Optimal body mass index for minimizing the risk for osteoporosis and type 2 diabetes
Article information
Abstract
Background/Aims
Body mass index (BMI) is positively associated with bone mineral density and type 2 diabetes. We investigated an optimal BMI range for osteoporosis and type 2 diabetes.
Methods
This cross-sectional study used data from the Korea National Health and Nutrition Examination Survey (KNHANES), 2008 to 2011. We included 3,774 men aged > 50 years and 4,982 postmenopausal women. Logistic regression models were applied to elucidate each BMI category’s osteoporosis and diabetes risks.
Results
The prevalence of osteoporosis was 9.0% for men and 40.8% for women. The prevalence of type 2 diabetes in men was 19.7% and in women was 15.5%. In men with BMI > 25 kg/m2, the osteoporosis risk did not further increase as BMI increased. In women, BMI was linearly associated with osteoporosis risk without a plateau. In both men and women, higher BMI was associated with a higher type 2 diabetes risk. Men with a BMI of 23.0 to 24.9 kg/m2 harbored about a 30% lower osteoporosis risk than and a similar diabetes risk to those with a BMI of 21.0 to 22.9 kg/m2. In women with a BMI of 23.0 to 24.9 kg/m2, the adjusted odds ratio for osteoporosis was 0.72 (95% confidence interval, 0.59 to 0.87); the diabetes risk was not higher than in those with a BMI of 21.0 to 22.9 kg/m2.
Conclusions
For Korean men aged > 50 years and postmenopausal women, a BMI of 23.0 to 24.9 kg/m2 was the optimal range for minimizing osteoporosis and type 2 diabetes risks simultaneously.
INTRODUCTION
Obesity is defined by excessive body fat accumulation and is a major cause of co-morbidities, such as type 2 diabetes and cardiovascular disease [1]. Weight loss remains the primary strategy for reducing the risks associated with obesity. However, several studies have shown a positive association between body mass index (BMI) and bone mineral density (BMD), and low body weight and substantial sudden weight loss induce bone loss [2]. Osteoporosis is characterized by reduced bone mass and disruption of bone architecture, resulting in increased risk of fractures. Osteoporotic fractures are associated with substantial pain and suffering, disability, and even death in affected patients and with substantial costs to the society [3]. Type 2 diabetes is associated with an increased prevalence of cardiovascular disease, causing significant morbidity and mortality [4-6]. In patients with diabetes, the risk of a wide range of vascular diseases is about twice that of patients without diabetes [7]. Therefore, it is important to minimize the risks of osteoporosis and type 2 diabetes, considering epidemics and economic consequences of the two diseases. Low body weight is a well-known risk factor for osteoporosis, but obesity is a significant risk factor for type 2 diabetes.
The World Health Organization (WHO) recommends the use of BMI ≥ 25 kg/m2 and BMI ≥ 30 kg/m2 for the definitions of overweight and obese, respectively [8]. These cut-off points are based on studies of associations between BMI and increased risk of type 2 diabetes and cardiovascular disease in Western populations. Therefore, it is uncertain whether the BMI cut-off values can be applied to populations of Asian ethnicity. The WHO/ International Association for the Study of Obesity/International Obesity Task Force have proposed BMI cut-off values of 23.0 to 24.9 kg/m2 for the classification of overweight and of ≥ 25.0 kg/m2 for obesity in Asians [9]. In these patients, inappropriate weight loss may increase the risk of osteoporosis.
Given that BMI is the target for weight control for health in underweight or overweight adults, we investigated the optimal BMI for minimizing the risk of both osteoporosis and type 2 diabetes in the Asian population.
