Current status of heart failure: global and Korea
Article information

Abstract
Heart failure (HF) is a condition in which the heart is unable to pump enough blood to meet the body’s needs for blood and oxygen. Thus, HF is a grave disease with high morbidity and mortality. Because the prevalence of and exposure to the risk factors for HF increase with age, the prevalence of HF has been increasing in an aging society, including Korea. The vast advancement of medical and device therapy has improved the outcomes of HF, but significant residual risk still exists, and the benefit is confined to patients with reduced ejection fraction. Finding effective treatment for HF with preserved ejection fraction and identification of groups who benefit from drug and device therapy remain challenging. In this review, we illustrate the epidemiology, temporal trends, and current status of medical and device therapy, including heart transplantation, as well as emerging treatments for HF in Korea and worldwide.
INTRODUCTION
Heart failure (HF) is a condition in which the heart is unable to pump enough blood to meet the body’s needs for blood and oxygen [1]. It is a complex clinical syndrome characterized by definite symptoms (e.g., dyspnea or fatigue) and signs (e.g., increased jugular vein pressure, leg swelling, and pulmonary edema) caused by structural and/or functional abnormalities of the heart [2,3]. Hemodynamically, there is impairment of cardiac output and/or elevated intracardiac pressures at rest and during stress. It is important to note that HF is not synonymous with left ventricular dysfunction or cardiomyopathy alone; symptoms are necessary to diagnose HF.
EPIDEMIOLOGY
HF is a disease with high morbidity and mortality worldwide and in Korea. It affects more than 26 million people worldwide, and its prevalence is increasing [4]. The prevalence of HF varies between 0.1% and 6.7% worldwide.
Traditional risk factors for the development of HF include hypertension, diabetes mellitus, ischemic heart disease, and atrial fibrillation. Because the prevalence of and exposure to these risk factors increase with age, the prevalence of HF increases with the aging of the society. Indeed, in 1994, the prevalence of HF was 90 per 1,000 person-years and it increased to 121 per 1,000 person-years in 2003 among medicare beneficiaries 65 years or older in the United States [5]. Based on the National Health and Nutrition Examination Survey (NHANES) 2009 to 2012, an estimated 5.7 million adults had HF, whereas the NHANES 2013 to 2016 estimated that 6.2 million people ≥ 20 years of age had HF in the United States. Projection analysis estimates that, in 2030, more than 8 million people in the United States ≥ 18 years of age will have HF, which represents a 46% increase in prevalence from 2012 to 2030. The total percentage of the population with HF is predicted to increase from 2.42% in 2012 to 2.97% in 2030 [6]. HF is the leading cause of hospitalization and is associated with enormous healthcare costs. More than 1 million people are hospitalized for HF each year, and the 1-year readmission rate is greater than 25% in the USA [7]. The total cost for HF was estimated to be $30.7 billion in 2012 and is expected to increase by 127% to $69.8 billion in 2030 [8]. Two-thirds of these costs are directly attributable to medical costs.
With a decrease in the birth rate and an increase in life expectancy, Korea became an aged society in 2017, indicating that the elderly account for more than 14% of the total population. Consequently, the prevalence of HF is expected to rise owing to the change in population structure (Fig. 1A) [9]. In addition, the westernization of the Korean lifestyle and an increasing prevalence of ischemic heart disease also contribute to the rise in HF prevalence.
