Percutaneous Coronary Intervention Versus Coronary Artery Bypass Grafting in Patients with Coronary Artery Disease and Diabetic Nephropathy: A Single Center Experience
Article information
Abstract
Background
Patients with diabetic nephropathy (DN) and coronary artery disease (CAD) represent a subset of patients with high cardiovascular morbidity and mortality. The optimal revascularization strategy using either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) remains controversial. The purpose of this study was to compare the clinical outcomes of PCI to CABG in DN patients with CAD.
Methods
The clinical and angiographic records of DN patients with CAD who underwent either CABG (n=52) or PCI (n=48) were retrospectively analyzed.
Results
The baseline characteristics were similar in the two groups except for the severity of the CAD. At 30 days, the death rate (PCI: 2.1% vs. CABG: 9.6%, p=0.21) and major adverse cardiac events (MACE) rate (PCI: 2.1% vs. CABG: 9.6%, p=0.21) were similar in comparisons between the PCI and CABG groups. At three years, the death rate (PCI: 18.8% vs. CABG: 19.2%, p=0.94) was similar between the PCI and CABG groups but the MACE rate (PCI: 47.9% vs. CABG: 21.2%, p=0.006) was higher in the PCI group compared to the CABG group. In addition, the repeat revascularization rate was higher in the PCI group compared to the CABG group (PCI: 12.5% vs. CABG: 1.9%, p=0.046).
Conclusions
The CABG procedure was associated with a lower incidence of MACE and repeat revascularization for up to three years of follow-up in DN patients with CAD. However, the overall survival rate was similar in the CABG and PCI groups. Therefore, CABG may be superior to PCI with regard to MACE and repeat revascularization.
INTRODUCTION
Coronary artery disease (CAD) is highly prevalent in patients with diabetic nephropathy (DN) and the incidence of DN is increasing worldwide. Compared to nondiabetic patients, the postoperative morbidity and mortality are higher in diabetic patients after coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI)1-3). Furthermore, the DN patients with CAD are a special subset of diabetic patients, who are known to be at a higher risk compared to diabetic patients without nephropathy4). The selection of the most appropriate revascularization strategy is important for improved patient survival in DN patients with CAD. Angioplasty for multivessel CAD has become increasingly common for high-risk patients with comorbidities. However, a major drawback of percutaneous transluminal coronary angioplasty is the abrupt vessel closure and higher restenosis rates compared to the CABG procedure. Technical advances such as the use of a coronary stent have decreased the restenosis rates. However, CABG offers the advantage of a more complete revascularization regardless of the coronary anatomy at the time of the procedure. Randomized trials of surgical therapy have shown that the benefits of surgical revascularization are proportional to the amount of myocardium affected by, or at risk for, ischemic injury5). Although, perioperative morbidity and mortality, duration of hospital stay and hospital cost is higher for CABG, several randomized clinical trials including the BARI (Bypass Angioplasty Revascularization Investigation) have suggested that CABG provided superior outcomes in the subgroup of diabetic patients due to better long-term patency of the grafts compared to PCI6,7). Therefore, contemporary PCI guidelines emphasize the long-term survival benefit with CABG for treatment of diabetics with multivessel CAD8). By contrast, survival data of 8818 patients derived from seven registries showed a long-term mortality (5-12 years) of 27.8% in patients treated by PCI and 26.3% in patients treated by CABG, revealing a mortality rate similar for the two groups9). The reason for the discrepancy between the subgroup analysis of the clinical and observational data is unclear, even though it is well known that CABG patient registries are usually much more clinically compromised than those for patients undergoing PCI. Although CABG appeared to provide a better outcome than PCI, most of the findings were obtained by subanalyses, without a focus on DN patients.
The purpose of this study was to compare the clinical outcomes of a subset of diabetic patients with high cardiovascular risk, DN patients with CAD, following PCI or CABG.
