The burden of symptomatic patients with chronic spontaneous urticaria: a real-world study in Korea
Article information

Abstract
Background/Aims
Chronic spontaneous urticaria (CSU) poses a considerable burden both on the quality of life (QoL) of individual patients and on healthcare systems. Real‑world data evaluating the disease burden of CSU are limited in this country. This study evaluated the disease burden and healthcare resource utilization (HRU) among symptomatic CSU patients.
Methods
This multicenter, noninterventional, retrospective, and cross-sectional study assessed CSU patients symptomatic for more than 6 months despite step-wise H1-antihistamine medications. Primary outcomes included Urticaria Activity Score over 7 days (UAS7) and Chronic Urticaria QoL scale (CU-QoL). Secondary outcomes included EuroQol 5-Dimension 5-Level (EQ-5D-5L), Dermatology Life Quality Index (DLQI), association of disease activity with QoL, medications used for the past 6 months, and HRU.
Results
Five hundred patients with CSU were enrolled. Mean disease duration was 3.7 years. Based on UAS7, 22.2% of patients were in well-controlled status and 31.2%, 28.4%, and 18.2% of them had mild, moderate, and severe disease, respectively. Mean CU-QoL and DLQI scores were 57.5 ± 29.7 and 10.2 ± 7.6, respectively, while the EQ-5D-5L utility score was 0.8 ± 0.2. H1-antihistamines were prescribed to 95% of patients, while omalizumab was prescribed to 33% of patients. Most patients (98%) had outpatient visits in the past 6 months. Negative correlations were noted between UAS7 and CU-QoL, EQ-5D-5L, EQ-5D-5L visual analog scale scores, but a positive correlation was noted with DLQI score (p < 0.001 for all). The number of outpatient department visits increased with disease activity (p = 0.001).
Conclusions
CSU affects QoL, leading to increased HRU, particularly in patients with severe disease.

INTRODUCTION
Chronic urticaria (CU) is defined as wheals (hives), angioedema, or both lasting more than 6 weeks [1]. CU can be classified as chronic spontaneous urticaria (CSU), previously recognized as chronic idiopathic urticaria, with the spontaneous appearance of hives and angioedema due to unknown cause, and chronic inducible urticaria (CIndU) for which specific eliciting factors are involved [1]. The worldwide prevalence of CSU is reported to vary between 0.02% and 5.0%, with women having a disproportionately higher incidence and a median age of onset in the 50s [2-7]. The prevalence of CSU in the Korean population ranges between 0.16% and 2.3%, at a similar level [2].
According to the joint initiative by the Korean Academy of Asthma, Allergy and Clinical Immunology (KAAACI) and the Korean Dermatological Association (KDA), nonsedating H1-antihistamines are the first-line treatment for CSU [2]. It has been observed that 50% of patients with CSU continue to be symptomatic despite their treatment with approved doses of H1-antihistamines. In case of inadequate response, the dose of antihistamines can be increased up to four times, but this is effective in only 45% to 50% of patients [8-10]. In addition, leukotriene receptor antagonists have been used, either as a single therapy or in combination with H1-antihistamines [1,2]. In patients who are unresponsive to H1-antihistamines, guidelines recommend treatment escalation to omalizumab and immunomodulators such as cyclosporine [1,11].
CSU is a debilitating skin condition, and its impact goes beyond the skin. CSU has a profound impact on quality of life (QoL) due to anxiety, depression, sleep disturbance, and comorbidities, including autoimmune and endocrine disorders [1,12,13]. Along with QoL impairment, patients with CSU pose a considerable economic burden on the healthcare system [14]. Previous studies such as ASsessment of the Economic and Humanistic Burden of Chronic Spontaneous/Idiopathic URticaria PatiEnts (ASSURE-CSU) (2015) and A World-wide Antihistamine-Refractory chronic urticaria patient Evaluation (AWARE) (2017), which evaluated the burden of disease among patients resistant to H1‑antihistamines, highlighted that symptomatic patients with CSU have poor QoL, and inadequate response to treatment poses a significant impairment to health-related quality of life (HRQoL) and leads to extensive healthcare resource utilization (HRU) [14,15]. However, very few patients who were prescribed omalizumab were included since it had not launched or had not come into wide use at the time of conduct of these studies [14].
