Intravascular imaging and physiologic assessment in ambiguous coronary lesion
Article information

A 66-year-old female presented to our clinic with worsening exertional chest pain for 1 month. This case was approved by the Institutional Review Board as exempt (AJOUIRB-EX-2023-220).
The coronary angiography revealed three-vessel disease with diffuse irregular 80% stenosis at the proximal portion of the left anterior descending artery (pLAD) (Fig. 1A), tubular irregular 77% stenosis at the distal portion of the left circumflex artery (dLCX) (Fig. 1B) and discrete eccentric 80% stenosis at the proximal portion of the right coronary artery (pRCA) (Fig. 1C, D).
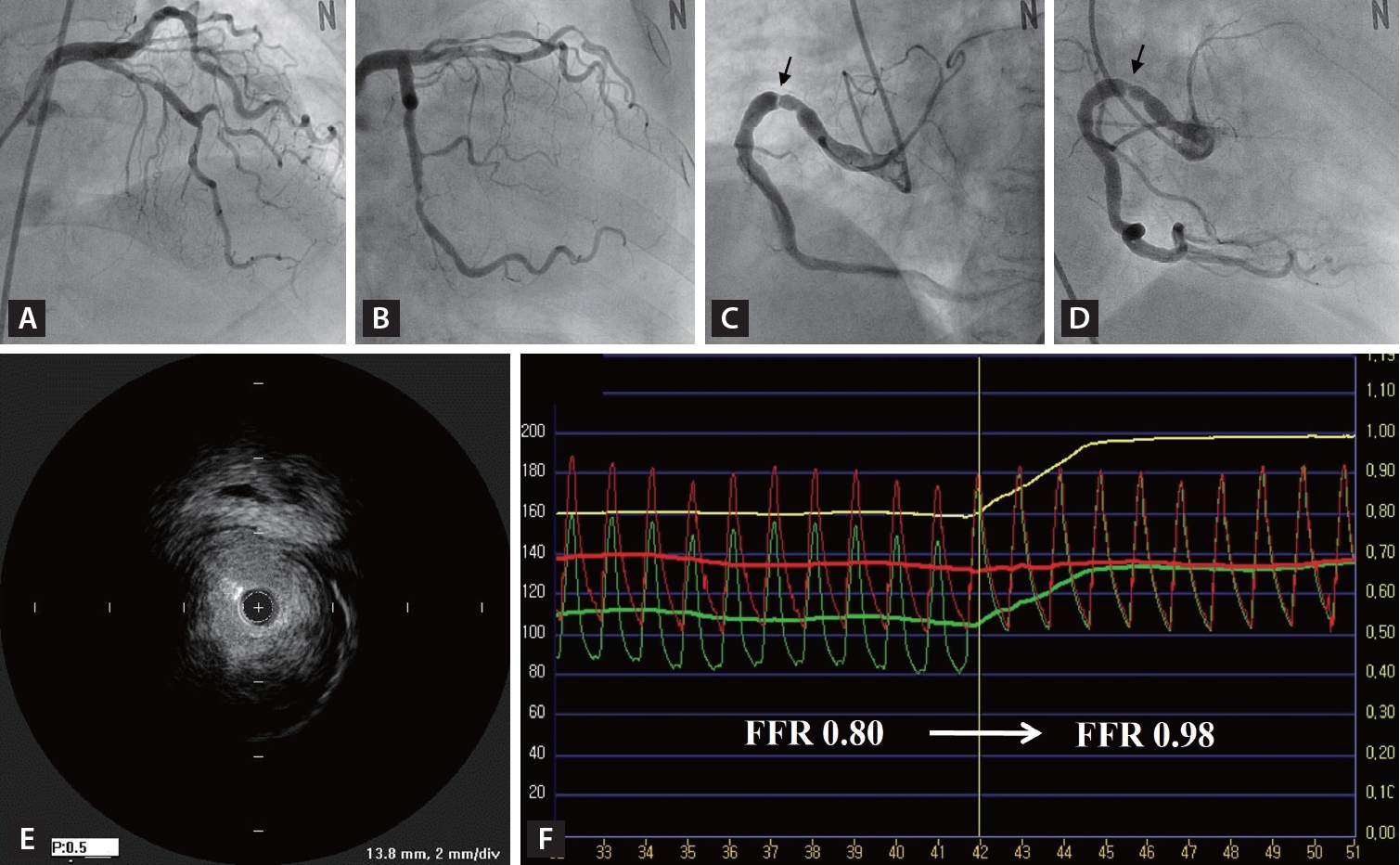
(A, B) Coronary angiography showing significant stenosis at the proximal portion of the left anterior descending artery and the distal portion of the left circumflex artery. (C, D) Angiographically, the lesion of the right coronary artery seems ambiguous owing to its eccentricity and involvement of very short segments. The ambiguous lesion has a web-like appearance at the site of the ectatic vessel segment (arrow). (E) An intravascular ultrasound scan showing the indeterminate lesion, not as a membranous web, but as a discrete eccentric fibrocalcific plaque with a minimal lumen area as 4.2 mm2. (F) The fractional flow reserve rising abruptly from 0.80 to 0.98 upon the withdrawal of the pressure wire through the ambiguous lesion.
Percutaneous coronary intervention (PCI) was performed on the pLAD and dLCX lesions based on angiographic findings. However, the ambiguous nature of the pRCA lesion required further clarification to determine whether PCI is required because of its eccentricity and involvement of very short segments. The angiographic images showed a weblike appearance at the site of the ectatic vessel segment (Fig. 1C, D).
To gather additional important diagnostic information, intravascular ultrasound (IVUS) was performed, and it revealed that the ambiguous lesion was not a membranous web but a discrete eccentric fibrocalcific plaque. The minimal lumen area (MLA) at the lesion site was 4.2 mm2 (Fig. 1E).
To evaluate functional significance, fractional flow reserve (FFR) was measured using pressure wire. The baseline FFR was 0.98. After hyperemia was induced through intracoronary adenosine 240 mcg/kg/min infusion, the FFR decreased to 0.80. However, it rose abruptly from 0.80 to 0.98 upon the withdrawal of the pressure wire through the ambiguous lesion (Fig. 1F).
Based on the MLA measured by IVUS and the FFR, we decided to defer PCI for the indeterminate lesion.
The use of intravascular imaging and functional evaluation should be considered in cases of angiographically ambiguous lesions [1,2].
Notes
CRedit authorship contributions
Kyoung-Woo Seo: writing - original draft; Jin-Sun Park: conceptualization, data curation, formal analysis, writing - review & editing
Conflicts of interest
The authors disclose no conflicts.
Funding
None