Factors associated with anticholinergic burden among older patients in long-term care hospitals in Korea
Article information
Abstract
Background/Aims
Drugs with anticholinergic properties (DAPs) are associated with adverse health outcomes in older patients. The objective of this study was to evaluate the factors that determine the prescribing of more DAPs in long-term care hospitals (LTCHs) in Korea. In addition, the current patterns of DAP prescription were explored using a novel platform, which can collect data from LTCHs.
Methods
This was a Health-RESPECT (integrated caRE Systems for elderly PatiEnts using iCT) sub-study, which is a pragmatic, cluster-randomized, controlled trial. The Health-RESPECT platform was used to collect prescribed medication data of 466 patients (aged ≥ 65 years) from seven LTCHs. DAPs were identified using the Korean Anticholinergic Burden Scale (KABS). Physical frailty, cognitive function, functional status, and quality of life were evaluated.
Results
Among 466 LTCH patients, 88.8% (n = 414) were prescribed DAPs, and the prevalence of high KABS (≥ 3) was 70.4% (n = 328). The drugs that contributed most to the total KABS were quetiapine (20.7%), chlorpheniramine (19.5%), tramadol (9.8%), cimetidine (5.8%), and furosemide (3.6%). Polypharmacy, higher body mass index, less dependence, better communication and cognitive functions, and poorer quality of life were associated with high KABS.
Conclusions
Although the patients with a high burden of DAPs were less dependent and had better cognitive and communication functions, they had poorer quality of life. DAP use in LTCH patients should be monitored carefully, and the risk/benefit relationship for their use should be considered.

INTRODUCTION
In Korea, the proportion of older adults, defined as those aged 65 or older, has doubled in only 17 years from 7% (an aging society) in 2000 to 14% (an aged society) in 2017 and is expected to grow to 21% (a super-aged society society) by 2026 [1]. Consequently, the prevalence of chronic diseases, non-specific symptoms caused by ageing, and functional impairment is expected to increase. Accordingly, the number of older people who require the services of a long-term care hospital (LTCH) in Korea has increased drastically due to the growth of the population in need of medical services for chronic multi-morbidity and personal care [2,3]. Frail older patients are hospitalized at LTCHs in Korea for extended durations because of the decrease in family support for older parents and easy access to inpatient care financed by the National Health Insurance Program [4].
Given the comorbidities in older adults, polypharmacy is common, thus raising the risk of using potentially inappropriate medications (PIMs), defined as medications with more risks than benefits. Polypharmacy and PIMs are growing concerns for older patients because of increased healthcare costs, adverse drug events, drug interactions, medication non-adherence, functional decline, and multiple geriatric syndromes [5,6]. Most drugs with anticholinergic properties (DAPs) are classified as PIMs, and their use in older patients is discouraged. DAPs are associated with dry mouth, dry eye, constipation, dizziness, falls, cognitive decline, and physical impairment [7–9]. Older patients with multi-morbidities, who are independent or frail, tend to complain of symptoms related to diseases or geriatric syndromes and are more likely to experience polypharmacy or take PIMs due to the prescribing cascade, resulting in adverse drug events [10–12]. Since the clinical and demographic characteristics of hospitalized patients at LTCHs are expected to differ from those of community-dwelling older patients, DAPs are likely to be prescribed more frequently for the older patients living in LTCHs. However, no study has identified the clinical characteristics of patients with a high DAP burden or the prescription pattern of DAPs in LTCHs in Korea.
The anticholinergic drug burden of an individual is defined by the cumulative effect of taking one or more DAPs. Several anticholinergic drug burden indices have been validated, and a higher anticholinergic drug index strongly correlates with poor cognitive and functional outcomes [13]. Due to differences in prescribing patterns and medication availability across countries, country-specific anticholinergic burden scales have been developed. In Korea, the Korean Anticholinergic Burden Scale (KABS) was developed and validated based on literature evaluation and a modified Delphi process [14,15]. KABS was validated in a claim-based case-control study on the dose-response relationship between KABS burden and incident dementia [15].
We aimed to investigate the clinical and demographic factors associated with the prescribing of more DAPs according to the KABS data in older patients. In addition, we explored the prevalence of DAPs and DAP burden, current status of polypharmacy, and patterns of DAP prescription in LTCH residents in Korea.