METHODS
Subjects and study design
This study was based on data obtained from the Korea National Health and Nutrition Examination Survey (KNHANES) IV to V (2008 to 2011). The KNHANES was a nationwide cross-sectional survey conducted in 1998 to 2012 by the Korea Centers for Disease Control and Prevention. A stratified, multistage, clustered probability design was used to select a representative sample of non-institutionalized Korean civilians for the KNHANES, which is performed periodically to estimate the health and nutritional status of the Korean population. Subjects completed a questionnaire that comprised a health interview, health examination, and nutrition survey. Detailed information regarding data collection is available on the KNHANES website (https://knhanescdcgokr/knhanes/indexdo) [10]. A total of 19,315 subjects aged ≥ 19 years were examined between January 2008 and December 2011. Of these subjects, 9,740 were excluded because they were aged < 50 years or were premenopausal women. Menopause was defined by a self-questionnaire as the absence of menstruation for 12 consecutive months. Moreover, 660 subjects were excluded due to missing a whole-body, dual-energy, X-ray absorptiometry (DXA) scan, and 150 subjects were excluded due to missing anthropometric data or health questionnaire survey responses. As there are no variables in the KNHANES that identify the type of diabetes, subjects who were younger than 29 years at diagnosis were assumed to have type 1 diabetes based on a previous national study of the epidemiological characteristics of diabetes in Korea [11]. Finally, 3,774 men and 4,982 women were included in the study analysis (Supplementary Fig. 1).
Health behaviors and comorbidity
Current smokers were defined as those who had smoked 100 cigarettes in their lifetime and had smoked in the last 30 days. Alcohol consumption was indicated as “yes” if the subjects drank alcohol at least once a month in the past year. The level of physical activity was evaluated using the International Physical Activity Questionnaire by WHO. Subjects classified in the moderate- and/or vigorous-intensity physical activity category engaged in moderate-intensity physical activity for at least 30 minutes more than five times per week, or vigorous-intensity physical activity for at least 20 minutes more than three times per week [12]. Diabetes was defined as fasting blood glucose values ≥ 126 mmol/dL or hemoglobin A1c over 6.5%, self-reported diabetes medication use, or a previous diagnosis of diabetes by a physician based on the interview data. Fasting glucose and hemoglobin A1c were analyzed in a central certified laboratory. Hypertension was defined as systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg, or if the patients were currently receiving antihypertensive medication, or received a previous diagnosis of hypertension by a physician. Blood pressure was manually measured by well-trained nurses using mercury sphygmomanometers (Baumanometer; W.A. Baum, Copiague, NY, USA).
Measurements of anthropometric parameters and BMD
Height and body weight were measured using standard methods while the subjects were wearing light-weight clothes. BMI was calculated as the weight divided by height squared (kg/m2). BMI values were categorized as follows: < 18.5, 18.5 to 20.9, 21.0 to 22.9, 23.0 to 24.9, 25.0 to 29.9, and ≥ 30 kg/m2. BMD values for the lumbar spine (L1 to L4), total hip, and femur neck were measured using DXA (Discovery QDR 4500; Hologic Inc., Waltham, MA, USA). The coefficients of variation for measurements of the lumbar spine, total hip, and femur neck were 1.9, 1.8, and 1.5%, respectively. The prevalence of osteoporosis was defined by any BMD T score of less than –2.5 at the skeletal sites according to WHO recommendations [13]. The KNHANES data sets include whole-body DXA measurements of bone mineral content (g), total fat mass (g), and total lean mass (g).
Statistical analysis
We analyzed men and women separately. Baseline characteristics were compared across BMI categories using tests for trend associations. We used cubic splines to test nonlinearity in the associations between BMI, osteoporosis, and type 2 diabetes mellitus. Multivariate logistic regression models were used to study the odds ratios (ORs) of BMI categories for osteoporosis and type 2 diabetes mellitus adjusted for age, smoking habit, alcohol consumption habit, moderate- and/or vigorous-intensity physical activity, and history of malignancy. Normal BMI (21.0 to 22.9 kg/m2) was the reference group for all analyses. Statistical significance was defined as p < 0.05. Statistical analyses were performed with Statistica version 12.0 (StatSoft Inc., Tulsa, OK, USA).