There have been no studies in Korea assessing the disease burden on symptomatic patients with CSU in terms of patient-reported outcomes (PROs), HRU, and their relationships, particularly after the approval of omalizumab for the treatment of CSU. The present study evaluated the burden of disease, including HRQoL and HRU, in symptomatic patients with CSU in Korea.
METHODS
Study design and subjects
This is a multicenter, noninterventional, retrospective, and cross-sectional study assessing adult patients with inadequately controlled CSU who visited outpatient departments across eight tertiary hospitals in South Korea from June 2020 to December 2020. The study had two components: (1) a 6-month retrospective medical chart review including patient medical record abstraction and (2) a cross-sectional patient survey containing several validated PROs (Fig. 1). Baseline demographics and clinical characteristics were assessed cross-sectionally, while medications used and HRU data from the past 6 months were collected through retrospective medical chart review. PRO data, including disease activity and HRQoL, were surveyed once at time of enrollment.

Study design. Baseline demographics and clinical characteristics were assessed cross-sectionally, while medications used and healthcare resource utilization data from the past 6 months were collected through retrospective medical chart review. Patient-reported outcome (PRO) data including disease activity and health-related quality of life, were surveyed once at time of enrollment. CU-QoL, Chronic Urticaria Quality of Life questionnaire; DLQI, Dermatology Life Quality Index; UAS7, Urticaria Activity Score over 7 days; EQ-5D-5L, EuroQol 5-Dimension 5-Level.
Patients were enrolled if they were ≥ 19 years of age, had a confirmed diagnosis of CSU based on the International Classification of Diseases, Tenth Revision (ICD-10) codes (L50.1, L50.8, L50.9), had an outpatient department visit at the time of enrollment, had received treatment for CSU during the past 6 months, and were symptomatic, including on the day of enrollment, despite standard care [2,16]. Symptomatic CSU was defined as chronic recurrent symptoms with unstable disease activity for > 6 months which was confirmed by patient interview and medical record review. Patients were excluded from the study if they had a sole diagnosis of CIndU (ICD-10 L50.2, L50.3, L50.4, L50.5, L50.6) without a diagnosis of CSU, if their symptoms resolved within 6 months of diagnosis, or if they were participating in a CSU/CIndU interventional study during the data collection period.
This study was approved by the Institutional Review Board (IRB) of Ajou University Hospital (AJIRB-MED-SUR-20-052) along with seven other participating hospitals. Written informed consent was obtained from each patient who participated in the study.
Patient-reported outcomes
The primary study variables and outcomes of interest were disease activity using the Urticaria Activity Score over 7 days (UAS7) and disease-specific HRQoL using the CU‑QoL scale. The UAS7 is a two-item assessment scale based on the aggregated rating of urticaria symptoms (US) in terms of the number of hives and intensity of itch measured once daily for 7 consecutive days. The scores range from 0 to 42, with a higher score indicating greater disease activity [17]. The CU-QoL is a 17-item instrument with four domain scores: current US, emotional distress (ED), food and environmental distress (FE), and stigma. The total score is reported on a scale of 0 to 100, with higher scores suggesting better HRQoL [18].
Other variables assessing QoL associated with CSU were EuroQol 5-Dimension 5‑Level (EQ-5D-5L) and Dermatology Life Quality Index (DLQI) scores. EQ-5D-5L consists of five domains (mobility, self-care, daily activity, pain/discomfort, and anxiety/depression) and a visual analog scale (VAS). EQ-5D-5L utility scores (range from 0 to 1) were calculated using responses to the five domains, and VAS score recorded as the patient’s self-rated health status on a graduated (0 to 100) scale, with higher scores indicating better QoL [19]. The DLQI is a 10‑item instrument and includes the follow-ing domain: symptoms and feelings, daily activities, leisure, work or school, personal relationships, and side effects of treatment. Each question is scored on a 4-point Likert scale, resulting in a maximum score of 30 and a minimum score of 0, with a higher score representing worse QoL [20].