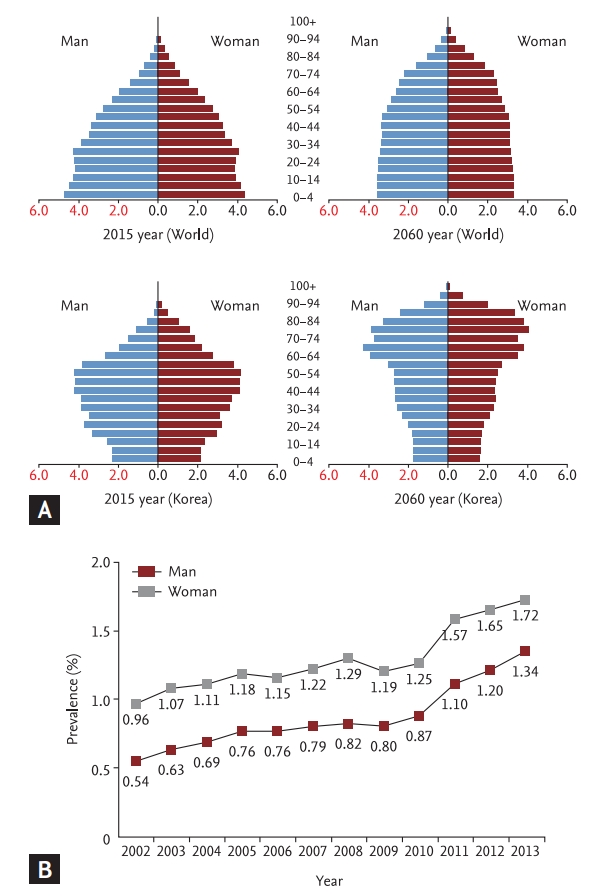
Population structure in 2015 and expected population structure in Korea in 2060. (A) Population structure of the world in 2015 (upper left panel) and expected structure in 2060 (upper right panel); population structure of Korea in 2015 (lower left panel), and expected population structure in 2060 (lower right panel). Adapted from Park et al. [9]. (B) Prevalence of heart failure according to sex in 2002 to 2013. Adapted from Lee et al. [10].
Using data from the 2002 to 2013 National Sample Cohort based on the National Health Information Database, the nationwide prevalence of HF in Korea was 0.75% in 2002 and 1.53% in 2012 (Fig. 1B). Interestingly, the projected HF prevalence is expected to be 1.89% and 3.35% in 2020 and 2040, respectively. By 2040, more than 1.7 million Koreans are expected to have HF [10].
The trend for increasing prevalence of HF is not a phenomenon confined to Korea but is observed worldwide in aging societies. Because the aging of the society appears to be inevitable, early and effective interventions to stop the progression of HF may be the only solution to prevent an HF epidemic [9].
DEFINITION OF HF
Left ventricular ejection fraction (LVEF) is an index of left ventricular contractility and is used to classify HF. The Korean Society of Heart Failure and the Heart Failure Association of the European Society of Cardiology define HF with normal LVEF (≥ 50%) as HF with preserved ejection fraction (HFpEF), HF with decreased LVEF (< 40%) as HF with reduced ejection fraction (HFrEF), and HF with LVEF ranging from 40% to 49% as HF with midrange ejection fraction (HFmrEF) [2,11]. By contrast, the American College of Cardiology Foundation/American Heart Association task force on practice guidelines categorize HF into HFrEF (LVEF < 40%) and HFpEF (LVEF ≥ 40%) groups only [3]. In the Korean Acute Heart Failure (KorAHF) registry, LVEF measurement was available in > 90% patients: 3,088 (60.5%) had LVEF that was 40% or less, while 1,285 (22.8%) had LVEF greater than 50% [12]. In the Korean Heart Failure (KorHF) registry, 743 (26.1%) patients had LVEF > 50% [13].
LVEF is not absolute, but it has relative value to volume status and is affected by heart rate in the acute setting. In addition, as the LVEF is not static, but changes during follow-up, some authors suggest reclassification of HF according to longitudinal LVEF changes. Patients with LVEF < 40% at baseline and > 40% at follow-up were defined as having HF with recovered ejection fraction (HFrecEF) or HF with improved ejection fraction (HFiEF) [14], whereas those with LVEF > 50% at baseline and < 40% at follow-up were defined as having HF with a declined ejection fraction (HFdEF) [15].
TEMPORAL TREND OF HF ACCORDING TO THE HF TYPE
Using 15-year follow-up data from Olmsted County, Minnesota, from 1987 to 2001, a similar trend of HF prevalence in the United States was illustrated. The proportion of patients with the diagnosis of HFpEF defined as LVEF > 50% increased over time, whereas that of HFrEF did not change significantly over time [16]. Regarding survival, the patients with HFpEF had a slightly higher survival rate. Among patients with HFrEF, the likelihood of survival increased during the study period, reflecting the improvement of therapy in HFrEF, whereas that of HFpEF did not change significantly reflecting the lack of effective treatment in HFpEF [16].
