Prognostic outcome of treatment modalities for epidermal growth factor receptor-mutated advanced lung cancer
Article information

Abstract
Background/Aims
The treatment of epidermal growth factor receptor (EGFR)-mutated lung cancer cases has shown remarkable development in the past two decades. However, there have been limited studies comparing the prognostic effects of EGFR-tyrosine kinase inhibitor (TKI) and other treatment modalities. Therefore, we compared the survival outcomes of patients treated with EGFR-TKIs versus those treated with other treatment modalities.
Methods
Patient data were collected from the Korean National Health Insurance Database, National Health Insurance Service-National Sample Cohort 2002 to 2015, which was released by the Korean National Health Insurance Service in 2015. The lung cancer group included patients (n = 2,003) initially diagnosed with lung cancer between January 2010 and December 2013. The main outcome was all-cause mortality. A Cox proportional hazard regression analysis was used to calculate the relative risk of mortality.
Results
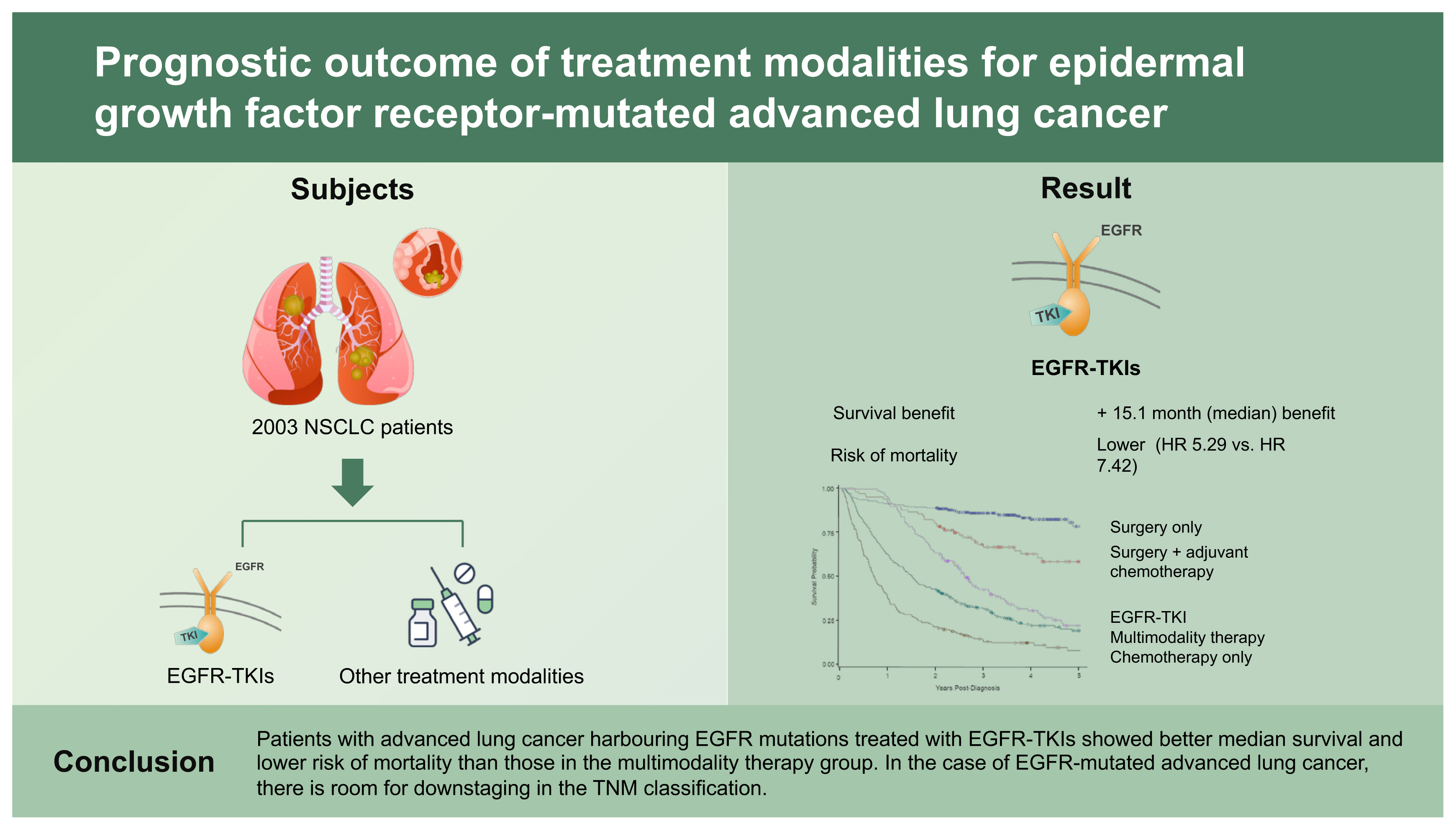
Among the newly diagnosed lung cancer cases, 1,004 (50.1%) were included in the analysis. A 15.1-month median survival benefit was observed in the EGFR-TKI group than that of the multimodality therapy group. The risk of mortality was as follows: EGFR-TKI treatment group (n = 142; hazard ratio [HR], 5.29; 95% confidence interval [CI], 3.57 to 7.86) and multimodality therapy group (n = 326; HR, 7.42; 95% CI, 5.19 to 10.63) compared to surgery only (n = 275).