METHODS
Study population
Data from participants of the Health-RESPECT (integrated caRE Systems for elderly PatiEnts using iCT) study, a cluster-randomized controlled trial conducted in long-term care institutions, were analysed. The study was conducted in seven LTCHs and five nursing homes in Korea. The study involved cluster randomization, after which patients who provided informed consent were recruited. During the study period, after the initial assessment, the intervention group underwent a 3-month intervention, while the observation group underwent a 3-month observation period with no intervention. A specific time point (initial assessment) was defined as the date when the intervention was started in the intervention group and was defined as the date of assessment visit in the observation group. Patients aged 65 years or older with chronic diseases and who had stayed in the facility for at least 2 weeks before enrolment were included in this study. However, patients that were comatose, expected to expire, or to be discharged within 3 months were excluded. Specific inclusion and exclusion criteria and services provided were described previously [16,17]. We analysed the data of patients recruited from LTCHs only to maintain the homogeneity of the accuracy of the data because nursing homes do not use electronic medication record systems, and the prescriptions were received from multiple medical institutions. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Patients or legal guardians provided written informed consent.
Health-RESPECT platform and data acquisition
The Health-RESPECT platform provides comprehensive geriatric assessment, individualized care plans for chronic diseases, medication and rehabilitation management through the service platform, periodic videoconference, and in-system assessment. The Health-RESPECT platform evaluates adverse events and generates warning alarms that are delivered via message to the attending physician of the LTCH. Data including patients’ vital signs, laboratory findings, and prescribed medication were retrieved from the electronic medication records of the LTCH via a health information exchange network system, which was previously developed and used for the patient referral service between institutions [18]. Medication prescription data were extracted from the Health-RESPECT platform.
Measurements
A trained nurse conducted an independent assessment of frailty status, demographic data, cognitive function, functional ambulatory capacity, overall functional status, and quality of life. Frailty status was evaluated using the Korean version of the FRAIL (K-FRAIL) scale. Scores of ≥ 3, 1 to 2, and 0 were classified as frail, pre-frail, and robust, respectively [19]. Functional status of older participants was measured using an interRAI long-term care facilities (LTCF) tool and comprehensive geriatric assessment [20]. From the items in the interRAI LTCF tool, several functional scales can be generated, including activities of daily living (ADL), cognition, depression, communication, and pain [21]. The ADL hierarchy (ADLH) scale is a seven-level tool of functional performance based on four items: personal hygiene, locomotion, toilet use, and eating [22]. Using an algorithm, severity patterns of the variables categorized people from 0 (independent) to 6 (total dependence). The depression rating scale measured the mood of an individual, and its score ranges from 0 to 14 [23]. The communication (COMM) scale encompasses two four-point items: self-understanding and the ability to understand others [24]. The COMM scale ranges from 0 to 8, with higher scores reflecting poorer communication. The pain scale quantifies pain frequency and intensity; a higher pain score indicates more severe pain (ranges from 0 to 3) [25]. EuroQol-5 Dimension (EQ-5D), the Korean version of the Mini-Mental State Examination (MMSE), and functional ambulatory category were used to evaluate the quality of life, cognitive function, and functional ambulatory category, respectively [26,27].
The data collected at initial assessment, which was initially surveyed by the assessment team or medical records collected from the Health-RESPECT platform, were analysed. The copies of written informed consent and study protocol were reviewed and approved by the Seoul National University Bundang Hospital Institutional Review Board (IRB number: B-1908/556-304).
Polypharmacy, potentially inappropriate medications, and Korean anticholinergic burden index
To investigate the current status and characteristics of the prescription pattern in LTCHs in Korea, the medication list at initial assessment was used for analysis. The medication list was defined for oral medications prescribed from 21 days before initial assessment to initial assessment. Although prescribing intervals differ across LTCHs, the time window was defined as 21 days because most LTCHs enter a prescription every 1 to 2 weeks. Polypharmacy and KABS were evaluated in the defined drug list. The numerical definition of polypharmacy was indicated as the simultaneous prescription of 5 or more drugs. Excessive polypharmacy was defined as the simultaneous prescription of 10 or more drugs [28]. A list of 89 PIMs was developed based on the Beers criteria and the 2016 Seoul National University Bundang Hospital Inappropriate Medication for Elderly criteria and adjusted for their clinical significance and frequencies in long term care facilities (Supplementary Table 1) [6,29]. Anticholinergic burden was evaluated using the KABS, and a KABS score of 3 and above was defined as a strong anticholinergic effect or high anticholinergic burden [14].
