Predialysis hyponatremia and mortality in elderly patients beginning to undergo hemodialysis
Article information
Abstract
Background/Aims
Predialysis hyponatremia has been recently reported to be associated with mortality in incident hemodialysis patients. However, whether hyponatremia is associated with unfavorable outcomes in elderly patients remains unknown. We hypothesized that nephrology referral inf luences hyponatremia, and aimed to define how nephrology referral affects the association between hyponatremia and mortality in the elderly.
Methods
We retrospectively assessed mortality in 599 incident hemodialysis patients aged ≥ 70 at a tertiary university hospital, between 2000 and 2010. We analyzed 90-day and 1-year all-cause mortality (ACM) in relation to predialysis serum sodium (sNa). We divided the patients into two groups according to predialysis glucose-corrected sNa: hyponatremia (< 135 mmol/L) and normonatremia (135 to 145 mmol/L).
Results
Low estimated glomerular filtration rate, high phosphorus, low albumin, nonpreparation of arteriovenous fistula or graft, and late referral were associated with a low sNa in the elderly. Among 599 patients, 106 and 174 patients died at the 90-day and 1-year follow-ups, respectively. Each 10-mmol/L increase in predialysis sNa tended to be associated with lower 90-day and 1-year ACM. When patients were stratified by nephrology referral, hyponatremia was associated with increased mortality in early referral group (90-day ACM: hazard ratio [HR] = 2.335, p = 0.041; 1-year ACM: HR = 1.790, p = 0.024). However, hyponatremia was not associated with mortality in late referral group.
Conclusions
Predialysis hyponatremia at hemodialysis initiation is associated with late referra
INTRODUCTION
Hyponatremia (serum sodium [sNa] concentration, < 135 mmol/L) is a common electrolyte disturbance among the geriatric population and is a cause of high morbidity and mortality [1-3]. The incidence of hyponatremia is higher in elderly patients than in younger patients because of age-associated abnormalities of water homeostasis, including changes in body composition, decrease in glomerular filtration rate (GFR), and hyper-responsiveness to arginine-vasopressin hormone with age [3,4]. Furthermore, elderly patients frequently use medications known to cause hyponatremia [3,5].
The incidence of hyponatremia may be high in patients with a chronic kidney disease (CKD), because these patients show a diminished ability to maintain water homeostasis [6,7]. Recently, a study showed that lower predialysis sNa concentration was associated with higher mortality in patients receiving maintenance and incident hemodialysis [8-10]. However, the relationship between predialysis hyponatremia and mortality in elderly patients beginning to undergo dialysis, who are a high-risk group for hyponatremia, has not been adequately evaluated. Therefore, we investigated the influence of hyponatremia on mortality in elderly patients undergoing incident hemodialysis.
Meanwhile, several studies have demonstrated the risk factors of hyponatremia in the dialysis population, such as malnutrition (hypoalbuminemia), lower residual renal function and estimated GFR, comorbidities, and infection [8-13]. Early nephrology referral and predialysis care was associated with the adequate control of risk factors related to CKD progression and complications, and risk factors of cardiovascular disease (i.e., nutrition, volume status, blood pressure, and anemia) [14-17]. Therefore, we hypothesize that nephrology referral affects sNa levels because predialysis care can control some of the risk factors related to hyponatremia, as discussed above. We investigated whether the timing of nephrology referral was associated with sNa concentration, and aimed to define how nephrology referral-associated hyponatremia affects the association between hyponatremia and mortality.
METHODS
Study population
The characteristics of the study population and design were published previously [18]. Between 2000 and 2010, there were 621 patients (age, ≥ 70 years) with end-stage renal disease (ESRD) who received incident hemodialysis at Seoul National University Hospital in Korea and whose predialysis data regarding sNa and glucose concentrations were available. We excluded the patients with sodium levels > 145 mmol/L as their number was too small to be included (n = 22). Consequently, 599 patients were included for this study. This study was approved by the Institutional Review Board of the Seoul National University Hospital (IRB No. H1107-092-370), with no written consent because patients records/information was anonymized and de-identified prior to analysis. All clinical investigations were conducted according to the 2008 Declaration of Helsinki and good clinical practice guidelines.