Conclusions
Patients with advanced lung cancer harbouring EGFR mutations treated with EGFR-TKIs showed better median survival and lower risk of mortality than those in the multimodality therapy group. In the case of EGFR-mutated advanced lung cancer, there is room for downstaging in the TNM classification.
INTRODUCTION
Drugs effective against epidermal growth factor receptor (EGFR)-mutated lung cancer have emerged and been tested in numerous randomised controlled studies [1–4]. However, only a limited number of studies have compared the prognosis of patients with lung cancer harbouring EGFR mutations and treated them with different treatment modalities while controlling variables affecting co-morbidity and prognosis in real-world treatment settings.
Remarkable progress has been made in the treatment of driver mutations [5–7]. Furthermore, it has been suggested that information on driver mutations should be included in the tumor, node, and metastasis (TNM) classification [8,9]. Lung cancer staging is determined by tumour size and location, as well as lymph node and distant metastases [10]. Furthermore, the tumour stages are adjusted by analysing the survival rate based on active treatment [11,12].
However, few studies have investigated the differences in prognoses of EGFR-mutated lung cancer patients with advanced disease who relapse after treatment with primary EGFR-tyrosine kinase inhibitor (TKI) versus other multimodality therapies. Therefore, the aim of this study was to compare the survival of lung cancer patients treated with EGFR-TKI versus those treated with other treatment modalities.
METHODS
Database
This database was described earlier [13]. Briefly, this study used data from the National Health Insurance Service-National Sample Cohort (NHIS-NSC) 2002 to 2015, released by the NHIS in 2015, which includes all medical claims filed from January 2002 to December 2015 for 1,031,392 nationally representative randomly selected patients, accounting for approximately 2.2% of the entire population of the NHIS in 2002. The current study was approved by the Institutional Review Board (IRB) of Keimyung University Dongsan Hospital (IRB 2018-05-016). The IRB waived the requirement for informed consent.
Patient identification
Patients with newly diagnosed lung cancer between January 2010 and December 2013 were enrolled in this study (Fig. 1). The codes of the International Classification of Diseases, 10th revision (ICD-10), were used as a reference for diagnosing the disease as well as for identifying data within the National Health Insurance (NHI) database, since the codes for lung cancer cases diagnosed before 2010 were maintained in the NHI database. New lung cancer cases were identified and counted by including newer cases registered during the calendar year after excluding pre-existing lung cancer. Patients with lung cancer (C34) were included only if they were identified with a special code, V193 or V194, designated by the NHIS, Korea. The NHIS-NSC data are linked to the Statistics Korea (national statistical office) data, which allows for the accurate identification of deaths by death certificate records.