Ethics statement
Written informed consent was obtained from all the subjects. KNHANES was conducted after the being given ethical approval by the Institutional Review Board of the Korea Center for Disease Control and Prevention (approval number: 2008-04EXP-01-C, 2009-01CON-03-2C, 2010-02CON-21-C, 2011-02CON-06C).
RESULTS
The clinical characteristics of the study subjects (men, n = 3,774; women, n = 4,982) are shown in Table 1. The mean ages of men and women were 63.6 ± 8.9 and 63.5 ± 9.7 years, respectively, and the mean BMIs were 23.6 ± 3.0 and 24.2 ± 3.2 kg/m2, respectively. The prevalence of osteoporosis was 9.0% in men and 40.8% in women, and 19.7% of men and 15.5% of women had type 2 diabetes mellitus (both p < 0.001)
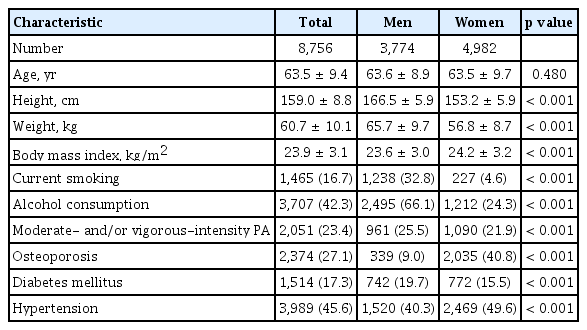
Clinical characteristics of Korean population in 2008 to 2011 Korea National Health and Nutrition Examination Survey
In men and women, 3.9% and 2.7% were underweight (BMI < 18.5 kg/m2), respectively, whereas 31.9% of men and 37.3% of women were obese with BMI > 25 kg/m2. Lower BMI categories were associated with older age, more common current smoking, and less prevalent type 2 diabetes and hypertension in both men and women. As the BMI increased, the prevalence of type 2 diabetes also increased: from 10.7% (BMI < 18.5 kg/m2) to 43.5% (BMI ≥ 30 kg/m2) in men and 7.4% (BMI < 18.5 kg/m2) to 30.0% (BMI ≥ 30 kg/m2) in women. There was an inverse relationship with osteoporosis: from 38.3% (BMI < 18.5 kg/m2) to 8.1% (BMI ≥ 30 kg/m2) in men and from 76.5% (BMI < 18.5 kg/m2) to 21.2% (BMI ≥ 30 kg/m2) in women (Tables 2 and 3, Fig. 1). As the BMI increased, the percentages fat mass increased but the percentages lean mass decreased in both men and women (both p < 0.001) (Fig. 2).
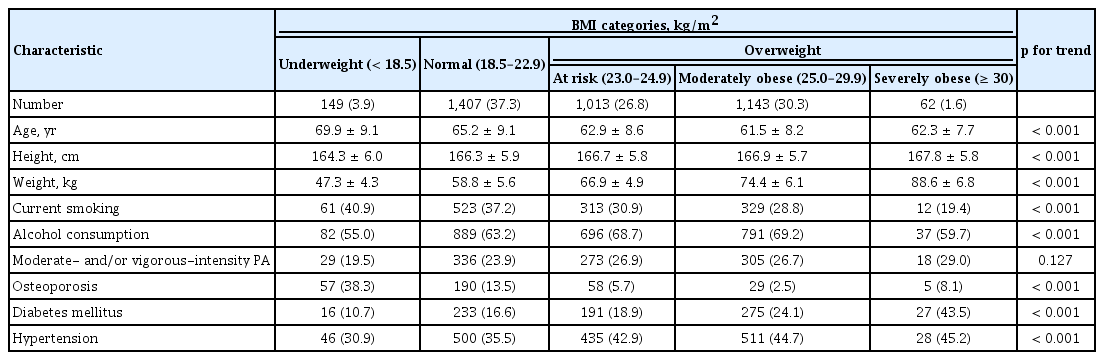
Clinical characteristics of men according to BMI category

Clinical characteristics of women according to BMI category
Prevalence of osteoporosis (A) and type 2 diabetes mellitus (B) in men and women. DM, diabetes mellitus; BMI, body mass index; BMD, bone mineral density.