Measurements and definitions
The patients’ data were retrospectively collected via a review of their electronic medical records. Laboratory data at the last time before first hemodialysis session were recorded as baseline laboratory data. Supplementary Fig. 1 shows a frequency distribution histogram of the interval between the timing of lab data and that of dialysis initiation according to nephrology referral. The concentration of sNa was corrected for serum glucose concentration by using the following formula: measured sodium concentration + [0.016 × (serum glucose concentration − 100)] [19]. According to the corrected sodium concentrations, the patients were assigned to one of the two groups of predialysis sNa concentration: hyponatremia (< 135 mmol/L) and normonatremia (135 to 145 mmol/L). Early referral (ER) and late referral (LR) were defined depending on whether the patients first consulted a nephrologist more than or less than 3 months, respectively, before they were first diagnosed with ESRD. Serum creatinine concentrations were measured using the alkaline picrate Jaffe kinetic method with an automatic analyzer (Toshiba-200FR, Toshiba, Tokyo, Japan). Estimated GFR was calculated using the Modification of Diet in Renal Disease study equation [20]. Presence of hypertension at baseline was confirmed if the systolic blood pressure was ≥ 140 mmHg or the diastolic blood pressure was ≥ 90 mmHg, as determined by a physical examination, or on the basis of a self-reported history of the disease or use of antihypertensive medication. Presence of diabetes mellitus was confirmed if glycated hemoglobin concentration was ≥ 6.5, or on the basis of a self-reported history of the disease or use of antihyperglycemic agents. Information on comorbid illnesses was obtained from the International Classification of Disease, 10th Revision (ICD-10) database at the start of hemodialysis. In this study, we transformed these ICD-10 data to Charlson comorbidity index (CCI) scores using ICD-10 coding algorithm [21]. The CCI was scored at the start of hemodialysis using the definitions proposed by Charlson et al. [22].
Outcome
We combined 90-day and 1-year mortality data after dialysis initiation from Statistics Korea with our dataset, using each individual’s unique identifier [23].
Statistical analysis
Continuous variables were expressed as mean ± standard deviation values, and categorical variables were expressed as proportions. The concentration of sNa was presented as median (interquartile range [IQR]). Differences in continuous variables were analyzed using the Student t test and Mann-Whitney U test, and differences in categorical variables were analyzed using the chisquare test and Fisher exact test. The factors associated with sNa concentration were evaluated using a multivariable linear regression analysis. Cox’s hazard proportion analysis was used to estimate the hazard ratios (HRs) for 90-day and 1-year mortality caused by hyponatremia as a continuous and categorical variables stratified by nephrology referral. We conducted the test of proportional hazards assumptions and restricted cubic spline curves (Fig. 1). The Kaplan-Meier method was used to calculate the participant survival distribution (Figs. 2 and 3). Covariate selection for the regression model was based on the significance level in univariable analysis and clinical reasoning. To prevent co-linearity among the variables, we used the backward stepwise selection method. A p < 0.05 was considered statistically significant. All analyses and calculations were conducted using SPSS version 21.0 (IBM Corp., Armonk, NY, USA) and STATA version 14.0 (StataCorp LP, College Station, TX, USA).

The dose-response relationship between glucose-corrected predialysis sodium and 90-day/1-year all-cause mortality. (A) 90-day all-cause mortality, (B) 1-year all-cause mortality. The range area indicates 95% confidence intervals. A histogram of corrected predialysis sodium is also shown.
Kaplan-Meier survival curve for 90-day mortality according to serum sodium (hyponatremia vs. normonatremia) stratified by nephrology referral. (A) Early referral. (B) Late referral.

Kaplan-Meier survival for 1-year mortality according to serum sodium (hyponatremia vs. normonatremia) stratified by nephrology referral. (A) Early referral. (B) Late referral.
