concomitant red-colored EV (RR, 5.341; 95% CI, 1.263 to 222.589; p = 0.023) were associated with bleeding-related death, while PPI use (RR, 0.582; 95% CI, 0.196 to 1.730; p = 0.330) was not. Multivariate analyses of the risk factors for rebleeding are shown in Table 5.
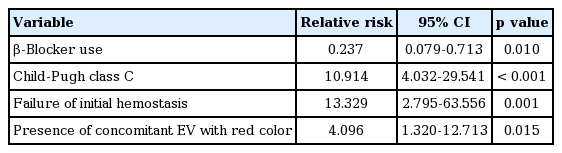
Multivariate analysis of potential risk factors for bleeding-related death
DISCUSSION
This is the first large study to assess GVO-induced ulceration and the association of PPIs with rebleeding or bleeding-related deaths. A distinct and novel finding of this study is that prophylactic use of PPIs reduces rebleeding, but not bleeding-related death, after GVO using NBC in patients with GVH.
GVH is characterized by more severe blood loss and higher mortality rates compared with EVH, and its clinical management presents a greater challenge than that of EVH [3,19,20]. The reasons for these differences are: (1) GVs are located deeper within the submucosa and are larger than EVs; (2) GVs are exposed to acid and pepsin; and (3) the folds in the gastric mucosa that cause blood pooling in the fundus and the high posterior gastric wall make GV diagnosis difficult [2,21]. PPIs are the most potent pharmacological agents for inhibition of gastric acid secretion. Therefore, these agents are the logical candidates to assess the effect of gastric acid on post-GVO complications.
Toriumi et al. [22] reported that subcutaneous application of Histoacryl may cause mild acute inflammation and chronic foreign body giant cell reactions. These findings suggest that sclerotherapy using Histoacryl may induce ulceration in patients with GVH. Although some studies have shown that PPIs reduce the incidence of esophageal hemorrhage and the size of post-EVL ulcers in EVH, few studies have described the efficacy of PPIs in the prophylaxis of GVO-induced ulcers, rebleeding, and/or bleeding-related deaths [14,15].
In the present study, initial hemostasis using NBC injections was achieved at a rate of 97.1%, which is consistent with rates of 90% to 97% reported in other studies [23,24]. Huang et al. [6] reported that rebleeding occurred in 23.3% of the patients over a period of 3 days to 16 months after GVO. In this study, rebleeding occurred in 0.3% of patients within 1 week, 2.2% of patients within 2 weeks, 3.9% of patients within 4 weeks, 18.9% of patients within 6 months, and 27.6% of patients within 12 months of the GVO procedure, which is consistent with previous reports [6].
We also evaluated risk factors for rebleeding after treatment and found that no PPI use and a previous history of UGI bleeding were associated with rebleeding. The type and size of GVs were not associated with risk factors for rebleeding, which is inconsistent with the results of other studies [3,24]. These results showed that rebleeding may be associated with no PPI use. We speculated that use of PPIs could reduce mucosal ulceration and, hence, ulceration-related GV bleeding. Although, in the follow-up EGD group, GVO-induced ulcer was not associated with rebleeding, and only a portion of patients received follow-up EGD. Moreover, most of these patients received follow-up EGD within 2 weeks after variceal bleeding (mean 12 ± 16.2 days) before development of delayed mucosal ulceration. Therefore, it is too early to conclude that the GVO-induced ulcer did not induce rebleeding.
The Child-Pugh score was not associated with rebleeding but bleeding-related death, which was found to be 7.0% in this study, consistent with other studies [7,10]. Another study showed that the mortality rare due to rebleeding immediately after NBC sclerotherapy was 12.5% [6]. Risk factors for bleeding-related death included no use of β-blockers, Child-Pugh score, and the presence of concomitant red-colored EV and failure of the initial hemostasis. Interestingly, PPIs did not reduce bleeding-related death. Other studies have shown that liver health, rapid and effective variceal hemostasis and complete and lasting obliteration of GVs impact bleeding-related deaths [10,23].
In this study, mucosal ulceration occurred in 34.6% of patients in the endoscopy follow-up group. Some studies have reported that mucosal ulceration, at a rate of 15.1% to 90%, is a common complication after GVO using NBC [6,8], which was consistent with our study.
There are several limitations to our study. First, its retrospective, single-center design limits generalization of the results across other patient populations. Second, not all patients underwent follow-up endoscopy; therefore, the rate of mucosal ulceration may not be accurate. Third, there was a lack of information regarding other drugs prescribed to the patients, including non-steroidal anti-inflammatory drugs. Fourth, the interval between the GVO and follow-up endoscopy was short (usually 7 to 10 days), which might have affected the NBC, causing chronic granulomatous inflammation, further contributing to an inaccurate rate of mucosal ulceration. In addition, long-term acid suppression with PPIs may be needed to heal ulcers, and we only assessed the effects of PPIs for 1 month or longer. Thus, larger, prospective, randomized studies will be needed to confirm the efficacy of PPI prophylaxis in relation to rebleeding and bleeding-related deaths in patients with GVH.
In conclusion, this large retrospective case control study showed that the prophylactic use of PPIs reduces rebleeding, but not bleeding-related death, after GVO using NBC in patients with GVH.
KEY MESSAGE
1. The rate of initial hemostasis of gastric variceal obliteration (GVO) using N-butyl-2-cyanoacrylate (NBC) in patients with gastric variceal hemorrhages (GVH) was 97.1%.
2. Rebleeding occurred in 0.3% of patients within 1 week, 2.2% of patients within 2 weeks, 3.9% of patients within 4 weeks, 18.9% of patients within 6 months, and 27.6% of patients within 12 months of the GVO procedure.
3. The prophylactic use of proton pump inhibitors reduces rebleeding, but not bleeding-related death, after GVO using NBC in patients with GVH.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was supported by grants from Chonnam National University Hospital, Gwangju, Korea.