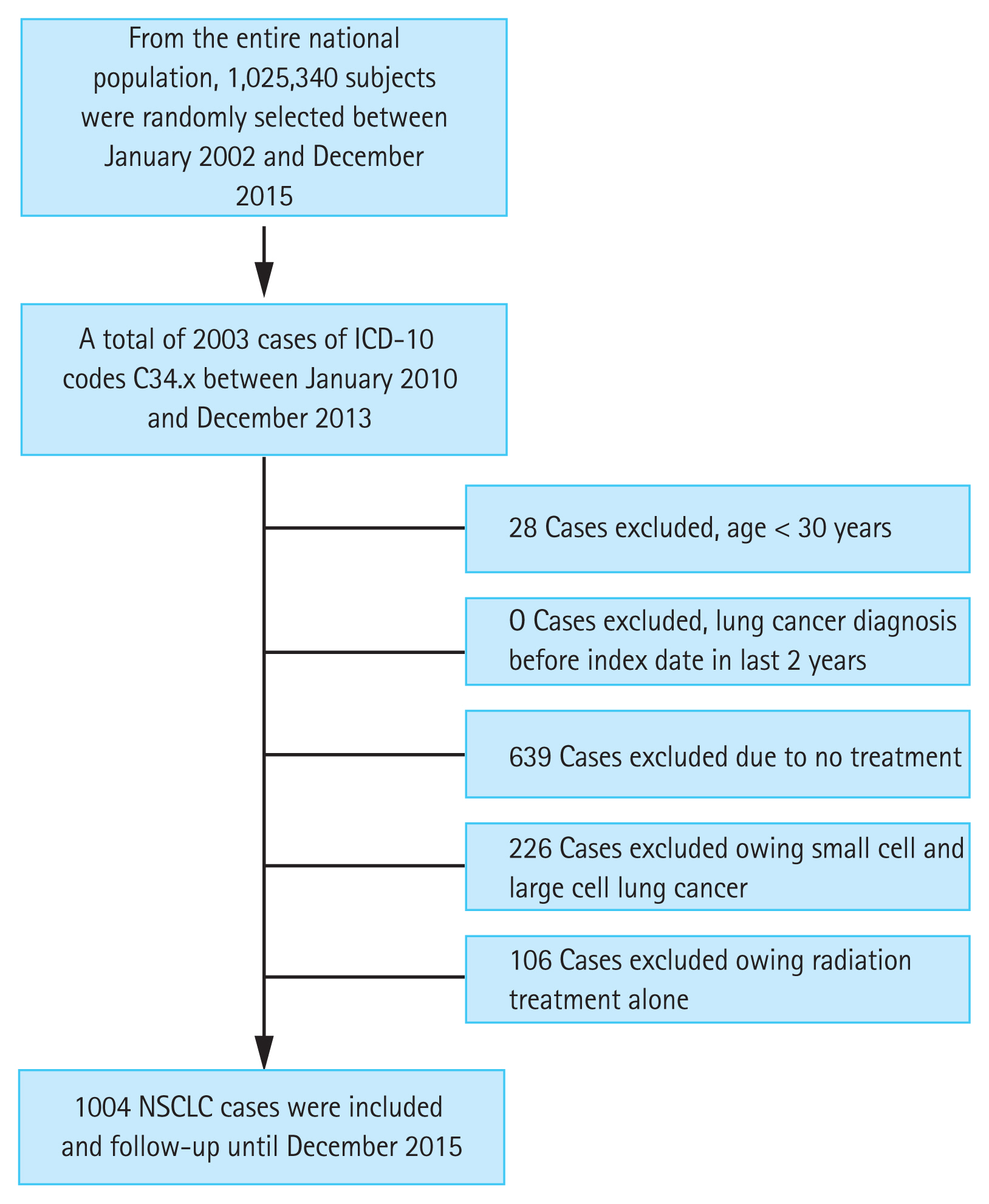
Flow chart of the study. Patient selection flow chart of non-small cell lung cancer (NSCLC). ICD-10, International Classification of Disease 10th revision.
Patient inclusion
The selection criteria for patients with small cell lung cancer or advanced stage large cell carcinoma were as follows: first-line treatment within 6 months of lung cancer diagnosis, using either cisplatin/carboplatin plus etoposide combination or regimen containing irinotecan/topotecan. In the treated lung cancer patients, 226 (16.9%) were classified as small cell lung cancer or large cell carcinoma.
Next, patients who underwent wedge resection and lobectomy before and after the diagnosis of lung cancer and who did not undergo adjuvant chemotherapy within 3 months were classified into the surgical group. The surgical codes were as follows: wedge resection (O1401, O1402), segmentectomy (O1410), lobectomy (O1421, O1422, O1423, O1424), and pneumonectomy (O1431, O1432). Patients who underwent wedge resection, lobectomy, bilobectomy, or pneumonectomy following adjuvant chemotherapy within 3 months of diagnosis were classified into the adjuvant chemotherapy group. Anticancer drug dosage codes (KK152, KK153, KK154) were used to distinguish cases of anticancer drug administration.