MATERIALS AND METHODS
Patients
All clinical records and catheterization reports of type 2 diabetic patients with nephropathy who underwent PCI or CABG at our institution from January 1, 1996 to December 31, 2005 were retrospectively analyzed regarding clinical and angiographic data. Diabetic nephropathy was defined as overt proteinuria (proteinuria > 500 mg/day) or a glomerular filtration rate (GFR) by the modified MDRD (Modification of Diet in Renal Disease) equation10) of less than 60 mL/min/1.73 m2. The revascularization strategy was determined by the clinical judgment of the cardiologists and cardiac surgeons. In Brief, PCI was recommended for patients with single- or two-vessel disease with normal or slightly depressed global left ventricular function and for those with lesions anatomically suitable for the procedure. Whereas, surgery was preferred for patients with left main CAD or those who had two- or three-vessel disease with impaired global left ventricular function (left ventricular ejection fraction < 45%) or other lesions unsuitable for catheter- based procedures. Repeat revascularization was defined as angiographic ballooning or stenting due to angiographic restenosis at the site of previous stent deployment or graft, the development of new lesions or progression of untreated lesions on a coronary angiogram.
Pecutaneous coronary intervention procedures
Coronary angiography was performed by the femoral approach according to standard techniques. At least six standardized projections of the left coronary artery and two of the right coronary artery were obtained. The severity of the coronary artery disease was determined visually and was classified as single, double or triple vessel disease, defined by the presence of hemodynamically relevant stenosis (stenosis > 50% of the luminal diameter) in one of the three major coronary vessels. A coronary lesion with critical stenosis (stenosis > 70% of the luminal diameter) was selected for coronary balloon angioplasty and stenting. Balloon angioplasty and commercially available bare metal stent implantation were performed according to standard techniques. The stent was deployed at the culprit lesion by inflating a balloon; inflation of the balloon expanded the stent. After the implantation of the stent, the stented area was often dilated further by standard balloon angioplasty techniques. The patients received 500 mg aspirin and 10,000 IU of heparin before the procedure. All patients were advised to take lifelong maintenance aspirin and another antiplatelet agent (clopidogrel, ticlopidine or cilostazol).
Coronary artery bypass grafting
The bypass surgery followed current standard techniques, preferably with a left internal mammary artery for revascularization of the left anterior descending coronary artery. Standard operative techniques for on-pump CABG for patients were used, including standard cardiopulmonary bypass, moderate hypothermia and cold potassium cardioplegia for myocardial protection. Off-pump CABG was performed using mechanical stabilization and intravascular shunting of the target coronary arteries.
Composite end points
The primary clinical end points were major adverse cardiac events (MACE) including death, myocardial infarction and repeat revascularization at 30 days, one year and three years. The secondary clinical end points were procedure related complications including stroke, post-procedural bleeding, pneumonia, renal failure requiring dialysis, and atrial flutter/atrial fibrillation at 30 days.
Statistical analysis
Continuous variables were expressed as mean±SD and were compared in the CABG and PCI groups by the Student's t-test. Categorical variables are presented as percentages and were compared by the chi-square test. For MACE, the event time was the number of days from the initial procedure to the first event. Time to death, time to MACE and time to repeat revascularization were evaluated at 30 days, one year and three years. Survival curves were generated using the Kaplan-Meier method. The Log-rank test was used to compare survival rates between CABG and PCI groups. In the subgroup analysis of CABG, according to type of surgery or graft, the Fisher's exact test was used to obtain the correlation of off-pump CABG or internal mammary artery with MACE or death. The multivariable Cox proportional hazards model was used to evaluate baseline clinical and angiographic characteristics and procedure-related variables in order to identify independent predictors of death and MACE. All statistical tests were two-tailed, and a significance level of 0.05 was used throughout. Statistical analyses were performed using SPSS version 12.0 (SPSS Inc., Chicago, Illinois, USA).
RESULTS
Baseline clinical characteristics and revascularization data
The pretreatment demographic and clinical characteristics and risk factors in the PCI and CABG groups were comparable, except for a significantly higher number of smokers in the PCI group and a greater number of patients presenting with myocardial infarction in the CABG group (Table 1). The CABG group had significantly more left main CAD (PCI group: 0% vs. CABG group: 21.2%, p= 0.001) and three vessel CAD (PCI: 33.3% vs. CABG: 84.6%, p<0.001). The number of lesions with a greater than 50% stenosis was significantly higher in CABG group (PCI: 3.6±1.6 vs. CABG: 5.1±2.0, p<0.001) (Table 1).
