Use of serology and polymerase chain reaction to detect atypical respiratory pathogens during acute exacerbation of chronic obstructive pulmonary disease
Article information
Abstract
Background/Aims
To use serological and multiplex polymerase chain reaction (PCR) assays to examine sputum samples from patients experiencing acute exacerbation of chronic obstructive pulmonary disease (AECOPD) for the presence of atypical pathogens, including Mycoplasma pneumoniae, Chlamydia pneumoniae, and Legionella pneumophila.
Methods
From September 2012 to February 2014, 341 patients with AECOPD attending outpatient clinics were enrolled as part of a randomized, double-blind, multicenter study. A commercial enzyme-linked immunosorbent assay was used to measure serum immunoglobulin M (IgM) and IgG antibody titers on the first day of the study and at 36 days post-enrollment. Multiplex PCR was used to test sputum samples for the presence of atypical pathogens. A urinary antigen test for L. pneumophila was performed on the first day.
Results
Nineteen patients (5.6%) showed serological evidence of acute infection with M. pneumoniae. Also, one and seven patients (2%) showed serological evidence of acute infection with C. pneumoniae and L. pneumophila, respectively. All DNA samples were negative for M. pneumoniae, C. pneumoniae, and L. pneumophila according to PCR. Only one urine sample was positive for L. pneumophila antigen, but serologic evidence was lacking.
Conclusions
Serological testing suggested that infection by atypical pathogens during AECOPD was relatively uncommon. In addition, PCR provided no direct evidence of infection by atypical pathogens. Thus, atypical pathogens may not be a major cause of AECOPD in South Korea.
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is associated with considerable morbidity and mortality. The World Health Organization estimates that COPD will be the third leading cause of death worldwide by 2030 [1]. The overall prevalence of COPD in subjects aged ≥ 40 years in Korea is estimated to be 13.4% [2]. Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) are the most important prognostic factor; such exacerbations are associated with short and long term reductions in quality of life and lung function, as well as an increased risk of death [3,4]. The etiology of AECOPD is multifactorial; the condition is caused by complex interactions between the host immune system, respiratory viruses, and airway bacteria, all of which lead to an increase in the inflammatory burden within the airway [5]. Previous data suggest that the etiology is unclear in nearly 30% of AECOPD cases; however, respiratory tract infection (50% to 60% of cases) and air pollution (10% of cases) are major causes [6].
Atypical respiratory pathogens usually include Mycoplasma pneumoniae, Chlamydia pneumoniae, and Legionella pneumophila, although the exact role of these pathogens in AECOPD is yet to be elucidated. Atypical pathogens are detected indirectly by serological assays, or directly by cell culture or polymerase chain reaction (PCR). Most studies used a single method [7-13], whereas a few combined methods [14-16]. Although serology may suggest that atypical pathogens play a significant role in AECOPD, interpreting serology results is tricky and yields variable results [7,8,17-25]. Also, culturing atypical pathogens is not easy. There are some data regarding the use of PCR for diagnosing atypical pathogens, and PCR appears superior to serology in this respect [26]. However, serology and PCR can yield discrepant results [14-16]. Indeed, a previous study revealed that, according to real-time PCR results, atypical pathogens do not play a significant role in stable COPD or AECOPD [9]. Thus, the role of atypical pathogens in AECOPD remains controversial. The present prospective study was designed to include patients with a moderate AECOPD (defined as an increase in symptoms that required treatment with antibiotics and/or corticosteroids, but not hospitalization); the aim was to use serology and multiplex PCR to determine the role of atypical pathogens in AECOPD.
METHODS
Study design and subjects
This was a post hoc analysis of a clinical trial examining the use of zabofloxacin versus moxifloxacin to treat patients with COPD exacerbation [27]. The study was a multicenter, randomized, double-blind, double-dummy, parallel-group, controlled, phase 3 clinical trial conducted at 31 university hospitals in South Korea. The first patient was enrolled in September 2012 and the last in February 2014.