Statistical analysis
Descriptive statistics, including mean and standard deviation for continuous variables and frequency and percentages for categorical variables, are provided. The independent t test and chi-squared test were used for continuous and categorical variables, respectively, to compare the patients’ baseline characteristics according to the anticholinergic burden. The relationship between frailty status, multi-morbidity, demographic data, ADL, cognition, depression, communication, and pain, EQ-5D, polypharmacy, or other confounding factors and KABS was determined using logistic regression. We used logistic regression analysis to evaluate the clinical factors associated with the high anticholinergic burden among LTCH patients while adjusting for demographic variables (age, sex, body mass index [BMI], medical aid beneficiary, and length of hospital stay). Adjusted odds ratios (aORs) with 95% confidence intervals (CI) are reported.
All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA) and p < 0.05 was considered significant with two-tailed analysis. All data from the participants were de-identified and analysed anonymously.
RESULTS
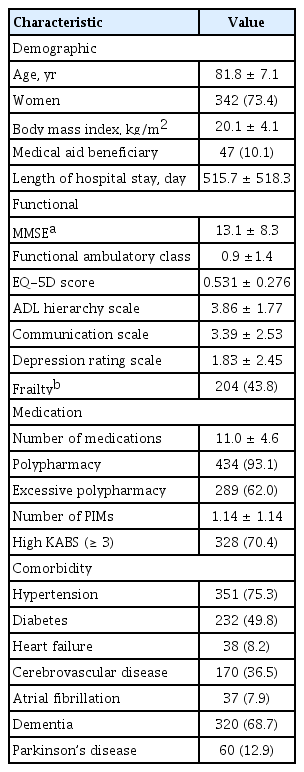
From September 5, 2019 to January 31, 2020, 508 patients were enrolled from LTCHs. After excluding 42 patients who did not complete an initial assessment because of unexpected death (n = 4), transfer to another institution or hospital (n = 16), discharge before assessment (n = 5), refusal for assessment (n = 16), or withdrawal of consent (n =1), 466 patients were included in the final analysis. The mean age of the participants was 81.8 ± 7.1 years and women accounted for 73.4% (n = 342). Hypertension was the most common comorbid condition (75.3%) followed by dementia (68.7%), diabetes (49.8%), cerebrovascular disease (36.5%), Parkinson’s disease (12.9%), heart failure (8.2%), and atrial fibrillation (7.9%). The mean number of medications and PIMs were 11.0 ± 4.6 and 1.14 ± 1.14, respectively, and 88.8% (n = 414) of patients were prescribed DAPs according to the KABS. The study found that 93.1% and 62% of the participants had polypharmacy and excessive polypharmacy, respectively. The mean KABS was 4.55 ± 3.34, and the proportion of patients with high KABS was 70.4% (n = 328) (Table 1).
Baseline characteristics of the study population
The top 10 frequently prescribed DAPs were quetiapine (47.0%), chlorpheniramine (29.6%), tramadol (22.3%), clonazepam (17.0%), furosemide (16.5%), escitalopram (14.4%), cimetidine (13.1%), alprazolam (12.4%), trazodone (10.5%), and guaifenesin (5.6%). Drugs with a KABS score of 1, 2, and 3 contributed to 27.0%, 37.9%, and 35.1% of the cumulative KABS score, respectively. Quetiapine (KABS 2, 20.7%), chlorpheniramine (KABS 3, 19.5%), tramadol (KABS 2, 9.8%), cimetidine (KABS 2, 5.8%), and furosemide (KABS 1, 3.6%) had the highest contribution to the total KABS score (Fig. 1). According to drug category, the most frequently prescribed DAPs were antipsychotics (49.4%), antihistamines (36.1%), anxiolytics (32.2%), antidepressants (31.3%), and analgesics (23.0%).