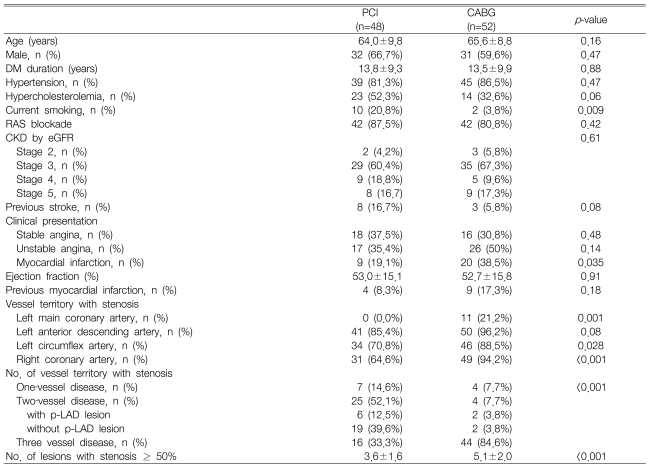
Baseline clinical and angiographic characteristics
Off-pump CABG was performed in 44.2% of the patients in the CABG group; using a mean of 2.5±1.4 grafts per patient. An internal mammary artery graft to the left anterior descending artery was used in 88.5% of CABG patients (Table 2).
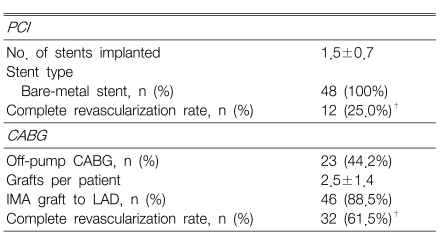
Procedural characteristics for PCI and CABG
Commercially available bare metal stents were used in the PCI group. The number of lesions revascularized was significantly smaller in the PCI group than in the CABG group (PCI: 1.5±0.7 stents vs. CABG: 2.5±1.4 grafts, p<0.001). The complete revascularization rate was higher in the CABG group (PCI: 25.0% versus CABG: 61.5%, p<0.001) (Table 2).
30-day clinical outcomes
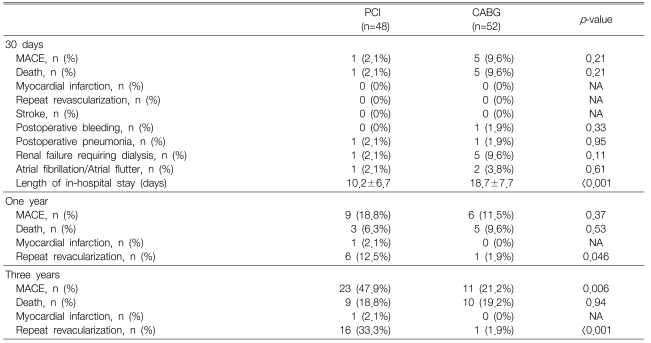
In the CABG group, five patients died (9.6%) because of cardiogenic shock (n=2), hypovolemic shock due to postoperative bleeding (n=1), respiratory failure due to a possible stroke (n=1), and sepsis due to pneumonia (n=1). There was a spectrum of secondary adverse events in the CABG group: renal failure requiring dialysis (n=5), atrial fibrillation/atrial flutter (n=2), postoperative lung hemorrhage (n=1), and pneumonia (n=1). In the PCI group, one patient died due to cardiogenic shock. Secondary adverse events in the PCI group included renal failure requiring dialysis (n=1) and postoperative pneumonia (n=1). The MACE and death rates were comparable in the CABG and PCI groups (p=0.21) and the mean hospital stay was significantly shortened in the PCI group (PCI: 10.2±6.7 vs. CABG: 18.7±7.7, p<0.001) (Table 3).