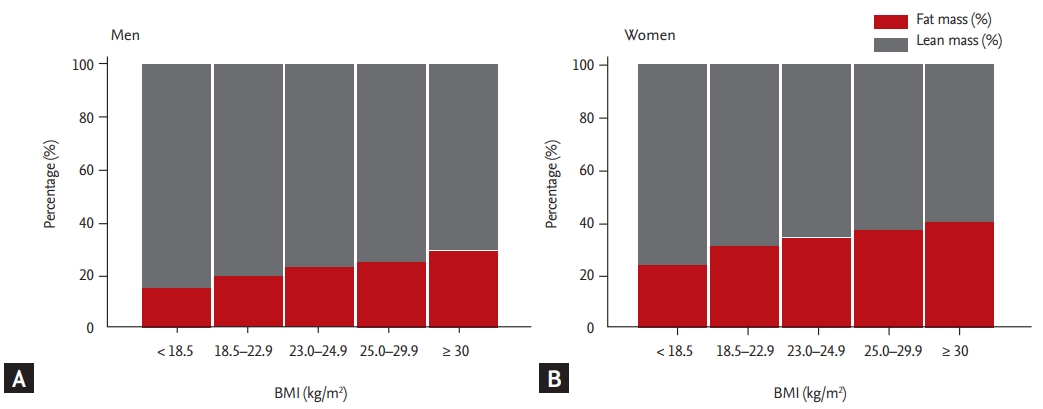
Percentages fat and lean mass according to body mass index (BMI) categories. (A) Men. (B) Women.
In men, the relationship between BMI and osteoporosis reached a plateau around a BMI of 25 kg/m2. However, increasing BMI was linearly associated with decreases in osteoporosis in women and was associated with increases in the prevalence of type 2 diabetes in both men and women (Fig. 3).
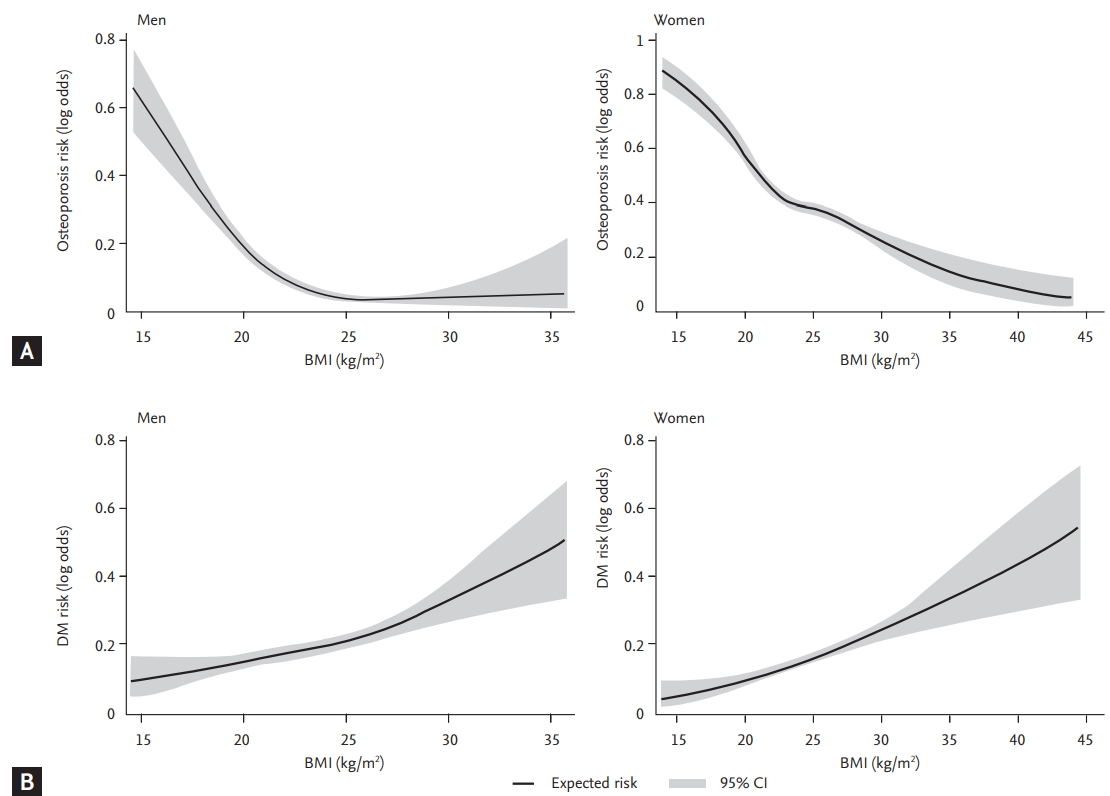
Association between body mass index (BMI) and (A) osteoporosis or (B) diabetes mellitus (DM) in men and women. CI, confidence interval.