The irradiation codes were as follows: external radiation therapy (HD051, HD052, HD053, HD054, HD055, HD056), arc therapy (HD057, HD058, HD059), conformal therapy (HD061), fractionated stereotactic radiation therapy (HD110), stereotactic body radiation therapy (HD111, HD112 HD211 HD212), and intensity-modulated radiation therapy (HZ271). However, patients treated with radiotherapy alone (n = 106) were excluded from the analysis.
Patients who received two or more modalities, such as surgery, radiation, or chemotherapy within 3 months after lung cancer diagnosis were classified into the multimodality therapy group. However, patients who received anticancer drugs within 3 months after surgery were excluded from the study.
Next, the EGFR-TKI group was defined as patients who received TKI for more than 2 months for the treatment of advanced stage lung cancer [14]. However, patients who received EGFR-TKI after recurrence post local treatment such as surgery or concurrent chemoradiation therapy, were excluded from this group, since multimodality therapy may interfere with the effectiveness of EGFR-TKI therapy.
Finally, the untreated cases were defined as those who never underwent surgery, radiation, or chemotherapy until death, after the diagnosis of lung cancer. Among the total lung cancer cases (n = 2,003), 639 (31.9%) were untreated. The treated cases were defined based on the medical claim data.
Co-morbidities
Patient comorbidities, which were followed after diagnosis and identification using ICD-10 codes from 2002 until the index date, included ischaemic heart disease, cerebrovascular diseases, hypertension, and diabetes mellitus.
Statistical analysis
Baseline characteristics at the date of diagnosis (age, sex, body mass index, smoking status, comorbidities, residential area, and household income) for cases and controls were summarised using descriptive statistics such as proportions. The chi-square test was used to compare the frequencies of variables between the survivor and non-survivor patients. Univariate and multivariate Cox regression models were used to evaluate mortality risk. Multivariate Cox regression models were constructed using patient age groups (30–49, 50–59, 60–69, 70–79, ≥ 80 years), sex, body mass index, smoking status, comorbidities, geographic location (capital, large cities, other), household income (high, middle, low, very low, Medicaid), and treatment modalities. Survival time was defined as the interval from the date of lung cancer diagnosis up to the last follow-up or death. Kaplan-Meier survival curves were used to calculate the 5-year survival rate for patients in different treatment groups. A post hoc analysis was used for multiple comparisons of the survival curves. The Harrell C index was used to evaluate the discriminatory ability of the staging systems. Statistical significance was set at p < 0.05. Statistical analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC, USA), SPSS version 24 (IBM Corp., Armonk, NY, USA), and STATA version 14.0, (StataCorp., College Station, TX, USA).
RESULTS
Baseline characteristics
The baseline characteristics of the patients (n = 1,004) are summarised in Table 1. Fifty-three percent of the patients had a history of cigarette smoking. For the initial therapy, 261 patients (25.9%) were treated with two or more combinations of surgery, radiation, and chemotherapy. EGFR-TKI therapy as first- or second-line treatment after chemotherapy was considered in 134 patients (13.4%). We enrolled 227, 244, 257, and 276 newly diagnosed non-small cell lung cancer patients in 2010, 2011, 2012, and 2013, respectively. The incidence of lung cancer during the study period was 48.3 cases per 10,000 person-years for all ages.
