Dermatomyositis without Elevation of Creatine Kinase Presented as Bronchiolitis Obliterans Organizing Pneumonia
Article information
Abstract
A case of dermatomyositis presented as bronchiolitis obliterans organizing pneumonia has been rarely reported. We describe a 46-year-old female patient with dermatomyositis without elevation of creatine kinase presented as bronchiolitis obliterans organizing pneumonia. She was treated with prednisolone and azathioprine. Over a 2-year follow-up she has had no elevation of creatine kinase. The patient remains asymptomatic and has no medication for dermatomyositis and bronchiolitis obliterans organizing pneumonia two years after initial treatment. It has been suggested that the prognosis of dermatomyositis without creatine kinase elevation may be poor. Because the prognosis of bronchiolitis obliterans organizing pneumonia is generally believed to be good, we tentatively suggest that the normal value of creatine kinase in dermatomyositis does not always seem to herald a poor prognosis, an associated malignancy or severe interstitial lung disease.
INTRODUCTION
Polymyositis/dermatomyositis are inflammatory myopathies of unknown etiology that commonly are associated with the elevation of serum creatine kinase. However there is no elevation of creatine kinase in some patients despite muscle involvement1). Although it has been suggested that the normal value of creatine kinase in polymyositis/dermatomyositis seems to confer a poor prognosis, either an associated malignancy or severe interstitial lung disease, the significance of no elevated creatine kinase remains to be clarified.
Bronchiolitis obliterans organizing pneumonia is a clinicopathologic syndrome of pulmonary inflammatory responses which has become increasingly recognized and has been described in association with a variety of disorders2). Bronchiolitis obliterans organizing pneumonia has been reported in polymyositis/dermatomyositis, but polymyositis/dermatomyositis presented as bronchiolitis obliterans organizing pneumonia was rare3). We describe a case of dermatomyositis without elevation of creatine kinase presented as bronchiolitis obliterans organizing pneumonia.
CASE REPORT
A 46-year-old-female was admitted to Guro Hospital of Korea University because of a 10-day history of dry cough, dyspnea on exertion, skin eruptions of three months' duration and proximal muscle weakness of one month's duration. At admission, she appeared acutely ill and her blood pressure was 130/90 mmHg, pulse rate 80/min, respiratory rate 24/min and temperature 37.2°C. Physical examination showed violaceous erythema of the face, erythematous macules on bony prominences as interphalangeal joints (Gottron's papules), on the neck, chest and back(Figure 1) and proximal muscle weakness with normal distal muscle strength of all four extremities. Crackles were present at both lung bases. Chest radiography revealed opacities in both lower lungs. The following tests were within normal limits; white blood cells (WBC), hemoglobin, liver enzymes, electrolytes, urinalysis, C-reactive protein, ASLO, rheumatoid factor, antinuclear antibodies, anti-Jo-1, ANCA, VDRL, cryoglobulin, HBsAg, HBsAb, anti-HCV. Creatine kinase was 180 IU/L (normal < 200), lactic dehydrogenase was 489 IU/L (normal <500), and aldolase was 3.2 IU/L (normal 2–8), but erythrocyte sedimentation rate was 47 mm/hour. Arterial blood gases showed pH 7.445, PaCO2 33.4 mmHg and PaCO2 70 mmHg. Pulmonary function test revealed forced vital capacity of 2.23 L(73%), forced expiratory volume in 1 second of 1.81 L(77%), FEV1/FVC of 81% and DLco of 15.9 mL/min/mmHg(81%). High resolution CT showed multifocal airspace consolidations in the subpleural location of both basal lungs(Figure 2), and bronchoalveolar lavage showed WBC of 7.2 × 106; macrophage of 60% (normal 85%), lymphocyte of 12% (normal 7–12%), neutrophil of 28% (normal 1–2%). Esophageal manometry showed negative results. Electromyographic examinations of arms and legs revealed features suggestive of myopathy; low amplitude, highly polyphasic motor unit potentials and biopsy of the right rectus femoris muscle showed negative' results. The skin biopsy of the forehead showed superficial perivascular lymphocytic infiltration, and thoracoscopic lung biopsy revealed the respiratory bronchiole and adjacent alveolar duct filled with fibroblastic plugs(Masson's body) and relatively spared interstitium(Figure 3). The findings represent bronchiolitis obliterans organizing pneumonia. A diagnosis of dermatomyositis without elevation of creatine kinase presented as bronchiolitis obliterans organizing pneumonia was made based on clinical and histologic evidence. The patient was given 50 mg of prednisolone daily with resolution of muscle weakness, dyspnea and skin lesions. Six months later, the prednisolone dose was tapered to 12.5 mg daily and oral azathioprine 100 mg daily was added as a steroid sparing agent. Both prednisolone and azathioprine were gradually tapered and over a 2-year follow-up, she has had no elevation of creatine kinase(Table 1). She remains asymptomatic and has no medication for dermatomyositis and bronchiolitis obliterans organizing pneumonia two years after the initial treatment.