We further used the logistic regression models of BMI categories for the risk of osteoporosis and type 2 diabetes after adjusting for age, smoking, alcohol consumption, moderate- and/or vigorous-intensity physical activities, and history of malignancy (Table 4 and 5). Men with a BMI of < 18.5 kg/m2 showed the highest risk for osteoporosis (OR, 4.95; 95% confidence interval [CI], 3.25 to 7.54) and the lowest risk for type 2 diabetes (OR, 0.48; 95% CI, 0.28 to 0.83). In men, compared with the reference range of BMI (21.0 to 22.9 kg/m2), a BMI of 23.0 to 24.9 kg/m2 was the highest BMI category for lowering osteoporosis risk without increasing type 2 diabetes risk. Women with a BMI < 18.5 kg/m2 showed the highest risk for osteoporosis (OR, 3.67; 95% CI, 2.23 to 6.05), but those with a BMI of < 18.5 kg/m2 carried the lowest risk for type 2 diabetes (OR, 0.44; 95% CI, 0.22 to 0.87). Similar to men, a BMI of 23.0 to 24.9 kg/m2 was the highest BMI category for lowering osteoporosis risk without increasing type 2 diabetes risk among BMI categories.
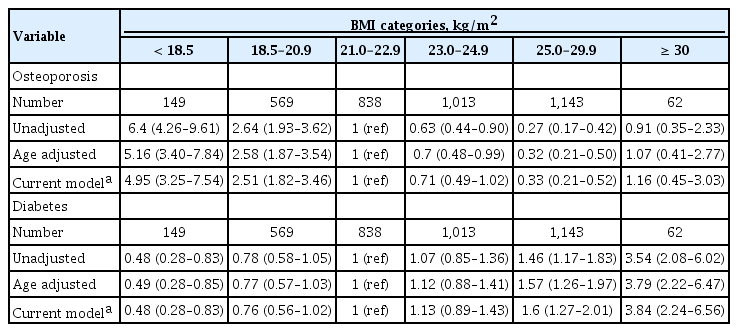
Logistic regression model of BMI categories for osteoporosis and diabetes in men after adjusting for covariates
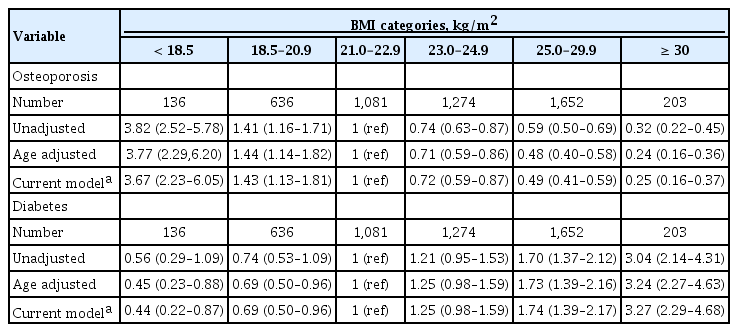
Logistic regression model of BMI categories for osteoporosis and diabetes in women after adjusting for covariates
DISCUSSION
In the nationwide study of Korean men above 50 years and postmenopausal women, we elucidated that a BMI of 23.0 to 24.9 kg/m2 was the optimal range for minimizing the risk of both osteoporosis and type 2 diabetes. The associations were maintained, even after adjustments for covariates, such as smoking, alcohol consumption, physical activities, and history of malignancy.