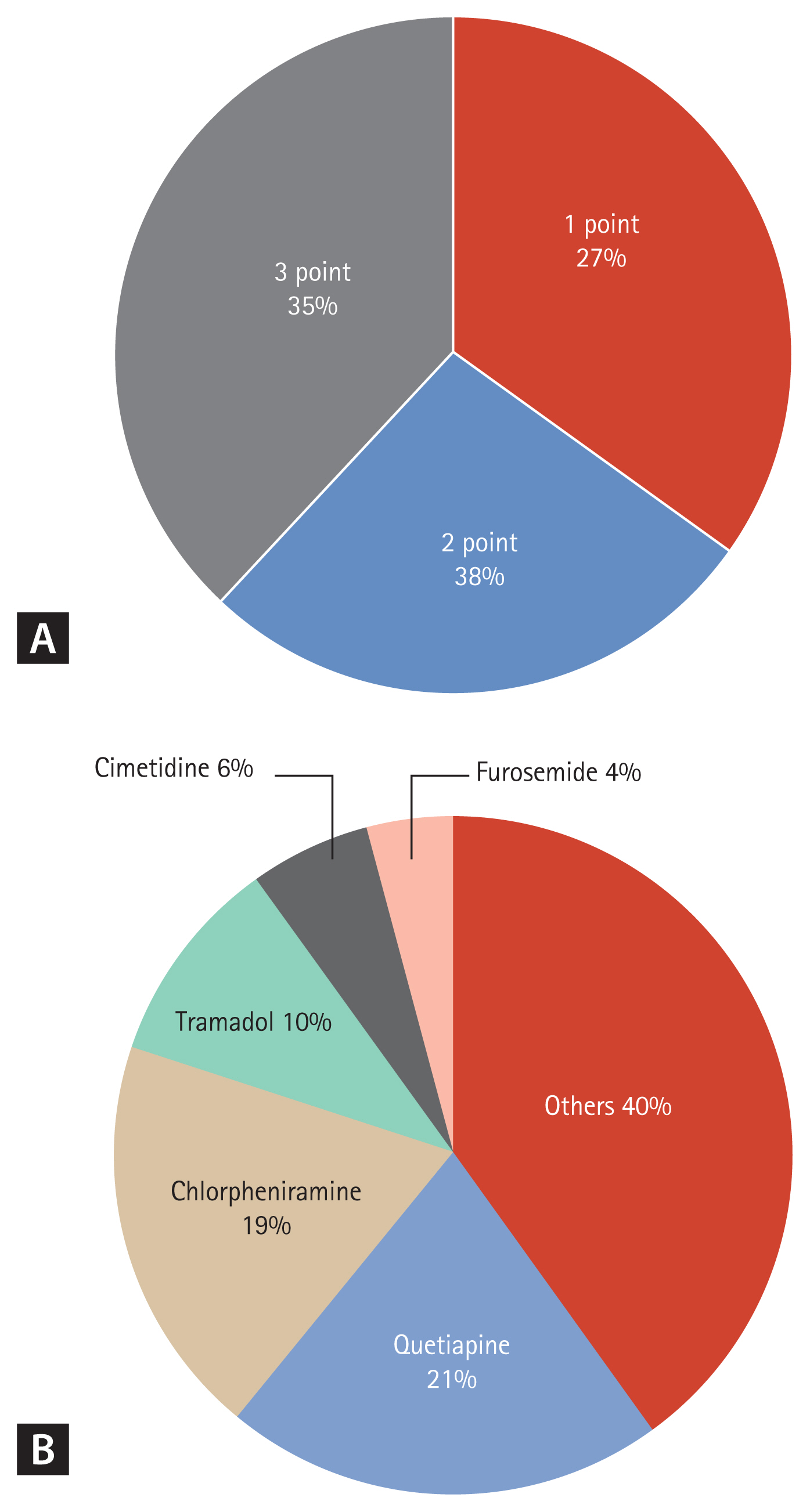
Distribution of (A) Korean Anticholinergic Burden Scale (KABS) score of medications and (B) specific medications that contributed to the total KABS burden of the study population. Medications of KABS scores 1, 2, and 3 contributed 27%, 38%, and 35%, respectively, to the total KABS burden. The top five medications with the highest contribution to the total KABS burden were quetiapine (21%), chlorpheniramine (19%), tramadol (10%), cimetidine (6%), and furosemide (4%).