Other outcome parameters
Data for all medications prescribed for the management of CSU in the past 6 months were collected and categorized by line of therapy recommended by the guidelines [11]. For assessing the HRU, data on the frequency of outpatient department visits, hospitalizations, and emergency room (ER) visits due to CSU were collected. In addition, whether CSU would be the cause of each hospital visit was verified through physicians’ medical chart reviews. The cost per case of HRU (i.e., outpatient department visit, hospitalization, and ER visit) was estimated from the Health Insurance Review & Assessment Service (HIRA) disease medical statistics information for idiopathic urticaria (L50.1) and medical service fee [21,22]. It was then multiplied by the frequency of each HRU to calculate the total cost.
Total costs = cost per case (outpatient department visit, hospitalization, and ER visit costs) × frequency of each HRU.
Additionally, all costs were converted from Korean won (KRW) to US dollars (USD) using the average exchange rate (1,184.15 KRW = 1 USD) in December 2021 [23].
Statistical analysis
Results are presented as mean ± standard deviation (SD) or frequency (%). Mean values with SD were calculated for continuous variables; counts were collected, and percentages within each category were computed for categorical variables.
Descriptive statistical analyses were used for baseline characteristics, disease activity (UAS7), HRQoL (CU-QoL, EQ-5D-5L, DLQI), medication use in the past 6 months, and HRU. The results were stratified by disease activity using the four UAS7 disease activity states: ≤ 6 (well‐controlled urticaria activity), 7–15 (mild activity), 16–27 (moderate activity), and 28–42 (severe activity) [24,25]. Associations between disease activity (UAS7) and HRU or patients’ HRQoL were analyzed using analysis of variance (ANOVA), Pearson correlation, or chi-square test. Univariate or multivariate linear regression was used to analyze factors associated with CU-QoL. Statistical analyses were performed using the SAS software version 9.4 (SAS Institute, Cary, NC, USA) and R Statistics version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria), and a two-tailed p < 0.05 was considered statistically significant.
RESULTS
Patient characteristics
A total of 500 patients with CSU were enrolled in eight recruitment centers. Baseline characteristics of participants are presented in Table 1. Participants included 321 (64.2%) female patients with a mean age of 44.6 ± 13.1 years. The mean duration of CSU was 3.7 ± 3.9 years, and the mean duration of current symptoms was 2.4 ± 2.8 years. CSU was accompanied by allergic airway diseases, CIndU, angioedema, and atopic dermatitis in 208 (41.6%), 108 (21.6%), 55 (11.0%), and 28 (5.6%) patients, respectively. Additionally, nine (1.8%) patients had autoimmune thyroiditis. The mean UAS7 (0–42) score in patients with CSU was 16.4 ± 11.4 (Table 1).
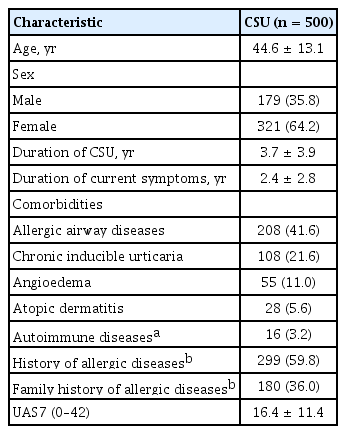
Patient characteristics
Medication use
All enrolled patients had been treated under the diagnosis of CSU during the past 6 months. Overall, 475 (95.0%) patients were prescribed H1-antihistamines, of whom 39.6% used H1-antihistamines only (29.0% used a single H1-antihistamine, while 10.6% used multiple H1-antihistamines). A total of 302 (60.4%) patients used other therapies in combination with or without H1-antihistamines, wherein omalizumab was the most commonly used therapy (190 patients, 38.0%) (Table 2). Of the 500 included patients, 187 (37.4%) were prescribed oral corticosteroids. Overall, 298 (59.6%) patients were on first- or second-line therapy (i.e., patients receiving H1‑antihistamines and their combinations), while 202 (40.4%) patients were on third‑line therapy and were receiving omalizumab, cyclosporine, or their combination (Table 2).