Gottron’s papules of the patient

High resolution CT showed multifocal airspace consolidations in subpleural location of both basal lungs.

Lung biopsy revealed the respiratory bronchiole and adjacent alveolar duct filled with fibroblastic plugs (Masson’s body) and relatively spared interstitium (Masson-Trichrome, x100).
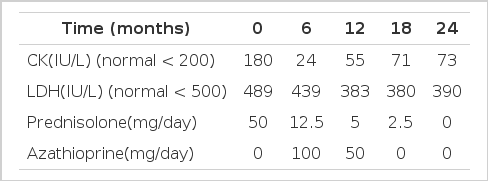
Clinical course of the patient.
DISCUSSION
Creatine kinase is the muscle enzyme most widely used to diagnose polymyositis/dermatomyositis and to follow therapeutic response. In general, patients with polymyositis/dermatomyositis have an increased creatine kinase, but it has been reported that some patients with polymyositis/dermatomyositis have not an elevated creatine kinase1,4,5). Serum inhibitor of creatine kinase or long standing disease with severe muscle atrophy has been proposed for the alleged association between the low level of creatine kinase and poor prognosis, and the significance and mechanism of normal creatine kinase level in polymyositis/dermatomyositis are yet unknown. Previous studies have suggested that the absence of creatine kinase elevation in polymyositis/dermatomyositis might signify a poor prognosis, an associated malignancy or severe interstitial lung disease5,6). However several studies have been unable to demonstrate that normal creatine kinase values herald a poor prognosis in polymyositis and dermatomyositis7–9).
Bronchiolitis obliterans organizing pneumonia has been reported in polymyositis/dermatomyositis, but a case of polymyositis/dermatomyositis presented as bronchiolitis obliterans organizing pneumonia has been rarely reported. In this case, the patient was diagnosed as dermatomyositis without elevation of creatine kinase presented as bronchiolitis obliterans organizing pneumonia. The patient had skin lesions of dermatomyositis and muscle weakness but no laboratory evidence suggestive of myopathy, except electromyographic findings. Although dermatomyositis without elevation of creatine kinase is not always the same an amyopathic dermatomyositis6), this case can be also considered as amyopathic dermatomyositis which refers to a condition that has a typical rash in which the typical cutaneous manifestations of dermatomyositis is present, but muscle disease is lacking, mild or transient(Figure 4)4). Amyopathic dermatomyositis is reported to represent 11%(6 of 54) of patients with dermatomyositis4) and can be divided into three types: Type 1 represents pure amyopathic dermatomyositis patients who have only skin disease. Type 2 are patients with skin disease who have subjective myalgia and weakness but no laboratory evidence of muscle disease. Type 3 are patients with no muscle weakness clinically but who have evidence of abnormal laboratory tests. Studies for clear classification between amyopathic dermatomyositis and dermatomyositis without elevation of CK are needed.

The prognosis of dermatomyositis without elevation of creatine kinase remains unclear when compared to that of dermatomyositis with elevation of creatine kinase. In this case, bronchiolitis obliterans organizing pneumonia as interstitial lung disease has been developed, but the patient's response to therapy has not been bad over a 2-year follow-up period. Because the prognosis of bronchiolitis obliterans organizing pneumonia is generally believed to be good, we tentatively suggest that the normal value of creatine kinase in dermatomyositis does not always seem to herald a poor prognosis, an associated malignancy or severe interstitial lung disease.