TEMPORAL TRENDS OF HF IN KOREA
In Korea there are four representative HF registries spanning almost 4 decades starting from 1987 until 2011: (1) between January 1987 and December 1997: the Hallym HF study including 1,657 patients from four hospitals in a retrospective registry [17]; (2) between January 1998 and August 2003: the Korean Multicenter HF study including 1,759 patients with acute heart failure (AHF) in a nationwide, prospective registry from nine university hospitals [18]; (3) between June 2004 and April 2009 the KorHF registry including 3,200 patients with AHF in a nationwide prospective registry from 24 academic hospitals [13]; and (4) between March 2011 and March 2014: the KorAHF registry including 5,625 patients with AHF in a nationwide prospective, multicenter registry from 10 hospitals [12]. These four registries help us to understand the temporal changes in HF in Korea (Table 1) [12,13,17-25]. In the last four decades, there was an increase in the mean age of the patients from 63.7 ± 13.4 years in 1987 to 69 ± 14 years in 2011. The prevalence of hypertension, diabetes mellitus, and atrial fibrillation also increased over time. The predominant etiology of HF was ischemic cardiomyopathy owing to the westernization of lifestyle and comorbidities among Koreans and improved survival of patients with coronary artery disease, including those presenting with acute myocardial infarction who eventually progress to cardiac dysfunction. This trend is also seen in Japan [26] and China [10]. In contrast, HF due to valvular heart disease has been decreasing, reflecting the decreasing prevalence of valvular heart disease in Korea.

Korean and international heart failure registries
During hospitalization for AHF, more parenteral drugs and extracorporeal membrane oxygenation or percutaneous cardiopulmonary support were applied, and more patients underwent heart transplantation, which led to a marked improvement in in-hospital mortality, while the costs increased by about 40% [12].
Regarding the post-discharge outcomes, the 1-year cumulative survival rate was 82%, 80.1%, 85%, and 81.8% for Hallym, Korea Multicenter, KorHF, and KorAHF, respectively. It is of note that direct comparison of the post-discharge outcomes is difficult because KorAHF validated survival using the National Insurance data or National Death Records mortality data, while the mortality was not validated in other registries, leaving the possibility of underestimation of the mortality rate. Taken together, the improvement in acute clinical care may have led to improved in-hospital outcomes, whereas long-term mortality remains unaffected.
MEDICAL THERAPY
Drugs targeting the sympathetic nervous system and neurohumoral activation have improved survival in patients with HFrEF [27]. To be more specific, angiotensin converting enzyme-inhibitors (ACEi), angiotenisn receptor blockers (ARBs), beta-blockers, mineralocorticoid receptor antagnoists (MRA), ivabradine, and recently sacubitril/valsartan were able to improve the clinical outcomes in patients with HFrEF [28-35]. In contrast, none of these drugs were able to improve survival in patients with HFpEF [36-39].