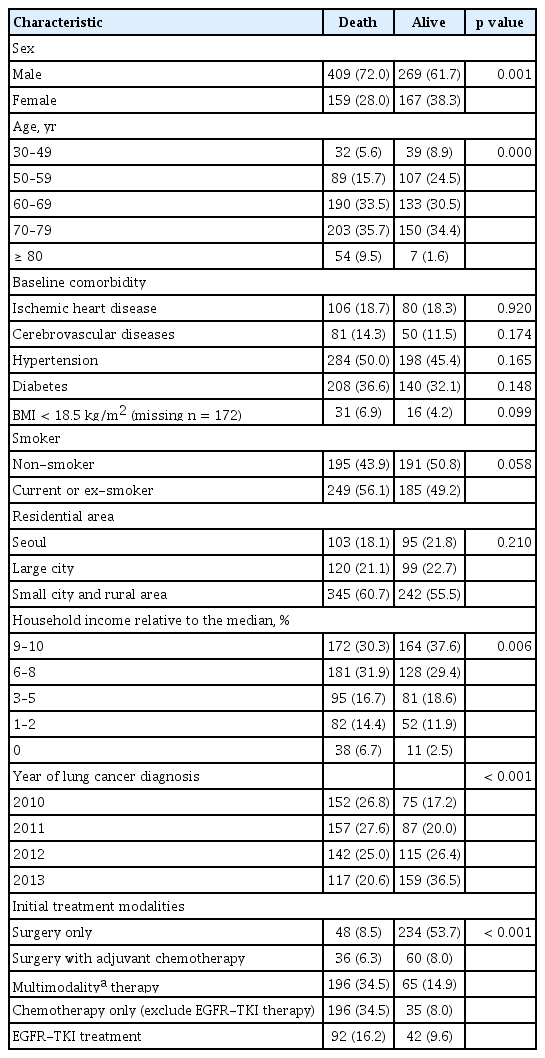
Demographic and clinical characteristics of patients with lung cancer
Risk factors associated with survival
Multivariate Cox regression analyses indicated a correlation with survival, where men were found to be at 1.38 times higher risk of mortality than females (Table 2). Furthermore, compared to patients aged 50 years, those aged 70 and 80 years had 1.2- and 2.4-time higher risk of mortality, respectively.
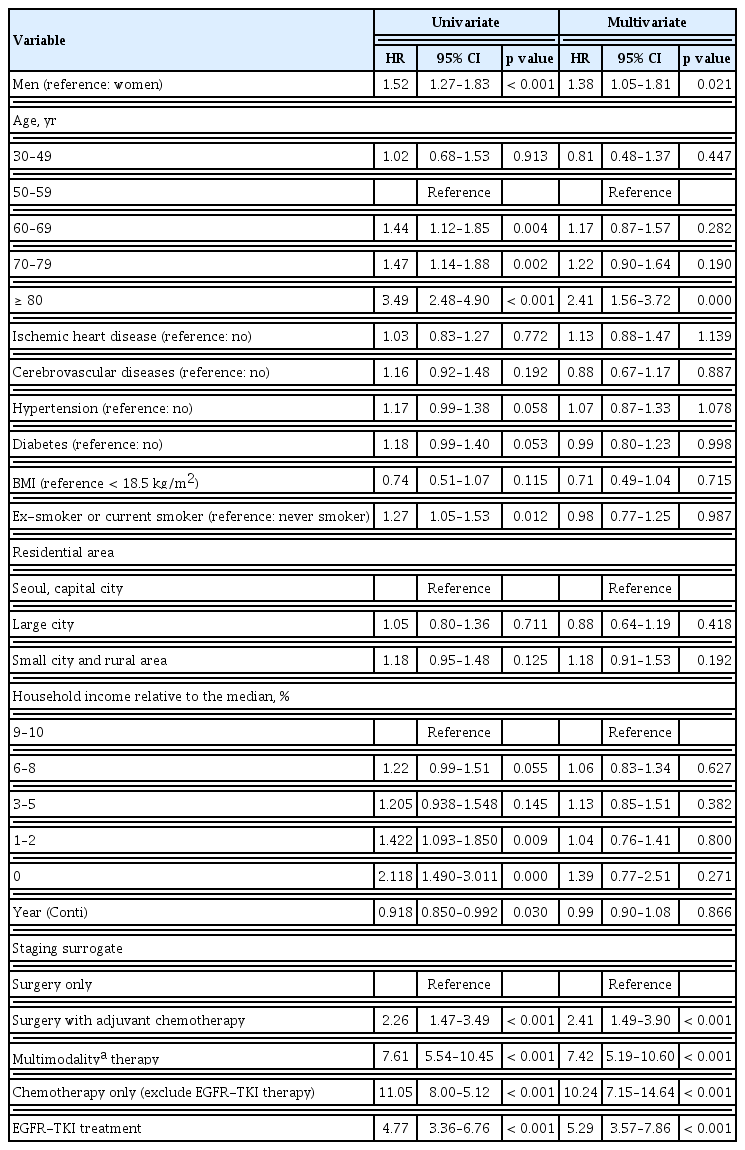
Univariate and multivariate Cox proportional hazard regression analyses for factors associated with the survival of EGFR mutated advanced lung cancer
The risk of mortality in patients receiving surgery plus adjuvant chemotherapy, multimodality therapy, chemotherapy alone, and EGFR-TKI was 2.4, 7.4, 10.2, and 5.2 times, respectively, that of those treated with surgery alone. Moreover, the magnitude of hazard ratios of the types of therapy was found to be stable in the multivariate analysis. While patients belonging to Medicaid, low household income groups, and smokers were found to be at an increased risk of mortality in the univariate analysis, the statistical significance could not be validated in the multivariate analysis. Additionally, the prognosis of the patients was independent of the year of diagnosis.