Eligible patients were aged ≥ 40 years and had COPD as defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines (i.e., a post-bronchodilator forced expiratory volume in 1 second [FEV1]/forced vital capacity < 0.7). Patients experiencing moderate exacerbation of COPD (defined as worsening of respiratory symptoms beyond normal day-to-day variations and leading to a change in medication but not requiring hospitalization), and who also had purulent sputum or an increased volume of sputum, were enrolled. Pregnant women; patients who received systemic antibiotics and/or antifungal agents within the last 72 hours; those with confirmed pneumonia (on chest X-ray) within 48 hours; and those with underlying septic shock, bronchiectasis, lung abscess, active tuberculosis, pulmonary malignancy, cystic fibrosis, empyema, or asthma were excluded.
Microbiological assays
Each patient provided a sputum sample on day 1 (visit 1), day 10 ± 3 (visit 3), and day 36 ± 7 (visit 4). A blood sample was obtained on day 1 and day 36 ± 7. The sputum specimens containing group 4 or 5 in Gram stain score were used for bacterial culture and group 3 to 5 were considered suitable for PCR. Paired serum samples were used for serological tests for M. pneumoniae, C. pneumoniae, and L. pneumophila. Urine samples for the urinary antigen test were also collected on day 1 and examined for the presence of L. pneumophila and Streptococcus pneumoniae. All samples were sent to the central Seegene medical foundation reference laboratory (Seoul, Korea). Serological assays for M. pneumoniae were performed using the M. pneumoniae immunoglobulin G (IgG)/IgM enzyme-linked immunosorbent assay (ELISA) (Vircell, Granada, Spain). The assay for C. pneumoniae was performed using the SeroCP™ IgG/IgM kit (Savyon Diagnostics, Ashdod, Israel) and that for L. pneumophila was performed using the L. pneumophila serogroup 1 IgG/IgM ELISA (Vircell). All assays were performed according to the manufacturer’s protocols. A definite acute infection was defined as a 4-fold or greater increase of the IgG titer between the acute (day 1) and convalescent (day 36 ± 7) serum specimens. A probable acute infection was defined as a positive IgM result on day 1. Legionella antigen was detected in urine samples using the Binax NOW Legionella Urinary Antigen Test (Binax, Portland, ME, USA). Sputum samples were tested for atypical respiratory pathogens (M. pneumoniae, C. pneumoniae, and L. pneumophila) using a multiplex PCR assay (Seeplex PneumoBacter ACE Detection kit; Seegene), according to the manufacturer’s instructions. This multiplex PCR assay had a detection limit of 100 copies per reaction, and no cross-amplification of DNA from the 63 different pathogens was observed. The assay was also reproducible when PCR reactions were run on 5 different days. An acute atypical respiratory pathogenic infection was defined when serological tests, PCR, or the Legionella urinary antigen test was positive.
The study was approved by the Institutional Review Board of each hospital (2012-52), and all participants provided written informed consent. The study is registered with ClinicalTrials.gov (number NCT01658020) (Clinical Research Information Service http://ncrc.cdc.go.kr/cris;KCT0000532).
Statistical analysis
All statistical analyses were performed using SPSS for Windows version 21.0 (IBM Co., Armonk, NY, USA). Categorical variables were expressed as numbers and percentages, while numerical variables were expressed as the mean ± standard deviation. Differences between groups were compared using Student t test or the Mann-Whitney U test (continuous variables) or the chisquare test or Fisher exact test (categorical variables). Multiple logistic regression analysis was performed to identify independent factors that discriminate patients with atypical respiratory pathogens from those without. A p < 0.05 was considered statistically significant.
RESULTS
Demographic characteristics
In total, 428 COPD patients with moderate exacerbation of COPD were screened during the study period, and 345 met the inclusion criteria. Of these, 341 patients were included in this analysis; three patients were excluded because the drug was not administered and one patient was excluded because no serum samples were obtained for serology tests. The study group comprised 311 men and 30 women (mean age, 68.1 ± 7.9 years). Most patients (93.8%) had a smoking history and 88 (25.8%) were current smokers. The average post-bronchodilator FEV1 % predicted value was 49.7%, and the mean COPD assessment test (CAT) score at screening was 22.9. The baseline characteristics of the study subjects are shown in Table 1.