30-day, one-year and three-year clinical outcomes
One-year clinical outcomes
Between 31 days and one year, there were two deaths in the PCI group, one of which was cardiac related (sudden death possibly due to stent thrombosis). Between 31 days and one year, one patient in the PCI group had a myocardial infarction. This patient had an acute anterior wall myocardial infarction due to thrombotic occlusion of a first diagonal branch that had previously been stented.
The MACE and death rates were comparable between the CABG and PCI groups while repeat revascularization rates were significantly higher in the PCI group (PCI: 12.5% vs. CABG: 1.9%, p=0.046) (Table 3, Figure 1).
Kaplan-Meier estimates of overall survival (A), MACE-free survival (B) and reintervention-free survival (C) at one year. Cum Survival, cumulative survival; MACE, major adverse cardiac event; CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention.
Three-year clinical outcomes
Between one year and three years, there were six deaths in the PCI group and five deaths in the CABG group. The causes of death assigned to the PCI group were as follows: acute myocardial infarction (two patients), cerebral hemorrhage (one patient), aspiration pneumonia (one patient), renal failure (one patient), and cancer (one patient). In the CABG group, the causes of death were acute myocardial infarction (one patient), sepsis due to urinary tract infection (two patients) and sudden death (one patient).
The MACE rate was lower in the CABG group than in the PCI group (PCI: 47.9% vs. CABG: 21.2%, p=0.006) and the death rate was comparable in the CABG and PCI groups (p=0.94). The repeat revascularization rate was significantly lower in the CABG group (PCI: 33.3% vs. CABG: 1.9%, p<0.001) (Table 3, Figure 2).
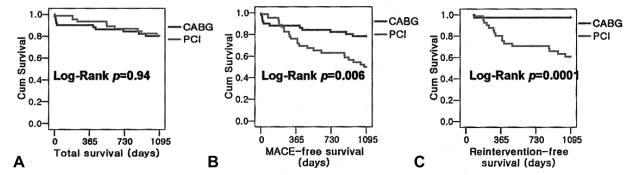
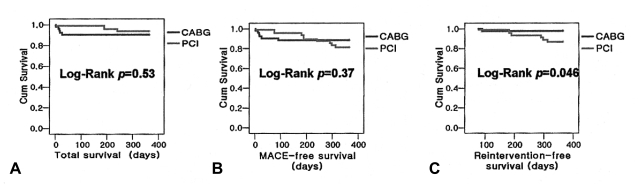
Kaplan-Meier estimates of total survival (A), MACE-free survival (B) and reintervention-free survival (C) at three years. Cum Survival, cumulative survival; MACE, major adverse cardiac event; CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention.
Subgroup analysis of the CABG group showed that the off-pump CABG and the on-pump CABG were not different in the death (off-pump CABG: 13% vs. on-pump CABG: 25%, p=0.48) and MACE rates (off-pump CABG: 17.4% vs. on-pump CABG: 25%, p=0.73). Internal mammary artery grafts provided greater protection from death (internal mammary artery grafts: 13.3% vs. saphenous vein grafts: 66.7%, p=0.01, odds ratio=0.077) and MACE (internal mammary artery grafts: 15.6% vs. saphenous vein grafts: 66.7%, p=0.015, odds ratio=0.092) than the saphenous vein grafts.
Predictors of MACE and death
The following variables were entered into a stepwise multivariable Cox proportional hazards model for MACE: age, gender, smoking history, GFR by the MDRD study equation, Ca X P product, uric acid, ejection fraction, myocardial infarction, prior stroke, peripheral vascular disease, therapy of lipidlowering drug, and type of revascularization (CABG or PCI). The Cox proportional hazards regression model demonstrated that smoking history was a positive independent predictor (hazard ratio: HR, 1.030, 95% CI, 1.006 to 1.055) and CABG was a negative independent predictor (hazard ratio: HR, 0.189, 95% CI, 0.064 to 0.556) of MACE (Table 4).

Independent predictors for MACE and death
The Cox proportional hazard regression model for death demonstrated that myocardial infarction was a positive independent predictor (hazard ratio: HR, 5.671, 95% CI, 1.230 to 26.134) and higher GFR by the modified MDRD study equation was a negative independent predictor (hazard ratio: HR, 0.921, 95% CI, 0.876 to 0.969) of death (Table 4).