RESULTS
Patients’ characteristics according to the presence of hyponatremia
The mean age of the study cohort (n = 599) was 76.3 years, and 59.9% were men. At baseline, the median sodium concentration at dialysis initiation was 137.3 mmol/L (IQR, 133.6 to 140.0 mmol/L) (hyponatremia [sNa < 135 mmol/L, n = 191]; normonatremia [sNa 135 to 145 mmol/L, n = 408]). Among the subjects, 67.9% showed diabetes mellitus, 12.2% showed congestive heart failure (CHF), 4.0% showed liver cirrhosis, and 18.5% showed malignancy. The mean CCI score was 5.9. In the case of most of the patients (74.4%), hemodialysis was initiated using a central venous catheter (CVC). A comparison of the clinical characteristics according to sNa level at dialysis initiation, after stratification by the timing of nephrology referral, is presented in Table 1 and Supplementary Table 1. Patients in the hyponatremia group (n = 191) were older than patients in the normonatremia group (n = 408). Furthermore, the frequency of use of CVC, frequency of LR at the initiation of dialysis, white blood cell (WBC) count, and serum phosphorus concentration were higher, but estimated GFR and serum albumin concentration were lower, in the hyponatremia group than in the normonatremia group (Table 1). After stratification by the timing of nephrology referral, the proportion of patients with hyponatremia was higher in the LR group than in the ER group (47.3% vs. 22.2%). Patients in the hyponatremia group with ER were older, had a higher WBC count, and lower estimated GFR and serum albumin level than those in the normonatremia group (Supplementary Table 1). Supplementary Fig. 2 shows a frequency distribution histogram of glucose corrected sodium concentration after stratification by the timing of nephrology referral.

Baseline characteristics of patients according to serum sodium at the time of dialysis initiation
Factors associated with sNa concentration
In all of the patients, a higher sNa was associated with higher estimated GFR (r = 0.098, p = 0.022), lower phosphorus concentration (r = −0.116, p = 0.006), and higher albumin concentration (r = 0.113, p = 0.006). Furthermore, nonpreparation of arteriovenous fistula or arteriovenous graft (AVF/AVG) (r = −0.188, p < 0.001), and LR (r = −0.169, p < 0.001) were associated with a low concentration of sodium (Table 2). History of malignancy was also associated with a low sNa concentration in the ER group (Supplementary Table 2).
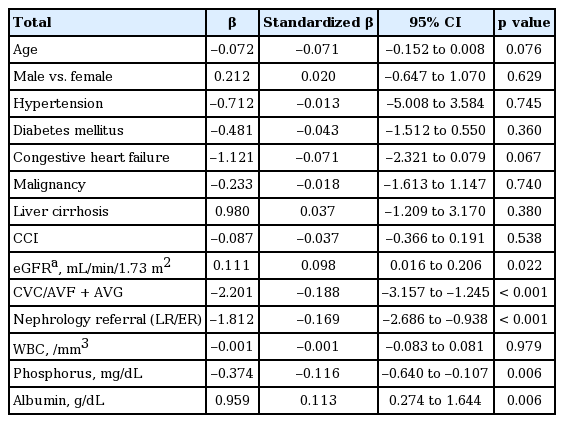
Factors associated with serum sodium using multivariable linear regression
Ninety-day and 1-year all-cause mortality
At the 90-day follow-up, 55 (28.8%) patients in the hyponatremia group, 51 patients (12.5%) in the normonatremia group had died. Considered as a continuous predictor, each 10-mmol/L increase in the sodium concentration tended to be associated with a lower all-cause mortality (HR = 0.746, p = 0.122). The risk of 90-day mortality was higher in the hyponatremia group than in the normonatremia group (HR = 1.547, p = 0.044) in total. After stratification by the timing of nephrology referral, a higher sNa concentration as a continuous variable reduced the mortality (HR = 0.423, p = 0.016), and hyponatremia as a categorical variable was associated with increased mortality in the ER group (HR = 2.335, p = 0.041). However, sNa concentration or hyponatremia was not associated with mortality in the LR group (Table 3 and Fig. 2). Besides hyponatremia, nonuse of renin-angiotensin aldosterone system blockade, high phosphorus, and low albumin were associated with a significantly increased risk of 90-day mortality in the ER group (p < 0.05). In the LR group, old age, higher score of CCI, and hypoalbuminemia were associated with increased risk 90-day mortality (p < 0.05) (Supplementary Table 3).