BMI is a strong and modifiable risk factor for both osteoporosis and type 2 diabetes. Being obese and overweight are strong protectors against bone loss. Ho et al. [14] reported that body weight was the best predictor of osteoporosis in postmenopausal Chinese women. A low BMI is associated with decreased BMD, and an increased risk of osteoporosis and osteoporotic fractures [2,15]. Compared with a BMI of 25 kg/m2, a BMI of < 20 kg/m2 had a risk ratio (RR) of about twice (RR, 1.95; 95% CI, 1.71 to 2.22) for hip fracture [16]. Optimal BMI levels for osteoporosis are not established, although Skrzek el al. [17] reported a BMI category of 26.0 to 27.9 kg/m2 for the lowest risk of osteoporosis in postmenopausal women. We demonstrated that a BMI of 25.0 to 29.9 kg/m2 in men and ≥ 30 kg/m2 in women conferred the lowest risk for osteoporosis. Compared with the reference group of BMI 21.0 to 22.9, the OR for osteoporosis was reduced by more than 60% in men with BMI of 25.0 to 29.9 and women with BMI of ≥ 30.
On the other hand, increasing BMI by 1 kg/m2 increased the risk of developing type 2 diabetes by 8.4% [18]. With this Korean data, an increase in BMI per 1 kg/m2 was related with the risk of type 2 diabetes by 10% in men and 12% in women. As the BMI increase by 1 kg/m2, the risk of osteoporosis in men and women decreases by 28% and 13%, respectively.
Approximately 80% of individuals with type 2 diabetes are overweight or obese (http://win.niddk.nih.gov/publications/PDFs/hlthrisks1104.pdf) [19]. In prediabetes, weight loss has been shown to delay the onset or reduce the risk of type 2 diabetes, while in type 2 diabetes, it has been shown to improve glycemic control [20-22]. In Asian populations, the proposed BMI cutoff values are between 23.0 to 27.5 kg/m2 for predicting the risk of type 2 diabetes, as well as cardiovascular disease and all-cause mortality [23-26]. Asian populations retain a relatively higher body fat percentage at a lower BMI than Western populations. Previous studies have shown that the risk of developing cardiovascular disease or type 2 diabetes is high at lower BMIs than that in Western populations [27]. Regarding the equivalent incidence of type 2 diabetes at a BMI of 30 kg/m2 in Western populations, the BMI cutoff value was 24 kg/m2 in South Asian, 25 kg/m2 in Chinese, and 26 kg/m2 in African populations [28]. We showed that the risk for type 2 diabetes began to increase at BMIs of 25 kg/m2 in men and women, which were the opposite for osteoporosis risk. Compared to men with a BMI of 21.0 to 22.9, men with a BMI of 25 to 29.9 had a 1.60-fold increase in type 2 diabetes risk and a 0.33-fold reduction in the risk of osteoporosis. Compared to women with a BMI of 21.0 to 22.9, women with a BMI of 25.0 to 29.9 increased the risk of type 2 diabetes by 1.74-fold and decreased the risk of osteoporosis by 0.49-fold.