Comparison of survival analyses in advanced-stage lung cancer patients treated with EGFR-TKI and other treatment modalities
Next, we observed that the 5-year survival rates in patients treated with surgery, adjuvant chemotherapy, surgery plus chemoradiation therapy, chemotherapy alone, and EGFR-TKI were 78.2%, 58.2%, 18.9%, 9.7%, and 22%, respectively (Fig. 2).
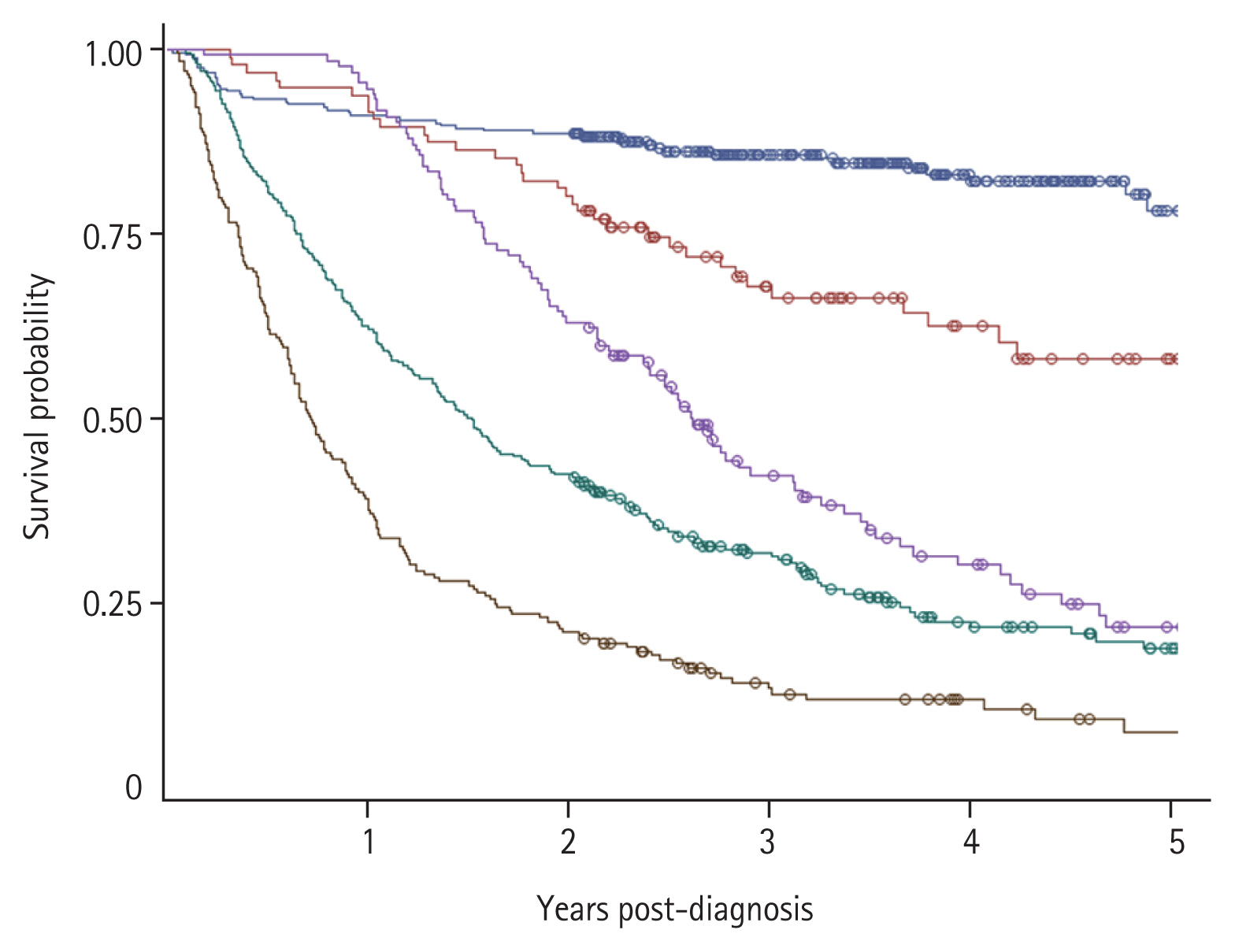
Survival curves for patients treated with surgery only (blue), surgery plus adjuvant chemotherapy (red), multimodality therapy (green), epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitor (TKI) (purple) and chemotherapy alone (brown).