Baseline characteristics of the 341 patients with acute exacerbation of chronic obstructive pulmonary disease
Atypical respiratory pathogens
IgM and IgG antibodies specific for atypical respiratory pathogens were identified in 341 acute phase (day 1) and 327 convalescent phase (day 36 ± 7) serum samples. Of the 341 patients, 28 (8.2%) were positive for atypical respiratory pathogens; 10 of these patients also yielded at least one typical bacterial pathogen upon culture. By contrast, culture tests revealed that 119 patients (34.9%) were positive for typical respiratory pathogens.
Serological tests were positive for M. pneumoniae in 19 cases and one was positive for C. pneumoniae. Seven samples were positive for L. pneumophila in serological tests and one was positive in the urinary antigen test. However, PCR results for atypical respiratory pathogens were negative in all patients. The results of the serologic tests and PCR assays are shown in Table 2. Acute phase serum specimens from 16, 6, and 1 patient were positive for M. pneumoniae-, L. pneumophila-, and C. pneumoniae-specific IgM antibodies, respectively. Only four patients showed a 4-fold rise of the IgG titer between the acute and convalescent serum specimens. Of the 10 patients harboring typical bacterial pathogens, Haemophilus influenzae was isolated from five, Klebsiella pneumoniae from three, and S. pneumoniae from two. The serology and sputum culture results for the 28 patients are shown in Table 3.
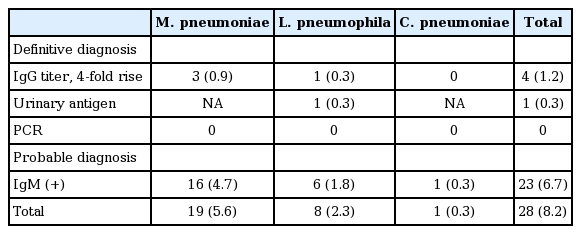
Prevalence of atypical pathogens in the 341 patients with acute exacerbation of chronic obstructive pulmonary disease
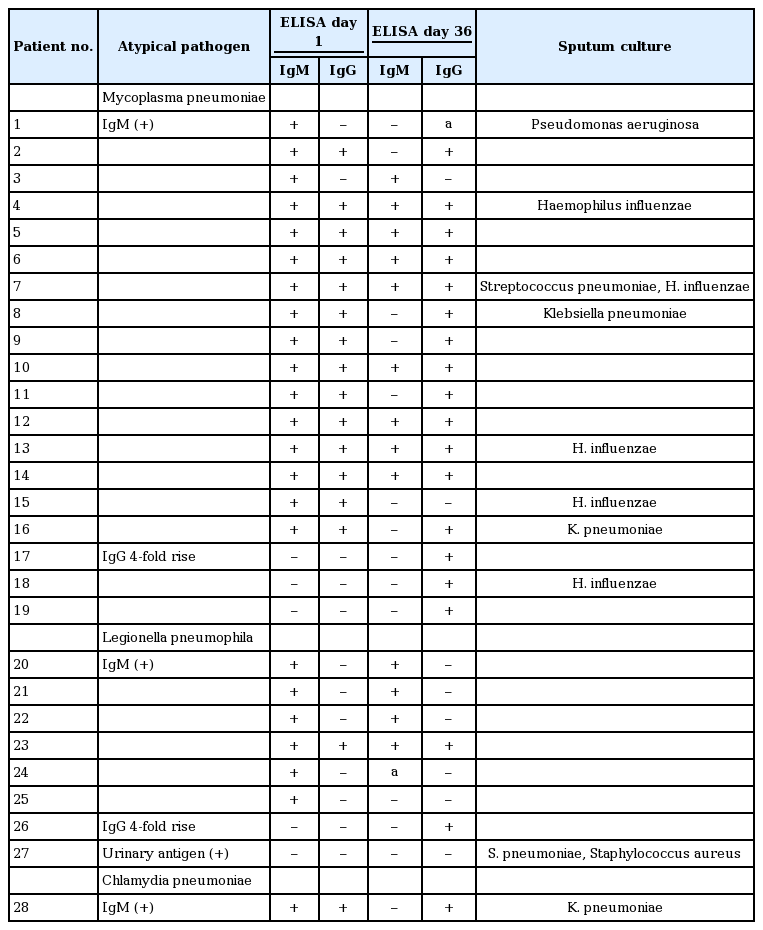
Serology and sputum culture results for 28 acute exacerbation of chronic obstructive pulmonary disease patients with a definite or probable diagnosis of infection by acute atypical respiratory pathogen
There was no significant difference between patients with and without atypical respiratory pathogens in terms of age, gender, smoking status, lung function, COPD stage, CAT score, severity of dyspnea, respiratory secretions, COPD phenotype, and clinical outcome. Only body mass index was significantly different between the two groups. However, none of the variables tested was identified as a significant independent factor by multiple logistic regression analysis (data not shown). Similar results were observed for patients with and without M. pneumoniae. There was no difference between patients with L. pneumophila and those without. Statistical analysis of data from groups with and without C. pneumoniae was not performed because only one patient had a positive result. The characteristics and outcomes of the patients with and without atypical respiratory pathogens are shown in Table 4.