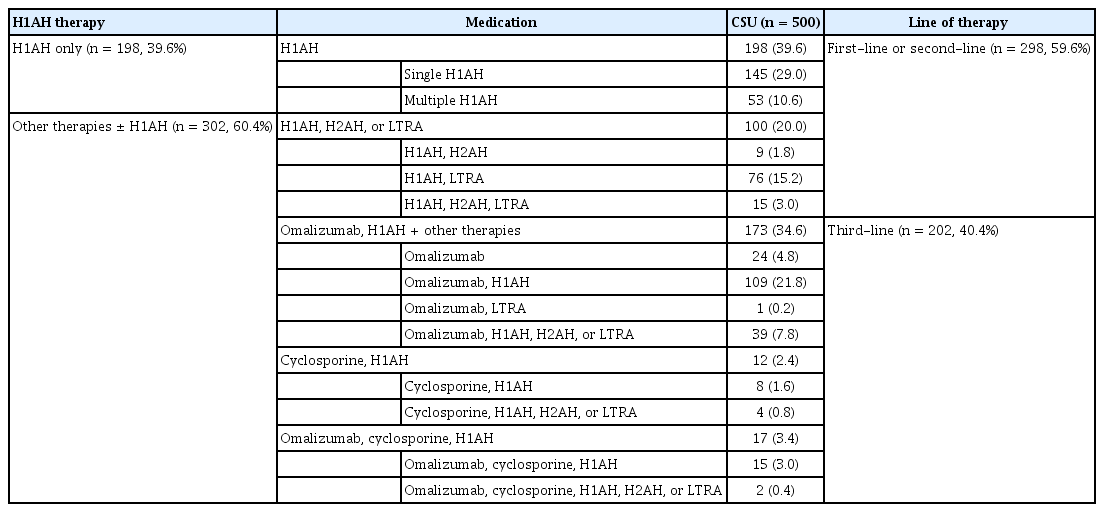
Medication used among patients with CSU in the past 6 months
Disease activity and HRQoL scores
All of the recruited patients completed CU-QoL, EQ-5D-5L, DLQI, and UAS7 surveys. Based on UAS7 assessed at enrollment, 111 (22.2%) patients were in well-controlled status, and 156 (31.2%), 142 (28.4%), and 91 (18.2%) had mild, moderate, and severe disease, respectively (Fig. 2). Overall, 233 (46.6%) patients were classified as having “moderate-to‑severe” CSU (UAS7 score ≥ 16). The proportion of patients who had received third-line therapy during the past 6 months increased with UAS7 activity: 36.9% (41/111) for well-controlled, 37.2% (58/156) for mild, 43.7% (62/142) for moderate, and 45.1% (41/91) for severe patients (Fig. 2).
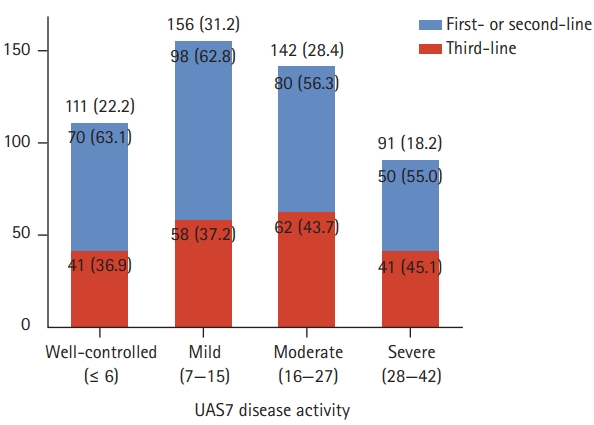
The number of patients according to Urticaria Activity Score over 7 days (UAS7)-disease activity. Patients were divided into four groups according to their UAS7 score: well-controlled (≤ 6), mild (7–15), moderate (16–27), and severe (28–42). The number of patients and the ratio of line of therapy in each disease activity is presented. Data are presented as number (%).
The mean scores for overall CU-QoL, US, ED, FE, and stigma domains were 57.5 ± 29.7, 42.0 ± 32.9, 53.8 ± 34.5, 58.0 ± 35.1, and 73.5 ± 32.4, respectively. The mean EQ‑5D-5L utility, EQ-5D-5L-VAS, and DLQI scores were 0.8 ± 0.2, 69.2 ± 19.3, and 10.2 ± 7.6, respectively. For all three HRQoL measurements, the mean scores among the four UAS7 activity states were significantly different (p < 0.001), with poorer HRQoL as disease activity worsened (Fig. 3).