Further, the median survival duration for patients in the multimodality treatment group was significantly less than that in the EGFR-TKI group (16.2 months vs. 31.3 months; 95% confidence interval [CI], 13.1–19.0 vs. 28.5–37.3) (Fig. 2). Whereas the median survival in the chemotherapy alone group was 10.4 months (95% CI, 8.2 to 12.0). Moreover, as shown in Fig. 2, the survival curves of each treatment modality appear well-separated from each other. Additionally, post hoc analyses for comparisons of survival curves in each group indicated statistical significance, as follows: EGFR-TKI group vs. chemotherapy alone (p < 0.001); EGFR-TKI vs. multimodality therapy group (p < 0.001); EGFR-TKI vs. surgery plus adjuvant chemotherapy (p < 0.001); and EGFR-TKI vs. surgery alone (p < 0.001), along with a C-index of 0.71 (95% CI, 0.69 to 0.73) for this staging system.
Overall survival between EGFR-TKI following multimodality therapy and EGFR-TKI as primary therapy
Next, we compared the survival rates conferred by EGFR-TKI as secondary treatment in patients who relapsed after treatment with multimodality therapy versus those who received it as a primary therapy. Our analysis suggested that median survival durations in patients treated with EGFR-TKI after multimodality therapy and those treated with EGFR-TKI as a primary therapy were 33.0 months (95% CI, 29.6 to 44.4) and 28.7 months (95% CI, 22.1 to 41.7), respectively. However, the survival gains at 4 months observed in this analysis did not reach statistical significance (Fig. 3).

Survival curves for patients treated with primary epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitor (TKI) (blue line) and those receiving EGFR-TKI after recurrence and treatment with multimodality therapy (red line).
DISCUSSION
The analysis indicated that treatment of advanced-stage lung cancer patients harbouring EGFR mutations, using EGFR-TKI, conferred better survival outcomes along with a 25% reduced hazard ratio than in those treated with multimodality therapy. The multimodality therapy group, which accounted for 25.9% of the lung cancer patients, was considered as clinical stage III and matched well with the lung cancer registry data [15]. Moreover, each survival curve, including that for the EGFR-mutated lung cancer group, was well separated and achieved statistical significance, as confirmed by the C-index value.
Although the median survival of patients in the EGFR-TKI group was better than that in the multimodality group, which may include a 9- to 13-month period of resistance development [1,4,16–18], we did not observe significant differences in their 5-year survival outcomes. Here, patients with advanced lung cancer had a better prognosis upon treatment with primary EGFR-TKI than those treated with multimodality therapy for locally advanced tumours. Therefore, EGFR-TKI therapy for the treatment of patients with stage IIIB and higher stage tumours harbouring EGFR mutations may be considered to downstage the disease.