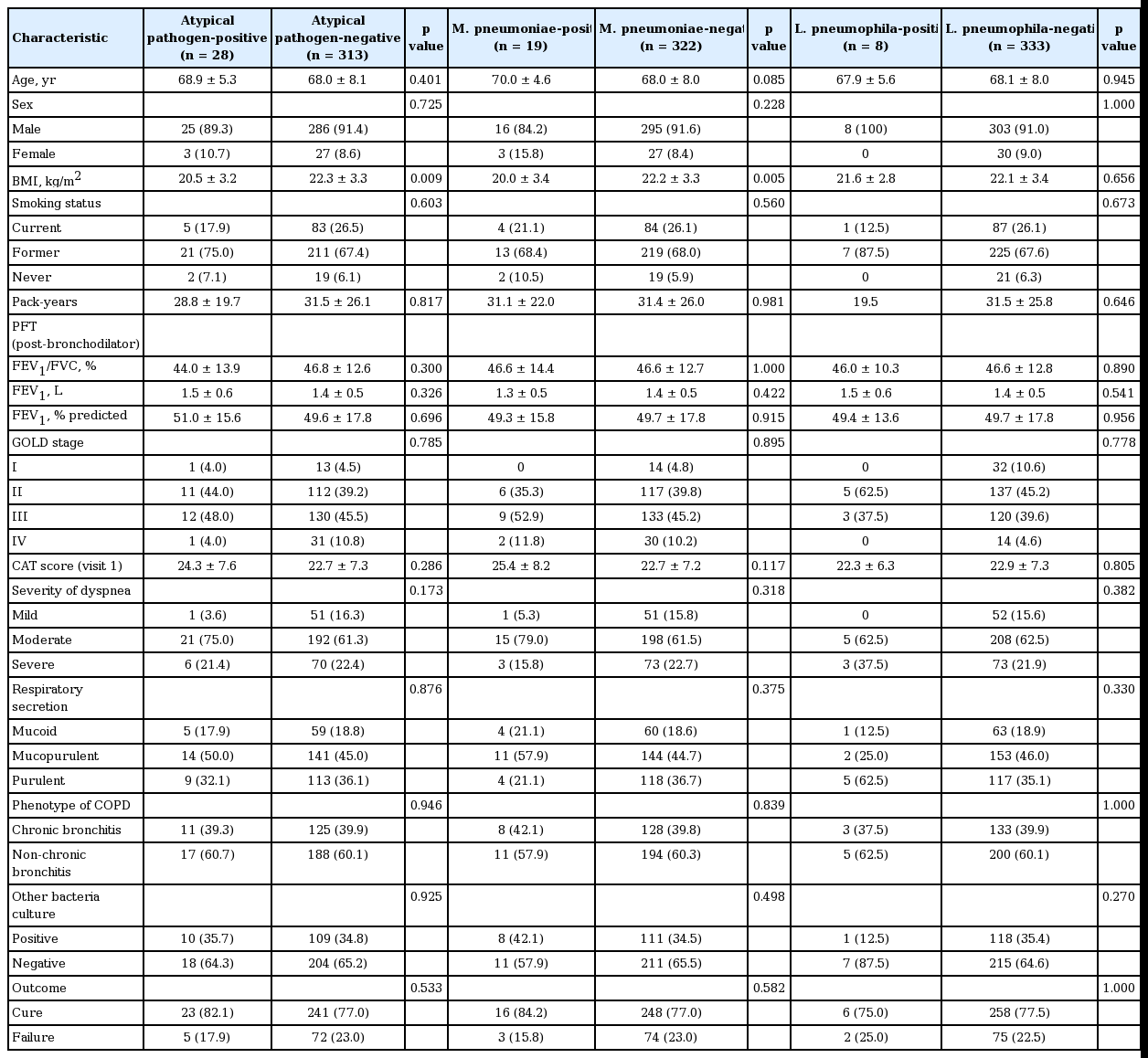
Characteristics and outcomes of patients with and without atypical respiratory pathogens
DISCUSSION
This study examined sputum samples from patients with AECOPD and used serological and multiplex PCR assays to assess the role of atypical pathogens. The serology results revealed that atypical pathogens were relatively uncommon in AECOPD. PCR revealed no direct evidence of atypical pathogens in AECOPD. Finally, we found no clinically significant differences between patients with and without atypical respiratory pathogens.