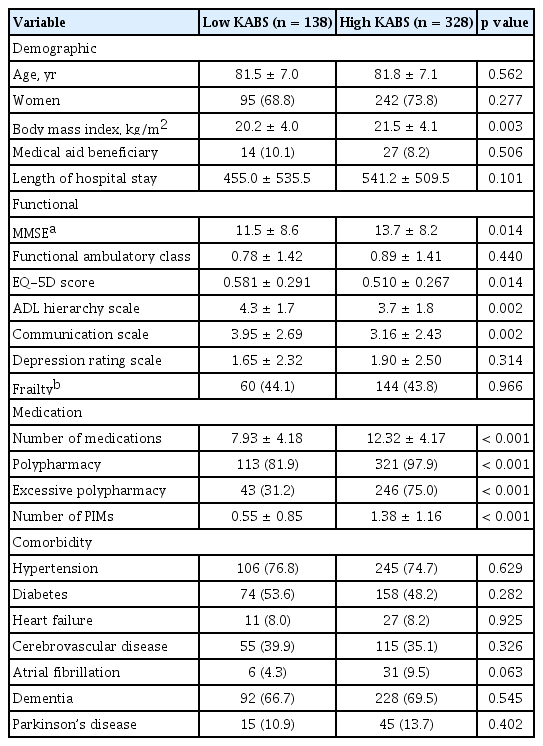
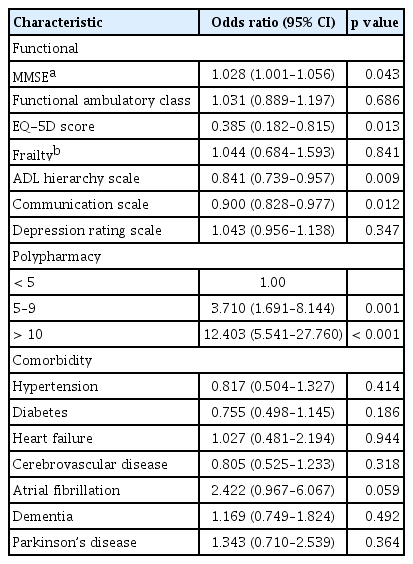
Patients with a greater BMI had high KABS scores. Additionally, lower ADLH scale, communication scale, and EQ-5D scores and a higher MMSE score were associated with high KABS, as were polypharmacy, excessive polypharmacy, and the number of PIMs (Table 2). Logistic regression analysis adjusted for age, sex, BMI, medical aid beneficiary status, and length of hospital stay revealed a significant association between high KABS and a higher MMSE score (aOR, 1.028; 95% CI, 1.001 to 1.056), lower EQ-5D score (aOR, 0.385; 95% CI, 0.182 to 0.815), polypharmacy (aOR, 3.71; 95% CI, 1.691 to 8.144), excessive polypharmacy (aOR, 12.403; 95% CI, 5.541 to 27.760), moderate ADL dependence (ADLH ≥ 5, aOR, 0.489; 95% CI, 0.322 to 0.744), and moderate impairment of communication (COMM ≥ 4, aOR, 0.611; 95% CI, 0.400 to 0.933) (Table 3).
Comparison of demographic, functional, medical, and comorbidity components by low and high KABS prescription
Factors associated with a high anticholinergic burden: univariate analysis with adjustment
DISCUSSION
The study results revealed a higher administration of DAPs to LTCH patients who are less dependent and have better communication and cognitive functions. This trend was maintained even after adjusting for age, sex, BMI, status of medical aid beneficiary, and length of hospital stay. Patients with a high burden of DAPs had a poorer quality of life and tended to use more drugs (7.93 vs. 12.32, respectively; p < 0.001). This pattern was similar to that observed in previous studies conducted in LTCF in Helsinki [30]. The drugs with the highest contribution to the total KABS score were quetiapine (KABS 2, 20.7%), chlorpheniramine (KABS 3, 19.5%), tramadol (KABS 2, 9.8%), cimetidine (KABS 2, 5.8%), and furosemide (KABS 1, 3.6%).
The prevalence of DAP prescription in LTCHs was 88.8% (n = 414), and this was higher than in previous research conducted in LTCF, which ranged from 30% to 77% [31,32]. This difference in DAP prevalence is likely due to the varied drug list used to define DAPs and the different population characteristics. Possibly, the patients in Korean LTCHs had excellent access to prescriptions, and the proportion of severe dementia was relatively small compared to those in nursing homes (mean cognitive performance score: 2.7 vs. 3.2); thus, more complaints of pain or non-specific symptoms for various geriatric diseases, such as urinary incontinence, dermatitis, insomnia, or allergy, could be expected [32]. Contrary to other countries where most long-term care institutions are nursing homes, in Korea, various medical services, including subacute, palliative, and rehabilitation care, are provided in LTCHs. Patients pay only 10% to 20% of the total medical fees because most of the citizens are eligible for coverage under the National Health Insurance Program. The prescription pattern observed in this study is characterized by frequent use of central nervous system active drugs (antipsychotics, 49.4%; anxiolytics, 32.2%; and antidepressants, 31.3%), antihistamines (36.1%), and analgesics (23.0%), which is consistent with that observed in a previous study conducted in LTCF [33].