As reported previously, the 24-month survival of patients with stage IIB and IIIA lung cancer defined by clinical staging was 72% and 55%, respectively [19]. In this study, the survival rate for advanced lung cancer patients treated with EGFR-TKI was 63%, which is closer to stage IIB disease. However, while the 5-year survival of stage IIB and IIIB lung cancer patients defined by clinical staging was 53% and 26%, respectively [19], patients in our study showed a 22% survival outcome, which is closer to stage IIIB disease. Therefore, these comparisons again correlate with the development of resistance to EGFR-TKI therapy. Evidence suggests the effectiveness of treatment with osimertinib and dacomitinib, along with combination therapy, such as bevacizumab, which may allow updating the position in the TNM classification of patients with EGFR-mutated lung cancer [6,20–22].
EGFR mutations were identified as an important factor in the response to EGFR-TKIs in the Iressa Pan-Asia Study (IPASS) study in 2009 [2]. Therefore, the use of EGFR-TKIs has been based on EGFR mutation status in advanced lung cancer (stage IIIb and IV). At the beginning of 2010, EGFR-TKIs were used as the primary treatment for EGFR-mutated advanced lung cancer. However, the NHIS has recommended concurrent chemoradiation therapy for patients with stage III lung cancer who have good general conditions, regardless of their EGFR mutation status. In these patients, EGFR-TKI can be used as the initial treatment when the Eastern Cooperative Oncology Group (ECOG) is 2 or higher. Therefore, patients with the same stage of EGFR-mutated lung cancer can be treated differently.
Furthermore, a median survival gain of 4 months was observed in patients treated with EGFR-TKI after multimodality therapy than in patients treated with EGFR-TKI as a primary therapy. Although the analysis failed to reach statistical significance, multimodal therapy may play a significant role in the outcome of EGFR-mutated lung cancer. Moreover, low tumour burden may contribute to improving the survival of patients with advanced stage disease treated in the multimodality therapy group than in the primary EGFR-TKI therapy group [23,24]. However, previous studies reporting the role of multimodality therapy in the treatment of locally advanced lung cancer with mutated EGFR have been controversial [25]. Therefore, a large cohort study is required to evaluate the effect of multimodality therapy on lung cancer patients with EGFR mutations. It would be necessary to compare the prognosis of EGFR-mutation-positive and EGFR-mutation-negative patients in the conventional treatment group that did not use EGFR-TKI; however, the analysis was not conducted due to the small number of EGFR-mutated lung cancers in this group [14].
At present, TNM staging does not include information on age, sex, and comorbidities. However, it appears necessary to also provide this information for prognosis. In this study, male sex and age above 80 years were identified as independent risk factors, even when treatment-related variables were controlled. Therefore, these epidemiological variables may also need to be incorporated into the treatment policy along with TNM staging.
This study has several limitations. First, the study results could not directly confirm the EGFR mutation status or type. Given the high cost of EGFR-TKI treatment, the NHIS strictly restricts this treatment unless the patient is positive for EGFR mutation. Therefore, the administration of EGFR-TKI treatment in patients without EGFR mutation would be rare when EGFR mutation types have not been identified. Second, since no information about the TNM classification was available, it was traced back through treatment. Moreover, data on patient performance were not included. Third, comorbidities defined based on ICD codes should have been validated through patient records. However, the database consisted of random samples of national insurance claim data without identification numbers, which prevented the validation of individual cases through chart review. Fourth, as the database did not include information on pathology, we could not perform further analyses.
In conclusion, treatment of advanced stage lung cancer patients harbouring EGFR mutations with EGFR-TKI, either as first- or second-line after chemotherapy, increased the median survival with a low hazard ratio compared to treatment with multimodality therapy. Therefore, we anticipate EGFR-TKI therapy to downstage tumours harbouring EGFR mutations in the TNM classification.
KEY MESSAGE
1. In the case of epidermal growth factor receptor (EGFR)-mutated advanced lung cancer, there is room for downstaging in the tumor, node, and metastasis (TNM) classification.
2. EGFR-tyrosine kinase inhibitor (TKI)-treated advanced lung cancer showed better survival than the multimodality therapy group, which was considered as locally advanced lung cancer.
3. Survival may not differ between primary EGFR-TKI therapy or multimodality therapy following EGFR-TKI therapy for EGFR-mutated locally advanced lung cancer.
Acknowledgments
This research was supported by a faculty grant from Myongji Hospital (2002-09-04). We thank the participants of the Korean Health Insurance Cohort study and the National Health Insurance Service, who developed the NHIS-NSC database.
Notes
No potential conflict of interest relevant to this article was reported.