We enrolled patients with moderate AECOPD who attended outpatient clinics; however, most previous studies enrolled hospitalized patients with severe AECOPD [7,14,18,21,28,29]. Moderate AECOPD is defined as an increase in symptoms that requires treatment with antibiotics and/or corticosteroids, whereas a severe exacerbation is one that requires hospitalization [30]. Although our study was part of a multicenter trial, all laboratory tests were performed at a single central laboratory to avoid technical differences that may cause inconsistent results.
The role of atypical pathogens in AECOPD is controversial because M. pneumoniae and C. pneumoniae are common causes of respiratory tract infections, and both show high seroprevalence of IgG antibodies in the general healthy population (up to 60% and 70%, respectively) [31,32]. In the present study, the seroprevalence of IgG antibodies against M. pneumoniae, C. pneumonia, and L. pneumophila was 74.2%, 84.8%, and 2.6%, respectively. Also, there are different diagnostic criteria for detecting atypical pathogens by serology. A definitive diagnosis is based on a 4-fold increase in the IgG titer between the acute and convalescent phases; however, some studies report that the IgM response may be nonspecific or absent, particularly in adults [31,32]. One study defined elevated IgM levels on day 1 as a probable infection [15]. Another study defined an acute M. pneumoniae infection as a significant increase in the M. pneumoniae IgG titer, seroconversion in paired sera, or the presence of IgM antibodies against M. pneumoniae [26]. We defined a definite infection by atypical pathogens as a 4-fold or greater increase in the IgG titers and a probable infection as a positive IgM result on day 1.
Most previous studies used serologic techniques to detect atypical pathogens in AECOPD samples [7-13]. More recently, however, molecular techniques have been used to detect etiologic agents of AECOPD; indeed, several studies used PCR to detect atypical pathogens in AECOPD [9,14-16].
A previous study based on serologic assays reported a possible relationship between M. pneumoniae infection and AECOPD in 9% of hospitalized AECOPD cases [28]. Other reports estimate the prevalence of M. pneumoniae in AECOPD at between 0% to 16%, depending on the serologic method and diagnostic criteria used [7,11,15]. Recent microbiological studies of patients hospitalized for AECOPD identified M. pneumoniae in only 1.5% to 2.2% of cases using serologic methods [14,29]. Two previous studies of outpatient AECOPD did not detect M. pneumoniae infection by PCR [9,15]; however, serological evidence was obtained in 16% of cases [15]. Another prospective study attempted to detect M. pneumoniae in hospitalized AECOPD using both serologic and PCR-based methods. The serologic assay identified M. pneumoniae in two patients (2.2%) who were also PCR-positive; however, another 3/92 patients were PCR-positive alone [14]. A recent study prospectively examined 50 cases (43 cases of hospitalized AECOPD) using real-time PCR and conventional procedures, including sputum culture. PCR detected M. pneumoniae in four cases (8%) without any serologic evidence of infection [16]. Here, we found that none of the moderate AECOPD patients was PCR-positive, and that only 5.6% were positive for Mycoplasma infection according to serological tests.