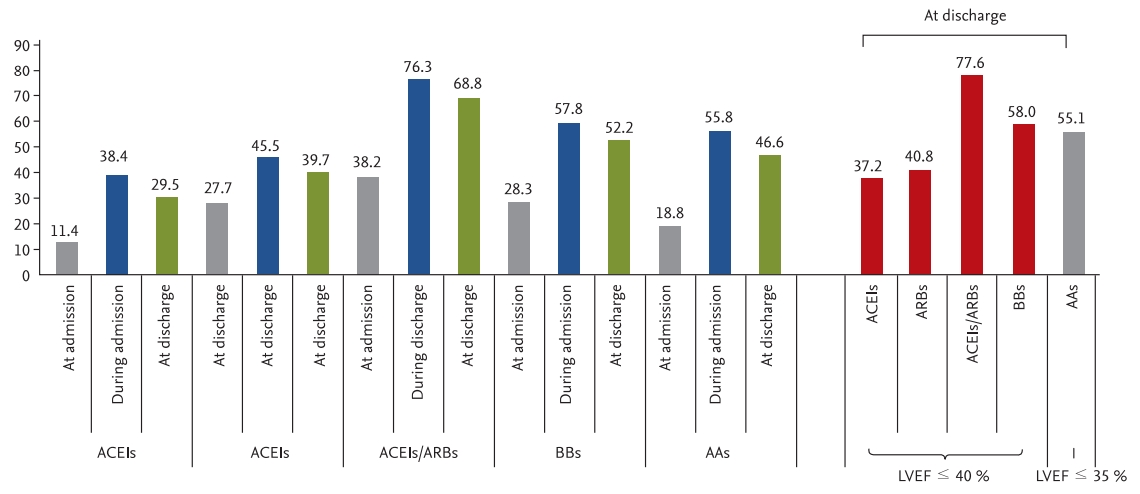
The KorAHF-Registry provides an important insight into drug prescription patterns during AHF admission. The prescription rate of the drugs was generally low at admission, which may be explained by the fact that 52% of the patients had de novo (new-onset) HF and were possibly drug naïve. The prescription rates reached a peak during hospitalization but declined by discharge, inferring that physicians attempt to initiate guideline-directed medical therapy but must discontinue some drugs due to intolerability. At discharge from AHF admission, 68.8%, 52.2%, and 46.6% of patients were on renin-angiotensin-system inhibitors (RAS inhibitors, ACEi, or ARB), beta-blockers, or MRAs, respectively (Fig. 2). When stratifying the patients according to the indications of each drug, that is, RAS inhibitors and beta-blockers in patients with LVEF ≤ 40% and MRAs in patients with LVEF ≤ 35%, 77.6%, 58.0%, and 55.1% of the patients were treated with RAS inhibitors, beta-blockers, or MRAs at discharge, respectively.
Many patients with HFrEF experience improvement or recovery of LVEF. In the KorAHF registry, 2,302 (75%) patients with HFrEF had baseline and follow-up echocardiography at 12 months. HF phenotypes were defined as persistent HFrEF (LVEF ≤ 40% at baseline and at the 1-year follow-up) or HFiEF (LVEF ≤ 40% at baseline and improved to > 40% at 1-year follow-up), and those with HFiEF had a lower mortality rate compared to patients with persistent HFrEF [14]. Regarding medical treatment, beta-blockers, but not RAS inhibitors or MRAs, were associated with a reduced all-cause mortality risk. The benefits seemed similar in patients receiving low- or high-dose beta-blockers. The study implies that although HFiEF is a distinct HF phenotype with better clinical outcomes than those of other phenotypes, beta-blockers should be continued in these patients [28].
Despite progress in HF therapies and improvement of the prognosis, there is still a substantial residual risk for death, stimulating the search for new therapeutic options. Diabetes is an important risk factor for HF. Although an increase in hemoglobin A1c is associated with an increased risk of HF, intensive glycemic control does not reduce the incidence of HF [40,41].
Because of the potential risk of adverse cardiovascular outcomes of antidiabetic drugs, they are required to undergo cardiovascular outcome trials to prove their safety. Sodium-glucose transporter 2 (SGLT2) inhibitors are a new class of oral antidiabetic drugs. In cardiovascular outcome trials (Table 2), empagliflozin [42], canagliflozin [43], and dapagliflozin [44] showed a robust reduction in hospitalization for HF in patients with type 2 diabetes mellitus with and without established atherosclerotic cardiovascular disease (ASCVD) [45]. This benefit was observed in a broad population regardless of prior HF, established ASCVD, ejection fraction, or kidney function [46].