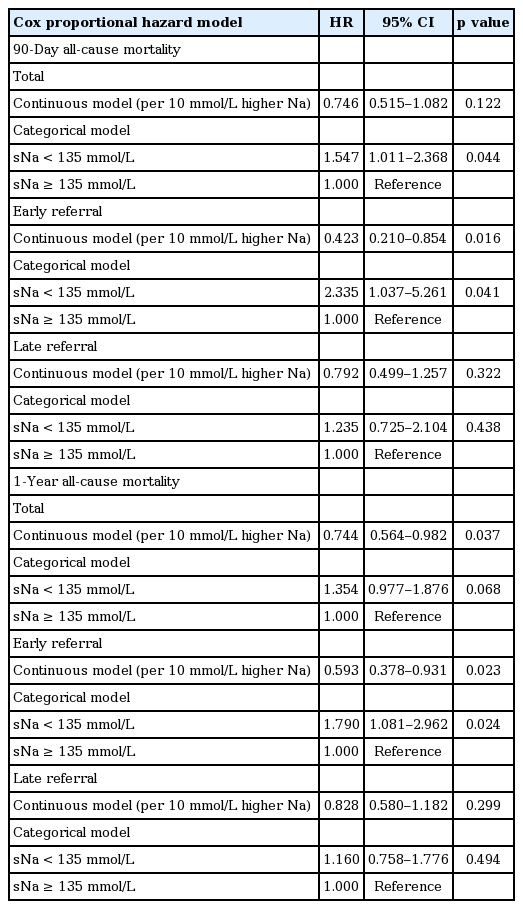
Ninety-day and 1-year all-cause mortality risk associated with predialysis serum sodium stratified by nephrology referral
The 1-year overall mortality rates for patients with ESRD were 44.0% (84 out of 191 patients) in the hyponatremia group, 22.1% (90 out of 408 patients) in the normonatremia group. A similar trend was observed when we analyzed the relationship between hyponatremia and 1-year mortality rate. The hyponatremia group also tended to showed increased 1-year mortality rate as compared to that of the normonatremia group in fully adjusted analysis (HR = 1.354, p = 0.068). After stratification by the timing of nephrology referral, higher sNa concentration as a continuous variable reduced mortality (HR = 0.593, p = 0.023), and hyponatremia as a categorical variable was associated with increased mortality in the ER group (HR = 1.790, p = 0.024). However, neither sodium concentration nor hyponatremia was associated with mortality in the LR group (Table 3 and Fig. 3). Besides hyponatremia, hypoalbuminemia, frequent use of CVC rather than AVF/AVG, and high phosphorus and were associated with significantly increased risk of 1-year mortality rate in the ER group (p < 0.05). In the LR group, old age, hypoalbuminemia, and frequent use of CVC rather than AVF/AVG were associated with increased risk of 1-year mortality (p < 0.05) (Supplementary Table 3).
DISCUSSION
In this study, among the 599 elderly patients for whom hemodialysis was initiated between 2000 and 2010, 31.8% presented with predialysis hyponatremia. We identified the factors associated with sNa concentration at dialysis initiation, and found that the timing of nephrology referral, in particular, was associated with sNa concentration. In addition, we found that predialysis hyponatremia increased the risk of short-term all-cause mortality in only the ER group.
In our study population, the proportion of elderly patients who experienced hyponatremia at dialysis initiation was 30.7%, similar to the proportion of patients receiving acute hospital care (28.2%) [2], and higher than the proportion of hospitalized elderly patients (18% to 24%) [24] or the proportion of adult outpatients receiving incident maintenance hemodialysis (12.8%) [8]. The possible explanation for the higher prevalence of hyponatremia in our study population is that our inclusion criterion was elderly (≥ 70 years) incident hemodialysis inpatients, who were at a high risk for hyponatremia. Because the definitions of the terms “elderly” and “hyponatremia” and the clinical setting vary widely among studies [3], we thought that direct comparisons of the prevalence of hyponatremia are difficult.
Our results pertaining to the factors associated with lower sNa concentrations, including lower albumin concentration, lower estimated GFR, and nonpreparation of AVF/AVG at hemodialysis initiation, were consistent with the results of the study by Nigwekar et al. [8]. In ArMORR (Incident hemodialysis patients from the Accelerated Mortality on Renal Replacement) study, hyponatremia was associated with hypercalcemia, elevated alkaline phosphatase, and hypoparathyroidism but not associated with phosphorous level [8]. However, in our study, hyperphosphatemia rather than hypercalcemia was significantly associated with hyponatremia among index of bone mineral metabolism. Although CHF is a risk factor for hyponatremia in general, CHF was not associated with sNa concentration in our population. We thought that there was a low prevalence of heart failure in our study to demonstrate the relevance of the association between CHF and hyponatremia. Also large scale cohort studies regarding hyponatremia in ESRD showed that CHF was not always associated with hyponatremia [8,9]. Furthermore, late nephrology referral showed a strong, significant association with hyponatremia even in a fully adjusted model. To our knowledge, ours is the first study to show that the timing of nephrology referral influences predialysis hyponatremia despite adjusting extensively for the possibility of confounders.