According to serological tests, the incidence of C. pneumoniae among AECOPD is 4% to 16% [8,23-25]. Another recent study detected only one positive result for C. pneumoniae after serologic testing of 132 patients hospitalized for AECOPD [29]. Here, we identified only one patient with a C. pneumoniae infection by serology; this was the only patient that was IgM-positive at the initial visit. The PCR assay was negative. Indeed, another study found no PCR-based evidence of C. pneumoniae infection in outpatient AECOPD [9]. A recent prospective study diagnosed acute or presumed acute infection with C. pneumoniae in 4/92 hospitalized AECOPD patients (4.3%) by serologic testing; two of the four were also PCR-positive whereas one was positive by PCR only [14]. Another prospective study detected C. pneumonia in one patient by PCR, without any serologic evidence of infection [16].
Studies of the association between Legionella and AECOPD are relatively rare. A prospective study revealed serological evidence of Legionella spp. in 16.7% of hospitalized AECOPD patients [18]; however, another study detected Legionella non-pneumophila DNA in only one sputum sample out of 126 outpatient AECOPD samples by real-time PCR [9]. By contrast, another prospective AECOPD study did not detect Legionella spp. by PCR [14]. In the present study, we identified seven L. pneumophila-positive samples in serologic assays and one in the urinary antigen test; however, PCR was negative for all 341 patients.
Although PCR is used to detect atypical pathogens in clinical laboratories, no clear guidelines regarding the true performance, drawbacks, and limitations of the technique have been published [14]. PCR has been used to test for M. pneumoniae infections for about 20 years, but the method has several limitations. First, PCR inhibitors in samples can lead to false-negative results. Second, contamination can cause false-positive results. Third, the time of sampling influences the results. Indeed, in contrast to serologic assays, the diagnostic accuracy of PCR may decrease at or beyond 7 days after disease onset [26,33]. The above could explain why PCR shows low sensitivity for detecting atypical pathogens in AECOPD. Finally, samples suitable for PCR may be difficult to acquire.
A previous study showed that PCR was superior to serology for the diagnosis of acute M. pneumoniae infection and identified a high rate of persistent infection [9]. The study examined M. pneumoniae infection in children aged 10 to 16 years who showed acute respiratory symptoms during a community outbreak of Mycoplasma infection. The results revealed that PCR testing of respiratory secretions may provide an early diagnosis and be more sensitive than serologic techniques.
Another prospective study was conducted to compare the diagnostic value of an indirect immunofluorescence assay with that of PCR for the diagnosis of M. pneumoniae in adults. PCR showed lower sensitivity than serology; therefore, the authors recommended the use of serology and PCR in parallel to confirm M. pneumoniae infections in adults with community acquired pneumonia [34].
A meta-analysis showed that commercial PCR tests generate consistent results with high specificity, but they show low/variable sensitivity for M. pneumoniae. These findings suggest that, although commercial PCR tests may be superior for diagnosing M. pneumoniae infection, they cannot completely replace serologic assays. Thus, PCR plus serology could be a good screening method for the reliable and accurate diagnosis of M. pneumoniae infection [35].
Although a previous study showed that the seroprevalence of M. pneumoniae infection in a study population was significantly higher than that in the control group, the role (if any) played by M. pneumoniae in AECOPD was not substantiated by culture isolation or PCR [15]. Thus, there is a need for more studies of well-defined patient populations with AECOPD to establish a correlation between serological evidence of M. pneumoniae infection and that provided by culture and PCR.
Few studies have examined correlations between different microbiologic techniques with respect to the detection of atypical pathogens [14-16]. Indeed, we found no correlation between serologic assays and PCR in this respect.
Another finding that we found interesting was that 10 of 28 moderate AECOPD patients (36%) who were positive for atypical pathogens also yielded at least one typical bacterial pathogen upon sputum culture. A previous study detected at least one additional respiratory pathogen (viral or bacterial) in 71% of hospitalized AECOPD cases with M. pneumoniae [7]. Another prospective study of patients with severe exacerbation and respiratory failure showed that 29% were mixed infections by bacterial pathogens [11]. The prevalence of mixed infections varied, depending on the detection method and pathogen examined. One pathogen may exacerbate infection by another pathogen, or two pathogens may act independently.