According to a large prospective cohort study of Western populations, the BMI category associated with the lowest all-cause mortality was 22.5 kg/m2 or 20.0 to 25.0 kg/m2 [29,30], whereas other study has shown that the BMI category 25.0 to 29.9 kg/m2 confers a lower all-cause mortality rate than the normal weight (BMI 18.5 to 24.9 kg/m2) [31]. In Asian populations, Ng et al. [32] showed that the BMI exhibited a U-shaped association with allcause and cardiovascular mortality, with a nadir at BMI 23.0 to 24.9 kg/m2. In line with this, we also revealed that BMI of 23.0 to 24.9 kg/m2 was the optimal range for minimizing the risk of both osteoporosis and type 2 diabetes.
We also observed a sexual dimorphism between BMI and osteoporosis. Unlike women, further increases of BMI over 25 kg/m2 did not result in a beneficial effect on osteoporosis risk in men in this study. Pluijm et al. [33] also found that BMD is positively related to fat mass in 264 women, but not in 258 men. Discordant association between BMI and sexual hormones in men and women may partially explain our findings. Testosterone and sexual hormone binding globulin levels decreased in men with increased BMI, while a favorable association was shown between BMI and serum estrogen concentrations in postmenopausal women [34-36]. Karim et al. [35] suggested that these associations can be explained by the increased fat mass with increased peripheral aromatization after menopause. Another putative mechanism is increased plasma levels of leptin. A recent meta-analysis showed that high levels of leptin were positively associated with BMD in postmenopausal women [37].
Several caveats should be mentioned. The results of this study must be interpreted within the limits of a cross-sectional design focused on the association between BMI and comorbidities, and they were unable to explain causality. The study findings did not account for the BMI throughout childhood and young adult years of life which can be a critical determinant of osteoporosis. Also, BMI does not consider the relative proportions of fat and lean mass and cannot distinguish body fat distribution. However, higher BMI corresponded to a greater percentage fat mass and a lower percentage lean mass (Fig. 2). Because the percentage fat mass is strongly correlated with insulin resistance, a higher BMI contributes to the development of type 2 diabetes [38,39]. As BMI increases, the risk of hip fracture may decrease because of the mechanical loading effect of higher body weight, more muscle mass, and greater soft tissue padding over the hip [40]. However, fat mass has been inversely associated with BMD after adjustment for weight, suggesting that fat mass has a detrimental effect on bones [41]. Meyer et al. [42] reported that abdominal obesity was associated with an increased risk of hip fracture. Our baseline variables were collected from self-reported data. Because of the limitations of the data, we were unable to include information regarding the use of steroids. Self-reported diabetic medication use is used as a criterion to define diabetes in this study. This could potentially have overestimated the diagnosis of diabetes. However, the KNHANES is a nationwide, population-based survey of the Korean population, which provides an important basis for investigating the prevalence and associated factors of osteoporosis and type 2 diabetes in large data samples.
To our knowledge, this was the first study to demonstrate an appropriate BMI range for both osteoporosis and type 2 diabetes in Korean men and women. In conclusion, our findings show that a BMI of 23.0 to 24.9 kg/ m2 is an optimal range for minimizing the risk of both osteoporosis and type 2 diabetes in Korean men over 50 years of age and postmenopausal women. Further studies on gender differences in the association between BMI and osteoporosis are warranted. Prospective longitudinal studies are also needed to validate the optimal BMI to minimize the risk of developing osteoporosis and type 2 diabetes.
KEY MESSAGE
1. For Korean men aged > 50 years with body mass index (BMI) > 25 kg/m2, the osteoporosis risk did not further increase as BMI increased. For postmenopausal women, BMI was linearly associated with osteoporosis risk without a plateau.
2. For Korean men aged > 50 years and postmenopausal women, higher BMI was associated with a higher type 2 diabetes risk after covariate adjustments.
3. For Korean men aged > 50 years and postmenopausal women, a BMI of 23.0 to 24.9 kg/ m2, which was the classification of overweight according to the World Health Organization in Asians, was the optimal range for minimizing the risk of osteoporosis and type 2 diabetes simultaneously.
Supplementary Materials
Notes
No potential conflict of interest relevant to this article was reported.