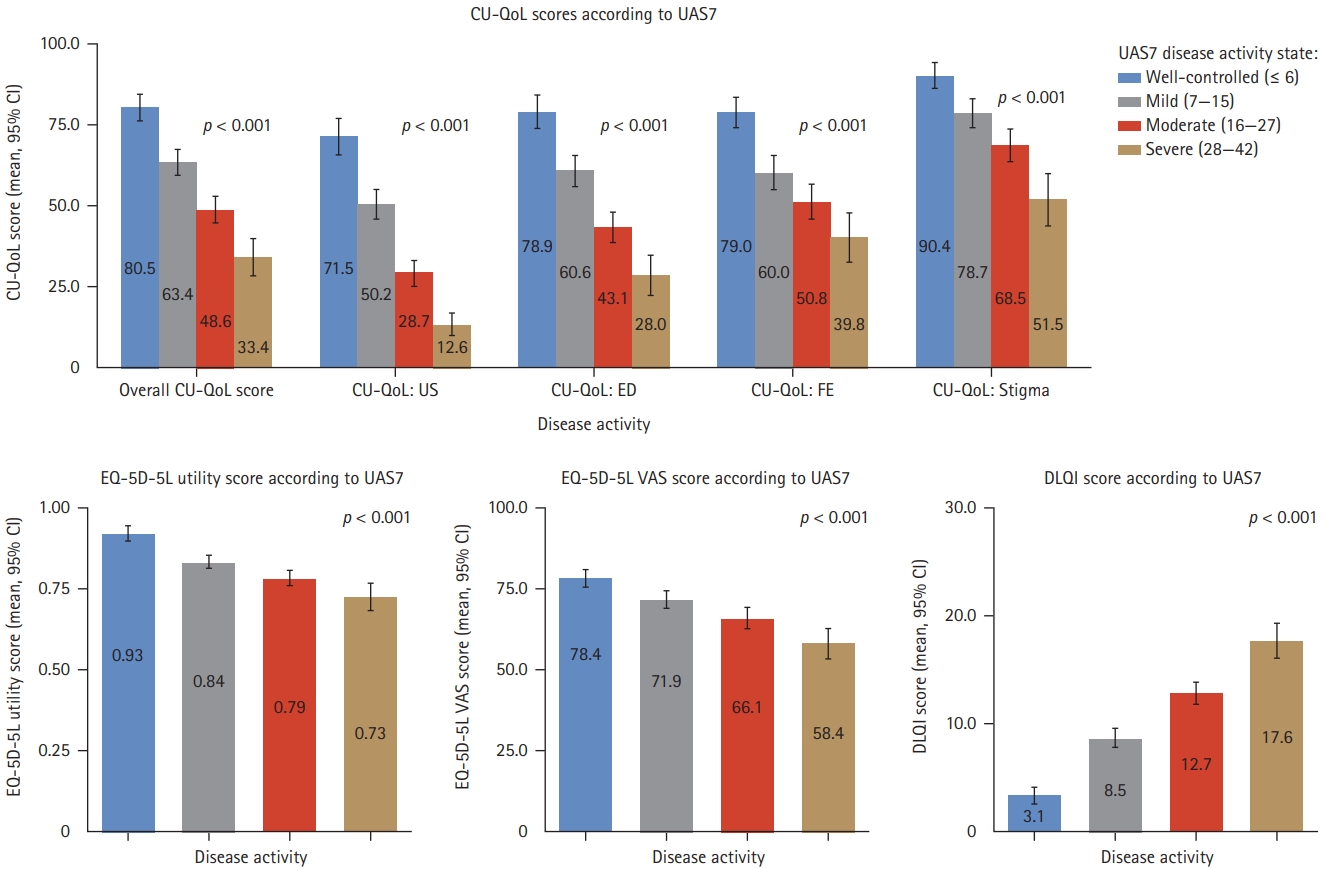
Health-related quality of life scores according to Urticaria Activity Score over 7 days (UAS7)-diasese activity. Patients were divided into four groups according to their UAS7 score: well-controlled (≤ 6), mild (7–15), moderate (16–27), and severe (28–42). The mean scores of Chronic Urticaria Quality of Life questionnaire (CU-QoL), EuroQol 5-Dimension (EQ-5D), and Dermatology Life Quality Index (DLQI) in each disease activity are presented. CI, confidence interval; US, current urticaria symptom; ED, emotional distress; FE, food and environmental distress; EQ-5D-5L, EuroQol 5-Dimension 5-Level; VAS, visual analog scale.