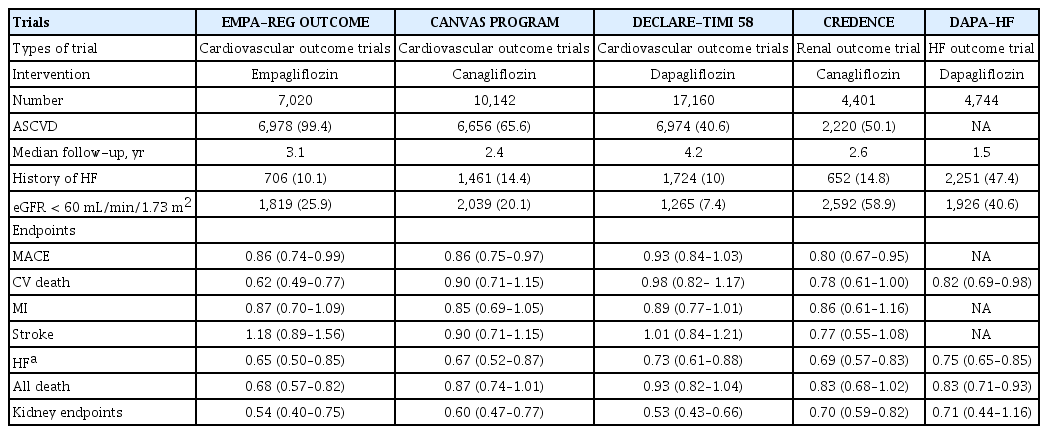
Summary of sodium-glucose transporter 2 inhibitor trials
The Study to Evaluate the Effect of Dapagliflozin on the Incidence of Worsening Heart Failure or Cardiovascular Death in Patients With Chronic Heart Failure With Reduced Ejection Fraction (DAPA-HF) trial [47] investigated the effect of dapagliflozin in patients with HFrEF with and without diabetes who received optimal medical treatment including beta-blockers, RAS inhibitors, sacubitril/valsartan, and MRAs. Dapagliflozin reduced the composite of CV death, hospitalization for HF, and urgent HF visits by 26%. Thus, SGLT2 inhibitors seem to be emerging drugs for patients with HFrEF.
In the withdrawal of pharmacological treatment for HF in patients with recovered dilated cardiomyopathy (TRED-HF) study, 51 patients with previous dilated cardiomyopathy whose LVEF had improved from < 40% to ≥ 50%, whose left ventricular end-diastolic volume (LVEDV) had normalized, and who had an N-terminal pro-B-type natriuretic peptide concentration < 250 ng/L were randomly assigned to phased withdrawal or continuation of treatment [48]. Over the first 6 months, 44% of the patients randomly assigned to treatment withdrawal experienced a relapse compared with none of those assigned to continue treatment. The study implies that many patients who recover from dilated cardiomyopathy will relapse following treatment withdrawal and suggests continuing treatment indefinitely.
On the contrary, some patients with HFpEF experienced a decline in LVEF during follow-up. Of the patients with HFpEF in the KorAHF registry, 426 (90.4%) were diagnosed as having persistent HFpEF and 45 (9.6%) as having HFdEF defined as LVEF ≥ 50% at admission and < 50% at 1 year [15]. Patients with HFdEF had a worse prognosis, and the use of beta-blockers, RAS inhibitors, and MRAs was not associated with improved prognosis of patients with HFdEF.
DEVICE THERAPY AND HEART TRANSPLANTATION
The current guidelines recommend an implantable cardioverter defibrillator (ICD) for primary prevention in symptomatic HF patients with LVEF ≤ 35% despite > 3 months of optimal medical therapy [2,11]. Cardiac resynchronization therapy (CRT) is indicated in symptomatic patients with LVEF ≤ 35% despite optimal medical therapy who have a left bundle branch block and a QRS duration ≥ 130 ms [2,11]. There has been an underutilization of ICD and CRT in Korea. In the United States, the ICD implantation rate was 46.2 cases per 100,000 persons in 2006 [49], whereas in Western Europe, the CRT device implantation rate was 19.7 per 100,000 persons in 2014 [50]. Furthermore, the ICD implantation rate in Japan was seven times (0.6 vs. 4.2 in 2009) higher than that of Korea from 2009 to 2010 [51]. However, with reimbursement for the device and increasing awareness and education of HF patients and physicians, there was has been a steady increase in device therapy in patients with HF (Fig. 3A) [52].
