Changes of the Carotid Artery Doppler Flow Velocity Pattern after Sublingual Nitroglycerin in Patients with Hypertension
Article information
Abstract
Objective
To evaluate the applicability of carotid Doppler echography for the assessment of changes of peripheral hemodynamics in the hypertensives.
Subjects
28 hypertensives (17 males, 11 females), mean age of 64 yrs and 40 normal controls (24 males, 16 females) mean age of 49 yrs.
Methods
We recorded the right common carotid arterial Doppler flow velocity (BFV) pattern and measured the peak velocities of the percussion wave (P) and late rising tidal wave (T), the ratio of the two (P/T), the time interval between the two peaks corrected by heart rate (P-Tc), systolic flow velocity integral (FVI) and carotid artery diameter (CAD) before and after 0.4 mg dose of subligual nitroglycerin (NTG).
Results
1) In hypertensives, the P wave velocity showed lower and P-Tc interval shorter than those of the normal controls at baseline. 2) After NTG, the P-Tc and P/T increased, but the T and FVI decreased significantly in both groups of subjects. 3) The P/T ratio was less significantly increased after NTG in the hypertensives than in the controls. These results suggest that NTG might have been involved in concomitant reduction and delay of the wave reflection from the peripheral vessels, preferentially in the normal subjects than in hypertensives.
Concluson
The carotid Doppler echography can be useful for the evaluation of the changes of hemodynamics in the peripheral vessel such as carotid artery in hypertensive subjects.
INTRODUCTION
At present, there have been few reports concerning the application of Doppler echography for the evaluation of both anatomical and functional abnormalities in the carotid artery1–10). Although there were a few papers on the evaluation of peripheral vascular hemodynamics by Doppler echography, no reports of defining and analyzing the systolic flow velocity profile were found. The purpose of the present study is to evaluate the changes in carotid arterial Doppler flow velocity pattern before and after sublingual nitroglycerin, as well as to evaluate its applicability for the assessment of peripheral hemodynamics in patients with hypertension.
SUBJECTS AND METHODS
In 28 hypertensive subjects (17 males, 11 females), who discontinued antihypertensive medication for more than 48 hours or were without medication until examination, and 40 normal control subjects (24 males, 16 females), two-dimensional (2-D) and color coded pulse Doppler echogram were obtained with Aloka’s model 870 (5 MHz phased array transducer with silicon rubber attach) from the right common carotid artery in the supine position of the subjects at baseline and every two minutes after sublingual nitroglycerin (NTG) of 0.4 mg for 10 minutes. The brachial arterial systolic and diastolic blood pressure were measured with an automatic sphygmomanometer simultaneously at every two minutes during the study. All recordings were stored on the videotape and pulsed Doppler echogram of the carotid artery was recorded with the paper speed of 100 mm/sec. We analysed the changes of the Doppler flow velocity profile and measured the peak velocities of the initial percussion wave(P), late rising tidal wave(T), the ratio of the two peak velocities(P/T), the time interval between the two peaks corrected by R-R interval on ECG(P-Tc), which was calculated as measured PT multiplied by 1000 msec (RR interval at the heart rate of 60/min) then divided by measured R-R interval(msec), systolic flow velocity integral (FVI) and the diameter of the common carotid artery at systole(CAD). (Fig. 1). We also calculated the arbitrary indices of flow rate and resistance from the above Doppler measurement, ie. carotid blood flow(CBF, ml/min) = FVI (cm) × (CAD/2)2 × 3.14 × heart rate; carotid vascular resistance (CVR, mmHg. Min./ml) = mean blood pressure/CBF. We compared the values at baseline between hypertensives and normal controls and compared the changes of the mean values before and after sublingual nitroglycerin in each group using paired or non-paired two group t test.
A pulsed wave Doppler flow velocity pattern obtained from the right common carotid artery in the normal subject. AR=aceleration rate; DR=deceleration rate; P=peak velocity of early systolic percussion wave; T=peak velocity of systolic tidal wave; P-T=time interval between P and T; D=peak velocity of diastolic wave; ET=ejection time.
RESULTS
In the hypertensives, the P wave velocity showed lower, the P-Tc interval was shorter and the CVR was higher than those of the normal controls at baseline(67±22 cm/sec vs. 93 ± 25 cm/sec, 118 ± 18 msec, vs 146 ± 22 msec, and 0.38 mmHg min/ml vs 0.27 mmHg min/ml, respectively, all p<0.05). After sublingual NTG, both mean systolic and diastolic blood pressures decreased significantly (from 158/83 to 140/78 mmHg), similar to normal controls (from 113/65 to 106/60 mmHg), but heart rate showed increasing tendency in both groups of subjects, 93 to 73 beats/min in normal controls and 73 to 81 beat/min in hypertensives (Fig. 3). The P-Tc interval and the P/T ratio increased significantly (152 ± 19 msec vs 118 ± 18 cm/sec, p<0.01 and 1.8 ± 0.5 vs. 1.3 ± 0.3, p<0.05, respectively), the P velocity increased (73 ± 23 cm/sec vs 67 ± 22 cm/sec, p<0.05), but the T velocity and the FVI decreased significantly after NTG (43 cm/sec vs 53 cm/sec and 0.11 m vs 0.14 m, respectively, p<0.05) in comparison with the baseline values (Fig. 4,5,6). The CAD, CBF and CVR showed no significant changes after NTG(Table 1, Fig. 6). When comparing the variables between the hypertensives and the normal controls, we found the similar changes, those of decreased T velocities and increased P-Tc interval in the Doppler flow velocity pattern before and after NTG except FVI, which decreased significantly in hypertensives after NTG resulting in decrease of CBF.