Healthcare resource utilization
Almost all included patients (490, 98.0%) visited the outpatient department during the study period. The mean number of outpatient department visits for the past 6 months was 4.0 ± 2.8; 67 (13.4%) patients showed ≥ 7 outpatient department visits (Table 3). Additionally, 18 (3.6%) patients visited the ER, and 14 (2.8%) patients were hospitalized due to CSU in the past 6 months. Of these, two (0.4%) patients experienced both hospitalization and ER visit.
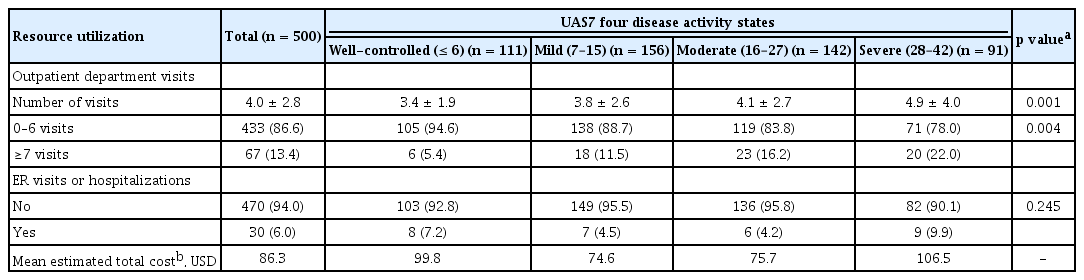
Healthcare resource utilization in the past 6 months
As disease activity worsened (i.e., higher UAS7 score), the number of outpatient department visits also increased (p = 0.001). No significant differences were observed in ER visits or hospitalization among the four UAS7 activity states(p = 0.245). The overall cost per patient for the management of CSU was $86.3, with no difference according to disease activity (Table 3).
Correlation of HRQoL and disease activity
In the study, we observed that QoL worsened with an increase in disease activity (i.e., higher UAS7 score) (Table 4). CU-QoL and EQ-5D-5L utility scores showed negative correlations with UAS7 (correlation coefficient, –0.562 and –0.432, respectively; p < 0.001). The DLQI score positively correlated with UAS7 (correlation coefficient, 0.677; p < 0.001). All HRQoL tools correlated significantly with each other. The correlation between CU-QoL and DLQI, a disease-specific HRQoL assessment tool, was higher than the correlation with EQ-5D, a generic QoL measure (CU-QoL and DLQI correlation coefficient, –0.815; p < 0.001).

Correlation between HRQoL and UAS7
Factors associated with CU-QoL
Female sex and patients being on third-line therapy were found to be significant factors associated with a decrease in CU-QoL score (Table 5). Further, patients in the “mild,” “moderate,” and “severe” UAS7 category were significantly associated with a decrease in CU-QoL score compared with patients with well-controlled UAS7 (Table 5).