The aim of the current prospective study was to use a combination of techniques (serologic assays and PCR) to determine the role of atypical pathogens in 341 AECOPD patients. This is a large cohort when compared with those in previous studies. However, a limitation of the present study is that we did not perform direct culture of atypical pathogens.
In conclusion, the serological prevalence of atypical pathogens in AECOPD was relatively low. These results, when combined with the negative PCR results, suggest that atypical pathogens play no (or a very limited) role in AECOPD, and that detection of atypical pathogens is not necessary in South Korea.
KEY MESSAGE
1. The serology results revealed that atypical pathogens were relatively uncommon in acute exacerbation of chronic obstructive pulmonary disease (AECOPD).
2. Polymerase chain reaction revealed no direct evidence of atypical pathogens in AECOPD.
3. Atypical pathogens may not be a major cause of AECOPD in South Korea.
Notes
This study was supported by Dongwha Pharmaceuticals, Seoul, Korea. The sponsors of all the funding bodies had no role in the design of the study, the collection and analysis of the data, or the preparation of the manuscript.
Acknowledgements
The participants of this study are as follows: Sung Hwan Jung, Jeong Woong Park, and Sun Young Kyung (Gachon University Gil Medical Center, Incheon, Korea), Joong Hyun Ahn, Ah Young Shin, Hwa Young Lee (College of Medicine, Incheon St. Mary's Hospital, The Catholic University of Korea, Incheon, Korea), Yoonki Hong (Kangwon National University Hospital, Chuncheon, Korea), Yi Young Jung (Gyeongsang National University School of Medicine, Jinju, Korea), Hee Joung Kim and Kwang Ha Yoo (Konkuk University School of Medicine, Seoul, Korea), Young June Jeon, Chi Young Jung (Keimyung University Dongsan Medical Center, Daegu, Korea), Kwang Ho In, Eun Joo Lee (Korea University Anam Hospital, Seoul, Korea), Sang-Do Lee, Sei Won Lee, Jae Seung Lee, and Yeon-Mok Oh (Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea), Lim, Gune-Il, Kim, Myung Shin (Soonchunhyang University Hospital Gumi, Gumi, Korea), Yong Hoon Kim, Jae Sung Choi, Ho Sung Lee (Soonchunhyang University Hospital Cheonan, Cheonan, Korea), Keu Sung Lee (Ajou University Hospital, Suwon, Korea), Kwang Won Seo, Yangjin Jegal, Jong-Joon Ahn (Ulsan University Hospital, Ulsan, Korea), Myoung Kyu Lee, Suk Joong Yong, Kye Chul Shin (Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea), Jin Hwa Lee, Yon Ju Ryu, Seok Jeong Lee, and Jung Hyun Chang (Ewha Womans University Medical Center, Seoul, Korea), Hang Jea Jang and Hyun Kuk Kim (Inje University Haeundae Paik Hospital, Busan, Korea), So Ri Kim, Seung Yong Park, Chi Ryang Chung (Chonbuk National University Hospital, Jeonju, Korea), Ju Ock Kim, Jeong Eun Lee (Chungnam National University Hospital, Daejeon, Korea), Ki Man Lee, Jin Young An (Chungbuk National University Hospital, Cheongju, Korea), Changhwan Kim, Jae Young Lee, Eun Kyung Mo (Hallym University Kangdong Sacred Heart Hospital, Seoul, Korea), Ki Suck Jung (Hallym University Sacred Heart Hospital, Anyang, Korea), Ji-Young Moon (Hanyang University Guri Hospital, Guri, Korea), Chin Kook Rhee (College of Medicine, Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea), Eu gene Choi (Daejeon Hankook Hospital, Daejeon, Korea), Yong-Soo Kwon (Chonnam National University Hospital, Gwangju, Korea), Ji-Hyun Lee (CHA Bundang Medical Center, CHA University, Seongnam, Korea), Myung Jae Park (Kyung Hee University Hospital, Seoul, Korea).
This work was supported by Soonchunhyang University Research fund.
We express our special thanks to Cheol Hee Lim and Sun Hea Lee in Dongwha Pharm Co. Ltd., Seoul, Korea.