Changes of the systolic (SBP), diastolic blood pressure (DBP) and heart rate (HR) after sublingual nitroglycerin (NTG) in controls and hypertensive subjects.

Changes of the carotid Doppler peak velocities of percussion (P), tidal (T) and diastolic wave (D) after sublingual nitroglycerin (NTG) in normal controls and hypertensive subjects.
Changes of the corrected PT intervals (PTc) and P/T ratio (P/T) after sublingual nitroglycerin (NTG) in controls and hypertensive subjects.
Changes of the carotid artery flow velocity integral (FVI) and diameter (CAD) after sublingual nitroglycerin (NTG) in controls and hypertensive subjects.
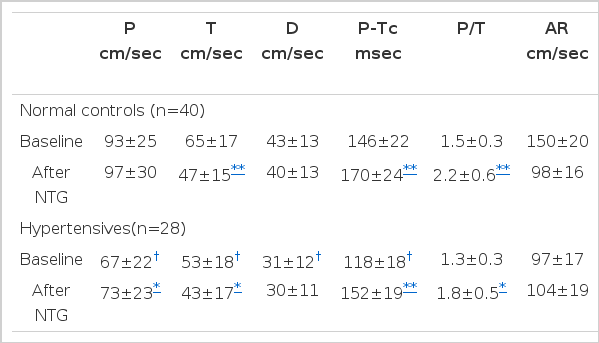
Carotid Doppler Echographic Parameters before and after Sublingual Nitroglycerin (NTG) in normal controls and Hypertensive subjects.
DISCUSSION
At present, many physicians have been interested in the pathophysiology of the hemodynamic changes of heart and the peripheral vessels in the hypertensive patients. Many studies have demonstrated that multiple factors, such as pulse wave velocity, wave reflection from periphery, aortic impedence and peripheral vascular resistances, as well as increased smooth muscle tone, are related to the vascular abnormalites in hypertensives. Since Levenson had first reported the utility of the pulsed Doppler system for brachial artery, several other studies were performed to evaluate peripheral vascular obstruction or carotid arterial hemodynamics1–11). But there were a few reports on the Doppler flow velocity pattern in the carotid artery. Prior to this study, we observed similar changes in shape and timing between Doppler flow velocity profile and carotid pulse tracing12)(Fig. 2). In this study, initial percussion flow velocity(P) of hypertensives at baseline showed smaller in amplitude than the normal control subjects. The finding was comparable to the studies of Yoshimura7,8) and Borthier13). In the former, the decrease in carotid flow velocity in elderly hypertrensive subjects might be resulted from increases of the carotid arterial wall stiffness and luminal diameter. In the latter, long acting nitrate might cause increase of carotid artery diameter but decrease of blood flow velocity. However, Doursout reported in his dog study that NTG produced the increase of carotid blood flow caused by either reflex increase of cardiac output or direct local vasodilation, and suggested that NTG has a decreasing effect on the carotid artery resistance14). The heart rate-corrected time interval between two peak flow waves (P-Tc) shortened and the ratio of the P to T increased in the hypertensives compared to those of the normals in this study. It might be resulted from the earlier wave reflection from the peripheral vessel causing late systolic increase of presssure wave on invasive measurment, which was compatible with the reports of O’Rourke and Kelly15–19). Kelly suggested that the causes of the increased carotid pulse amplitude in aged person were both increase of arterial stiffness and progessively earlier wave reflection, which can augment the systolic pressure in the ascending aorta and increase the left ventricular afterload. He reported that nitroglycerin dilates the peripheral artery, such as carotid artery, and decreases the wave reflection and ascending aortic systolic pressure, but sphygmomanometer could not detect the pressure decrease of ascending aorta after NTG. We observed no significant differences in carotid arterial diameter and carotid blood flow, but calculated carotid vascular resistance showed significant increase in the hypertensives compared to the normal controls at baseline. In this study, after sublingual nitroglycerin, an agent for decreasing the arterial stiffness, the P was increased, the T decreased, the P-Tc prolonged, the P/T increased in the hypertensives. These findings were considered to be resulted from apparent decrease in T wave, which might be influenced by decreased wave reflection from the peripheral vessel. Thus, we suggest that wave reflection itself is one of the important determinants of abnormal hemodynamics in the hypertensives and the carotid Doppler echography seems to be a simple non-invasive method, which can be used to assess, not only the changes of the peripheral vascular hemodynamics, but also the effects of hypotensive agents on peripheral vessels such as carotid artery after pharmacological treatment in hypertensive subjects.

An example of simultaneous recording of the right carotid pulse (CPT) with the left carotid artery Doppler flow velocity (CFV) in a normal subject.
LIMITATIONS
In this study, the mean age of the hypertensives was higher than the normal controls so that there were some limitations to compare the precise changes of the carotid Doppler flow velocity pattern between the two groups and, also, aging itself made some additive changes to hypertensive hemodynamics.