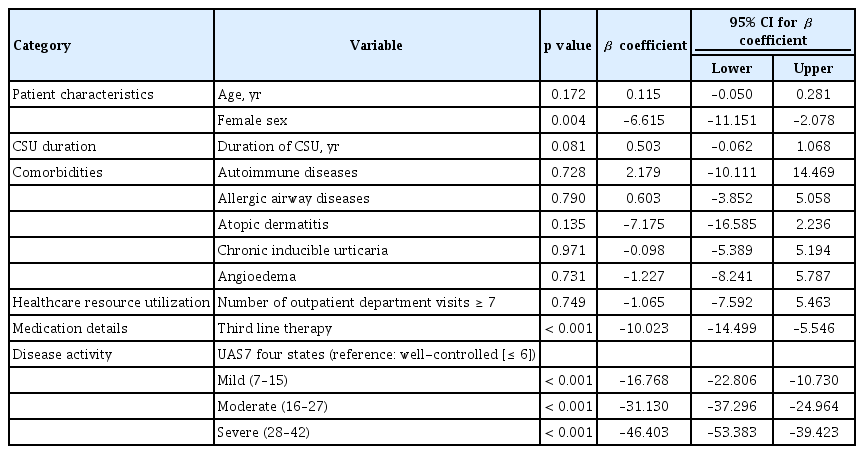
Multivariate regression for CU-QoL score
DISCUSSION
This real-world study evaluated the overall disease burden of symptomatic patients with CSU in a clinical setting, where omalizumab was available as a treatment option. Symptomatic patients with CSU with treatment history during the past 6 months were enrolled, and their current disease activity, HRQoL, and the impact of previous treatment were assessed. PROs were assessed through various measures such as UAS7, CU-QoL, EQ-5D-5L, and DLQI scores, and the association between disease activity (UAS7) and HRQoL was also evaluated. The present study adequately represents the real-world situation of patients with CSU in Korea, as it was conducted in eight tertiary hospitals where CSU treatment is actively performed.
In the present study, 64.2% of patients with CSU were female. This finding is substantiated by a recent meta-analysis of worldwide population‐based studies, in which women were more affected by urticaria than men [26]. In the ASSURE study, around 70% of patients were reported to have moderate-to-severe CSU, with a mean disease duration of 5 years [27]. This was in line with the results of our study, wherein the overall disease duration of CSU was around 4 years, with nearly 50% of patients categorized as having moderate-to‑severe CSU.
In the present study, patients were treated following the recommended guidelines and previously published studies, suggesting that investigators who participated in the study adhered to urticaria treatment guidelines, contributing to a higher quality of patient care [28,29]. However, some notable differences were observed in the treatment pattern in comparison with other real-world studies, such as ASSURE-CSU and AWARE [14,15]. All (100%) patients enrolled in this study were prescribed medications to treat CSU in the past 6 months, whereas 18.1% of patients in ASSURE and 29.9% in AWARE study at baseline did not receive any treatment [14,15]. In the present study, 35% of patients (who were in uncontrolled status on H1-antihistamines) received omalizumab following the KAAACI/KDA recommendations, and the percentage of patients receiving third-line therapy increased as disease activity worsened (proportion of third-line therapy use in each UAS7 disease category: 36.9% for well‑controlled, 37.2% for mild, 43.7% for moderate, and 45.1% for severe) [11]. However, in the ASSURE-CSU study, less than 6% of patients received omalizumab [14]. This difference could be attributed to omalizumab not being approved for CSU at the time of data collection in the ASSURE-CSU study [14]. Additionally, in the AWARE study, it was observed that the proportion of patients receiving both escalated doses of H1‑antihistamines and omalizumab was quite low although impairment in QoL still remained [30]. Furthermore, a small percentage (11% or less) of patients received escalated doses of H1-antihistamines and omalizumab, indicating a lack of proper treatment in patients with uncontrolled disease [30]. As shown in Fig. 2, among patients with moderate-to-severe CSU (UAS7, 16 to 42), 55.8% still remained on first- or second-line therapy while 44.2% received third-line therapy. Among patients who received third-line therapy, 79.7% had well-controlled, mild, or moderate disease activity. Considering that enrolled patients were still symptomatic for more than 6 months and third-line therapy showed effectiveness in decreasing disease activity, an early and appropriate introduction of step-up treatment based on regular assessment of disease activity could effectively lessen disease burden of patients with CSU.