In previous observational and retrospective cohort studies, a high burden of DAPs was associated with adverse cognitive impact or incident dementia [15,34]. However, in another study, similar to the current study, the use of DAPs was associated with better cognition and functioning [9,30]. This finding may be related to several medical and non-medical factors. First, since the priority of medical treatment in LTCHs is improving quality of life rather than improving survival or guideline-based chronic disease management, patients with poor cognitive or communication function are likely to have been prescribed a lower number of DAPs because their symptom complaints are not frequent or clear. Second, previous studies have emphasized the avoidance of DAPs, which may impact cognition, delirium, or behavioural symptoms [35,36]. Therefore, patients with low cognitive function may have possibly tried adjusting medications or reducing the unnecessary DAPs to improve delirium. An increase in the number of DAPs according to the KABS, from 0 to more than 3 (p = 0.28 in Kruskal-Wallis test), was associated with a stepwise decrease in the quality of life (Fig. 2). Although further study is needed to investigate causality between DAP use and cognitive function, physical function, or quality of life, we showed a dose-response relationship between the DAP burden and quality of life of LTCH patients.
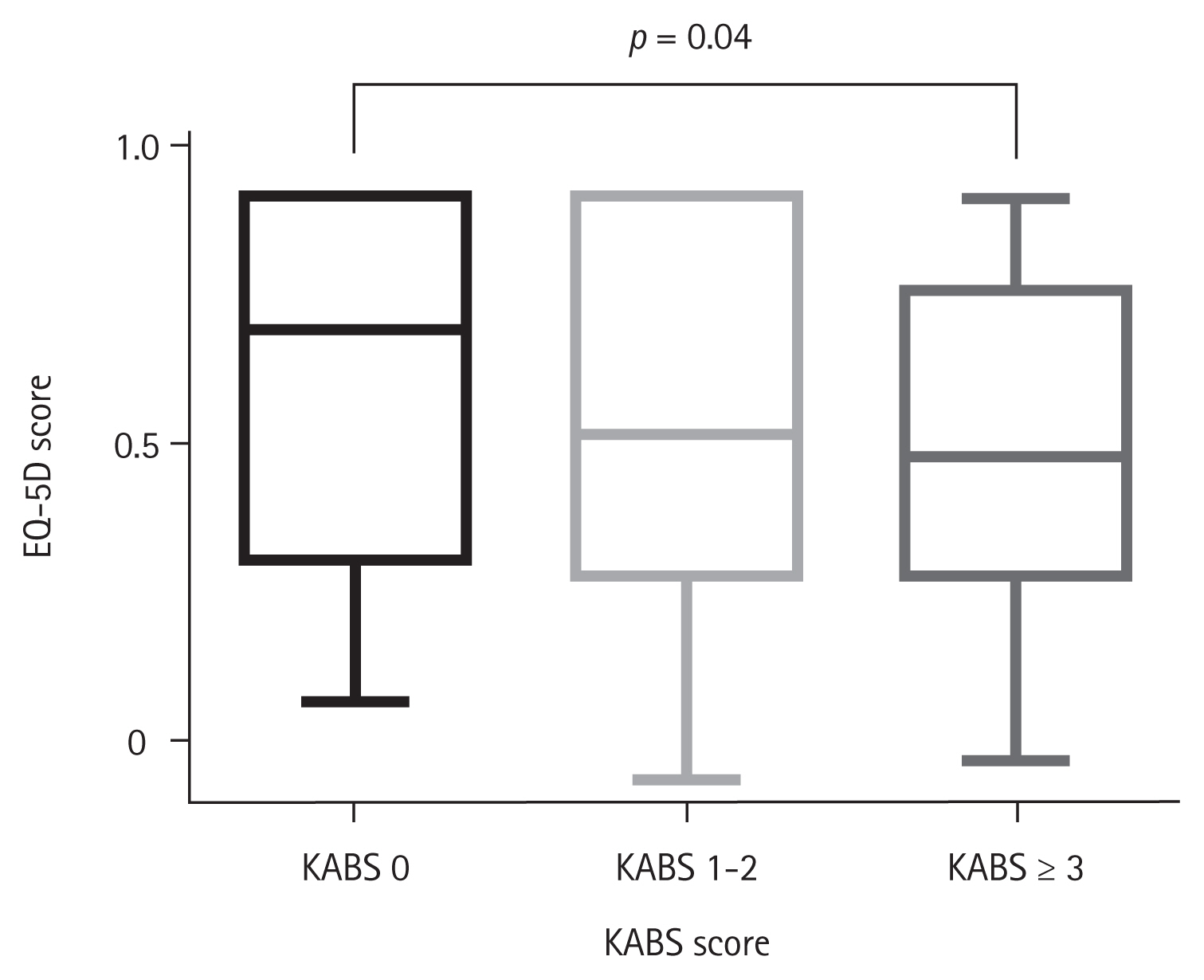
Quality of life score according to the anticholinergic burden: no anticholinergic medication (Korean Anticholinergic Burden Scale [KABS] 0), intermediate burden of anticholinergic medications (KABS 1–2), and high burden of anticholinergic medications (KABS 3 or more). There was a significant difference in the quality of life score according to the anticholinergic burden (KABS 0 vs. 3 or more, p = 0.01).
DAPs have central and peripheral antagonist effects on muscarinic receptors, leading to delirium, falls, cognitive impairments, constipation, and dry mouth [31,33]. In a previous study, DAPs were widely prescribed for various diseases in older adults, including Parkinson’s disease, depression, cardiovascular disease, urinary incontinence, asthma, and allergies [37]. Older patients in LTCHs were more likely to be exposed to polypharmacy, PIMs, and DAPs because of their disease patterns, frailty, pain, and non-specific symptoms. In this study, although there was no difference in the number of PIMs (1.20 vs. 1.12, p = 0.571) and anticholinergic burden (KABS, 4.65 vs. 4.53, p = 0.746) according to disease burden (number of comorbidities ≥ 4), more medications (11.98 vs. 10.77, p = 0.022) were prescribed to the group of patients