Overall, lower sNa concentration, as a continuous variable and hyponatremia, as a categorical variable tended to be associated with a higher risk of mortality in incident elderly hemodialysis patients. Although the mechanism(s) are not entirely clear, sNa concentration influences the 3-dimensional conformations of protein and enzyme and plays a critical role in cellular function. The relationship between abnormal sNa and cerebral dysfunction has been well described [10,25]. However, it remains uncertain whether hyponatremia is a bystander or a causative factor. While one meta-analysis showed that improvement in hyponatremia would revert the mortality risk related to hyponatremia [26], some other studies demonstrated that the resolution of hyponatremia did not reduce this risk [27-29]. We thought that hypona tremia might be used to predict for mortality. When the patient data were analyzed separately after stratification by the timing of nephrology referral, hyponatremia predicted mortality in only the ER group. No impact of hyponatremia or lower predialysis sNa concentration on mortality was observed in the LR group. We also re-conducted analysis, based on the patient’s with laboratory data immediately before dialysis (the ones with “0 to 1 day,” n = 440). We rigorously controlled for the influence of the available laboratory data on patients. A similar trend was observed when we analyzed the relationship between hyponatremia and 90-day/1-year mortality rate (90-day mortality: HR = 2.367, p = 0.037 in ER group, HR = 1.280, p = 0.384 in LR group; 1-year mortality: HR = 1.802, p = 0.040 in ER group, HR = 1.216, p = 0.401 in LR group). The possible explanations for the difference in the impact of hyponatremia on survival according to the timing of nephrology referral are as follows: first, in our data, although LR group experienced chronic inflammation and malnutrition more frequently (higher WBC and lower albumin concentration) compared to ER group, only ER group have statistically significant differences in WBC and albumin which were well-known to be predictors for mortality in incident hemodialysis patients between hyponatremia and normonatremia (Supplementary Table 1) [30,31]. Second, LR group experienced acute complications more frequently during the early period of dialysis, including infection and cardiovascular events, contributing to higher early-period mortality rate [18,32-36], although we could not confirm this possibility through our data because the cause of death was unavailable. In the present study, other factors including chronic or acute inflammation (i.e., frequent CVC use) or malnutrition (hypoalbuminemia) might have overshadowed hyponatremia as a predictor for 90-day and 1-year mortality in the LR group (Supplementary Table 3). We thought that referral-associated other acute complications, rather than hyponatremia, affected mortality in the LR group. We emphasize the originality of this study in that predialysis hyponatremia affected early-period mortality in the elderly incident hemodialysis patients, and in particular, nephrology referral associated hyponatremia affected the association between hyponatremia and mortality.
This study has several limitations. First, we used only a single sNa concentration for the analysis. Repeated measures of sNa concentration may reflect the true internal condition and yield more accurate results. Second, other confounding factors, including ultrafiltration volume, dialysate sodium concentration, residual renal function, and Kt/V cannot be excluded. However, data regarding dialysis prescription were unavailable. Previous studies have emphasized on vascular access, predialysis care, and nutritional status (hypoalbuminemia) rather than dialysis-associated factors as predictors of early-period mortality [34,36]. The dialysate sodium concentration is not typically adjusted for the predialysis sodium concentrations [10]. Third, although previous studies have clarified the effects of hyponatremia on cellular function or organ system [25,33], our retrospective study could not clearly explain the mechanism by which hyponatremia affects mortality.
In conclusion, predialysis hyponatremia at the initiation of maintenance hemodialysis is associated with the timing of nephrology referral and increased risk of mortality in the elderly. In particular, predialysis hyponatremia increased the risk of short-term all-cause mortality in only the ER group, and nephrology referral associated affected the association between hyponatremia and mortality in the elderly. Future prospective studies will be needed to determine whether an abnormal sNa concentration should be considered as an indication for treatment in clinical trials.
KEY MESSAGE
1. Predialysis hyponatremia at hemodialysis initiation is associated with the timing of nephrology referral and increased risk of short-term mortality in the elderly, particularly among early referral group.
2. Nephrology referral affects the association between hyponatremia and mortality in elderly patients.
Notes
No potential conflict of interest relevant to this article was reported.
Supplementary Materials
Baseline characteristics of patients according to serum sodium at the time of dialysis initiation stratified by nephrology referral
Factors associated with serum sodium using multivariable linear regression stratified by nephrology referral
Factors associated with 90-day and 1-year mortality using multivariable cox regression stratified by nephrology referral