DISCUSSION
This retrospective, observational study compared the clinical outcomes between PCI and CABG in DN patients with CAD. The overall survival was similar in the CABG and PCI groups but the MACE rates and incidence of repeat revascularization were significantly higher in the PCI group compared to the CABG group during follow up. PCI has been shown to be effective in reducing clinical symptoms in patients with CAD and myocardial ischemia. PCI may be the preferred strategy of myocardial revascularization in patients with serious systemic illness such as chronic renal failure and ESRD. The PCI procedures are less invasive than CABG and therefore are associated with less physical and psychological trauma. Compared to PCI, CABG is more invasive and the perioperative mortality and morbidity is very high especially in chronic renal failure patients. Furthermore, a longer hospital stay following CABG results in higher hospital costs. It has been generally accepted that CABG is the preferred revascularization modality in DN patients with left main CAD or multivessel disease (three vessel or two vessel disease including proximal left anterior coronary artery lesion) with impaired left ventricular function (ejection fraction < 0.35) or complex lesions (total occlusion, calcified lesions, or bifurcation lesions)11). CABG has been associated with a higher incidence of significant adverse postoperative events. Therefore, in patients with serious illness such as chronic renal failure and ESRD, PCI can be an attractive alternative revascularization strategy to CABG. However, previously reported data do not provide support for either CABG or PCI as an initial strategy for diabetics with multivessel CAD who are at a high risk for adverse outcomes with CABG.
Our study on patients with DN showed that PCI resulted in outcomes comparable to CABG with respect to survival at three years. However, the repeat revascularization and MACE rates were significantly higher in the PCI group than in the CABG group at three years after the procedure. The anatomical patterns of CAD in the diabetic patients may influence their prognosis and response to revascularization. Previous studies have demonstrated that diabetic patients more frequently have left main coronary artery lesions, multivessel disease and diffuse CAD12,13). Our study results demonstrated that the CABG group had left main coronary artery lesions, multivessel disease, and diffuse CAD more frequently than the PCI group. However, the significantly higher complete revascularization rate in the CABG group (PCI: 25.0% vs. CABG: 61.5%, p<0.001) may have influenced the clinical outcomes. Until recently, no prospective trial has compared CABG with PCI in DN patients; post hoc analysis of trials has suggested favorable results with CABG in diabetics. The Arterial Revascularization Therapy Study (ARTS) compared the relative efficacy of CABG and multivessel bare metal stenting in diabetics and non-diabetics14). This study showed no difference in mortality between PCI and CABG in this subset of diabetics at one year. However, the revascularization rate clinically necessary in diabetics treated with PCI was twice as high as the revascularization rate in diabetics treated with CABG. The BARI reported that for patients who had diabetes, and symptomatic multivessel disease, CABG resulted in an improved five year survival rate (81%) compared to PTCA (65%). However, < 20% of patients had diabetes6). A large observational study of patients with multivessel disease reported that CABG was associated with higher adjusted long-term survival outcomes than PCI15). The CABG group included patients with diabetes (33%), while 25% of the stented group were patients with diabetes. After the subgroup analysis of the patients with diabetes, hazard ratios for death were generally lower after CABG than after PCI. In the ARTS, 25% of patients had chronic kidney disease (CKD) at entry. CABG was associated with a reduced risk for revascularization compared with PCI10). In a recent meta-analysis, data were too sparse on renal disease patients to draw any definite conclusion16). However, the newly published Kidney Disease Outcomes Quality Initiative guidelines emphasized that outcomes in dialysis patients with established CAD are worse than outcomes in the general population. The guidelines support CABG as the preferred therapy for ESRD patients with three-vessel or left main CAD17). The complete revascularization rate with PCI in CKD patients ranges from only 25% to 50%18). Patients who have CKD and undergo PCI were more likely to have peripheral vascular disease, cerebrovascular disease, hypertension, and diabetes and may have clinically silent CAD19). The largest ESRD population studied was the US Renal Data System national database between 1978 and 1995. In nearly 7,000 dialysis patients who underwent an initial PCI, the two-year survival rate was roughly 50%. Using the Cox regression model in this retrospective comparison, Herzog et al. showed that dialysis patients in the United States had better survival rates after CABG than after PCI20). Le Feuvre et al. reported a primary success rate of 96% in 21 dialysis patients, and the need for repeat intervention was similar to 187 control participants (30% vs. 25%). However, at two years, the rate of cardiac death was 15%, compared with 5% in the control group21). Furthermore, there was no significant difference in the mortality rate between PCI and CABG groups if they had the same left ventricular function22). Our study group was unique with regard to including patients with diabetes and nephropathy. Patients were included with CKD from stage 3 to stage 5 (95% of whole patients) and ESRD patients on dialysis (17% of whole patients). Diabetes mellitus and CKD are increasing in the general population and many of these patients require coronary revascularization procedures because of CAD. Renal insufficiency was reported as an independent predictor of the one-year mortality after PCI in a previous study19). Our study showed that decreased renal function was an independent predictor of the three-year mortality after PCI or CABG.