with high disease burden. As the use of DAPs in LTCHs is inevitable, a periodic automatic monitoring system is needed for proper management of the patients. The medical staff in LTCHs also need an appropriate consultation system to facilitate the control of symptoms and to prevent disease aggravation without the need to transfer the patients to regional acute care hospitals. To solve these unmet needs for patients and medical staff in LTCHs, access to information on PIMs could be provided by linking the electronic medication record of the LTCH to the Health-RESPECT platform, along with periodic videoconferencing with the geriatrician of the regional acute care hospital, to ensure timely care of acute conditions [17]. In addition, linking the Health-RESPECT system to the health information exchange network system can ensure real-time monitoring and adjustment of PIMs and DAPs.
Our study had several methodological strengths. In contrast to previous research that used claim data, we used cross-sectional drug exposure data, which can be considered more reliable because the data were extracted directly from each electronic medication record of the LTCH. In addition, the Health-RESPECT program, a system to share and cooperate with regional acute care hospitals, was established to access PIMs or DAPs and facilitate intervention in further practice. However, our study was limited by the cross-sectional design, which cannot determine causality. Further observational studies are needed to identify the prevalence of adverse outcomes related to DAP administration.
In conclusion, the prevalence of DAP administration in this study was 88.8% (n = 414), and 70.4% (n = 328) of the patients had a high burden of DAPs. Patients with a prescription of many DAPs (high KABS) tended to have higher BMI, less dependence, better communication and cognitive functions, and poorer quality of life. The long-term relationship between DAP administration and adverse clinical outcomes in older LTCH patients should be investigated in further observational or cohort studies.
KEY MESSAGE
1. Over 70% of long-term care hospital (LTCH) patients experienced high anticholinergic burden, and quetiapine (20.7%), chlorpheniramine (19.5%), tramadol (9.8%), cimetidine (5.8%), and furosemide (3.6%) mostly contributed.
2. High anticholinergic burden in LTCHs is associated with polypharmacy, less dependence, better cognitive function, and poor quality of life.
3. It is necessary to develop and apply a medication management program considering the high prevalence, adverse impact, and characteristics of LTCH patients.
Notes
No potential conflict of interest relevant to this article was reported.