It has been observed that HRQoL deteriorates significantly in patients with CSU, owing to its unpredictable symptoms [31]. ED is thought to cause CSU and is a common comorbidity among patients with CSU [13]. In the present study, patient’s ED and stigma were evaluated in the subdomains of CU-QoL; however, the presence of anxiety, depression, or other psychiatric illness as comorbidities was not assessed. The poor QoL results of patients with CSU enrolled in this study were consistent with those of previous studies [14,15,32]. It suggests that despite better treatment compliance with treatment guidelines, patients with CSU still have unmet needs and there remains room for improvement in care. In line with previous studies, it was observed that patients with severe disease had worse QoL [31-34]. For all three HRQoL measurements (i.e., CU-QoL, EQ-5D-5L, and DLQI), the mean scores among the four UAS7 activity states differed significantly. Multivariate regression analysis showed that UAS7 continued to be a significant variable in CU-QoL and had a relatively larger coefficient value than other variables. These findings suggest that it may be possible to predict QoL among patients with CSU by assessing disease activity.
Factors that were negatively associated with QoL included female sex and disease activity. In addition to these factors, third-line therapy was also associated with poor QoL. This can be interpreted that as disease activity worsened, patients could not be controlled on first- or second-line treatment and thus presumably had lower QoL, requiring treatment with third-line agents such as omalizumab.
Atopic dermatitis (5.6%) and angioedema (11.0%) were negatively associated with CU-QoL, but the results were not statistically significant in the multivariate analysis. This may be attributed to the high proportion of women with comorbidities affecting QoL in the total population. Autoimmune diseases, atopic dermatitis, and angioedema were observed in 4.0%, 6.5%, and 12.1% of females, respectively, at higher proportions than those in males (1.7%, 3.9%, and 8.9%, respectively). Additionally, angioedema is often underdiagnosed and under-reported in patients with CSU despite being associated with significant CSU activity, poor HRQoL, and productivity impairment [27].
Almost all patients visited the outpatient department in the past 6 months. The results correspond with those from a previously published real-world study, in which 72.1% of patients had at least one visit to a healthcare professional for their CSU in the past 12 months [14]. In our study, as disease activity worsened, the number of outpatient department visits tended to increase. However, ER visits or hospitalization did not increase significantly with an increase in disease activity. This may be because hospitalization and emergency department admission provide more intensive treatment focused on acute symptoms than outpatient departments where the focus is on long‑term disease control. The proportion of patients with ER visits or hospitalization in the past 6 months was higher in severe (9.9%) and well-controlled (7.2%) disease activity states. The high rate reported in well-controlled patients could infer that they previously had severe disease activity requiring hospitalization and ER visits and have now been effectively transitioned to the well-controlled state. The average cost per patient for CSU management was estimated to be $86.3 in the present study, with no correlation with disease activity.
The present study had a few limitations that need to be highlighted. First, the study collected medical information retrospectively, and cross-sectional questionnaires had different recall periods, which may have caused difficulties in interpreting causality and effects. Second, since only patient responses were captured to determine their QoL and disease activity, there could be a discrepancy between subjective disease activity reported by the patient and objective judgment of the physicians for treatment. This could have led to overestimation or underestimation of patient responses and subsequent interpretation of the study results. Third, as the dosage of antihistamine used was not collected, the line of H1-antihistamine therapy (approved dose or increased dose to four-folds) could not be differentiated. Lastly, owing to the coronavirus disease 2019 (COVID-19) pandemic, HRU could have been underestimated due to patients minimizing hospital visits in fear of infection risks during travel or at the hospital.
In conclusion, this study demonstrates that almost half of the symptomatic patients with CSU have moderate-to-severe disease activity despite standard care, and more than half of them remain on first- or second-line therapy. Symptomatic patients with CSU have considerable burden on HRQoL and HRU; disease activity affects the burden of disease. CSU management requires a comprehensive approach that considers the line of therapy, QoL, disease activity, HRU, and PROs.
KEY MESSAGE
1. Almost 50% of symptomatic patients with chronic spontaneous urticaria (CSU) had moderate or severe disease activity. As disease activity worsened, quality of life (QoL) decreased and healthcare resource utilization (HRU) tended to increase.
2. To evaluate the disease burden of CSU, a comprehensive approach is required that considers HRU and patient-reported outcomes, including disease activity and QoL.
Notes
The study was sponsored by Novartis Korea Ltd. Hae-Sim Park has received grants for consulting on this study.
Acknowledgements
The authors thank Ravneet Kohli (Novartis, India) for medical writing support and editorial assistance in preparing the manuscript.