Moreover, our study showed that the repeat revascularization rate was significantly higher in the PCI group compared to the CABG group. This observation may result from the fact that CABG is not associated with stent restenosis or stent thrombosis, and that arterial grafts may protect vessels from atherosclerotic progression and plaque rupture23, 24). In our study, about 89% of patients who had a CABG underwent an internal mammary artery graft. Progressive atherosclerosis was responsible for repeat revascularization in a significant number of diabetic patients25, 26). Progression of non-stented lesions was the reason for revascularization in 56% of patients who required repeat revascularization in our study. Furthermore, CABG provided a more complete revascularization rate than PCI (CABG: 61.5% vs. PCI: 25.0%, p<0.001). If one could effectively reduce restenosis in PCI, PCI would be a more attractive treatment modality than CABG. Recently published data demonstrated that the use of drug-eluting stents (DES) dramatically reduced the incidence of restenosis27). However, the outcomes of the studies using DES were not conclusive. Ben-Gal et al. reported that the midterm clinical outcome of diabetic patients treated surgically was better than that of patients undergoing PCI with DES despite improved results of PCI with DES28). Our study did not include patients who received a PCI with DES because DES was only recently introduced at our hospital. The number of patients who received PCI with DES is very small so it is impossible to obtain statistically meaningful results by comparing clinical outcomes of PCI with the bare metal stent group or the CABG group at three years. Our results showed that the treatment modalities (PCI or CABG) affected the MACE rate. CABG may be the preferred treatment modality for prevention of restenosis and for reducing the hospital cost for reintervention. However, PCI may be preferred for revascularization in severely ill patients.
Study limitations
Our study has several important limitations. This study was a single-center, non-randomized, uncontrolled registry that requires validation by prospective randomized studies. Consequently, systematic comparison of long-term outcome was not available. The rate of MACE may be underestimated because of the absence of follow-up angiography and patient refusal of follow-up angiography and the possibility of silent ischemia. As only periprocedural, one-year and three-year outcomes were analyzed, a long-term follow-up study will be necessary to confirm our findings. Van Domburg et al. reported that a slight benefit, up to ten years, in favor of CABG among a diabetic subgroup was comparable to the results in the BARI trial. However, after ten years, both survival curves converged29). Another important limitation is that comparative studies of CABG and PCI can rapidly become outdated in view of evolving medical and technological procedural improvements. For example, triple therapy with antiplatelet agents (aspirin, clopidogrel and cilostazol), adjunctive use of glycoprotein IIb/IIIa inhibitor, new antirestenosis therapies such as DES, and coronary brachytherapy may reduce the need for reintervention and improve long-term outcome. In addition, surgical techniques for CABG continue to improve.
Conclusions
CABG was associated with a lower incidence of MACE and repeat revascularization in the up to three-year follow-up of DN patients with CAD. However, the overall survival rate was similar in the CABG and PCI groups. CABG may be superior to PCI during this timeframe with respect to MACE and the repeat revascularization rate.