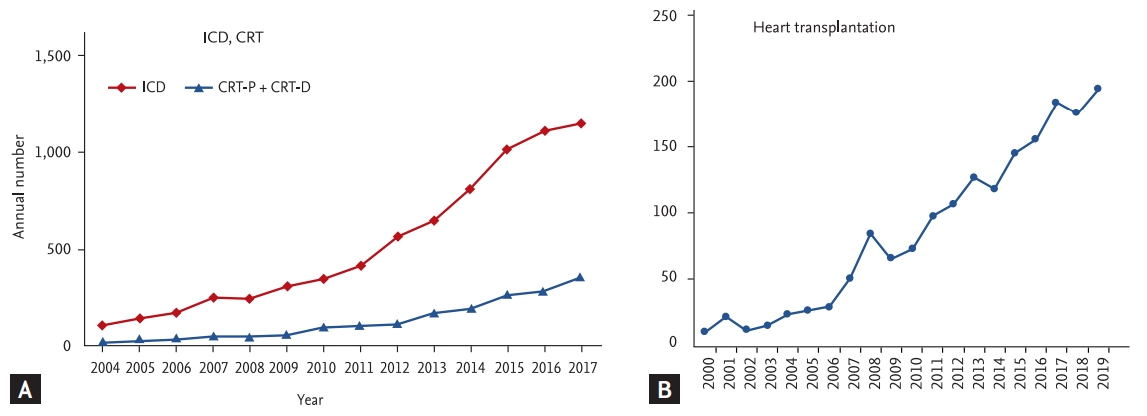
Temporal trends of device therapy and heart transplantation. (A) Cardiac implantable electronic device implantation in Korea. (B) Heart transplantation. Adapted from Choi et al. [52]. ICD, implantable cardioverter-defibrillator; CRT-P, cardiac resynchronization therapy without defibrillator; CRT-D, cardiac resynchronization therapy with defibrillator.
Because of the improvements in the treatment of HF, an increasing number of patients are living with advanced-stage HF [53]. Heart transplantation is a valid treatment option for patients with end-stage HF who are deemed to be appropriate candidates. Improvements in immunosuppressants, donor procurement, surgical techniques, and post-transplant care have resulted in a substantial decrease in allograft rejection and increased survival, exercise capacity, and quality of life [54,55]. In Korea, the first heart transplantation was performed in 1992, and by the end of 2019, over 1700 patients had undergone heart transplantation (Fig. 3B). Because the number of patients with end-stage HF who are eligible for heart transplantation is increasing, there is a significant organ shortage and a long waiting time. The disparity between available donor hearts and cardiac transplant candidates led to the development of mechanical circulatory support (MCS) devices, and durable and implantable MCS devices are used as a bridge to cardiac transplantation. Since 2019, left ventricular assist devices have been reimbursed by the Korean National Health Insurance and have been actively used as a bridge to cardiac transplantation in patients requiring MCS in Korea.
HEART FAILURE WITH PRESERVED EJECTION FRACTION
Although patients with HFpEF have normal or preserved LVEF, they have a prognosis similar to HFrEF. HFpEF is challenging because the underlying pathophysiology is poorly understood; therefore, there are controversies regarding the diagnostic criteria, and its diagnosis can be difficult even for HF specialists [56]. More importantly, until now, no therapy has been shown to improve the outcomes in these patients.
In the Japanese Diastolic Heart Failure (J-DHF) study with 245 patients with LVEF > 40%, carvedilol did not improve the prognosis of patients with HFpEF [37]. In an individual patient-level meta-analysis of 11 trials, Cleland et al. [57] also demonstrated that administration of beta-blockers did not improve outcomes in patients with HFpEF defined as an LVEF of ≥ 50%. Regarding RAS inhibitors, perindopril [58], irbesartan [36], candesartan [59], and spironolactone [38] showed neutral results in terms of survival gain. Similarly, sacubitril/valsartan, an angiotensin-receptor-neprilysin inhibitor, failed to improve survival in patients with HFpEF [39]. Thus, it is of clinical interest and importance to determine whether SGLT2 inhibitors can improve the outcomes in patients with HFpEF and change the practice guidelines.
CONCLUSIONS
HF is a disease with high morbidity and mortality. With an aging society, its prevalence is expected to grow in Korea and worldwide. Although there have been enormous advancements in treatment that have significantly improved the outcomes of HF, significant residual risk exists, and the benefit has been confined to HFrEF. Finding effective treatment for HFpEF and identifying groups of patients who would benefit from drug and device therapy remains a challenge.
Notes
No potential conflict of interest relevant to this article was reported.