Impact of guideline-directed medical therapy on the cardiac or non-cardiac death in acute myocardial infarction
Article information
 , Dahee Hyun2, Seung Ho Hur3, Seung Woon Rha4, Seung Jae Joo5, Hyo-Soo Kim6, Myung Ho Jeong7, on behalf of KAMIR-NIH investigators
, Dahee Hyun2, Seung Ho Hur3, Seung Woon Rha4, Seung Jae Joo5, Hyo-Soo Kim6, Myung Ho Jeong7, on behalf of KAMIR-NIH investigatorsAbstract
Background/Aims
While the clinical effectiveness of guideline-directed medical therapy (GDMT) is well established in patients with acute myocardial infarction (AMI), its specific impact on cause-specific mortality remains unclear. This study aimed to investigate the impact of GDMT on both cardiac and non-cardiac mortality in AMI patients.
Methods
Data of the KAMIR-NIH, a multicenter prospective registry of AMI in Korea between 2011 and 2015, were included. The competing risks of cardiac and non-cardiac death in patients who received GDMT were compared with those who did not, using a multivariable-adjusted cumulative incidence analysis of propensity score-matched patients. Primary endpoint of interest was 3-year cardiac and non-cardiac mortality.
Results
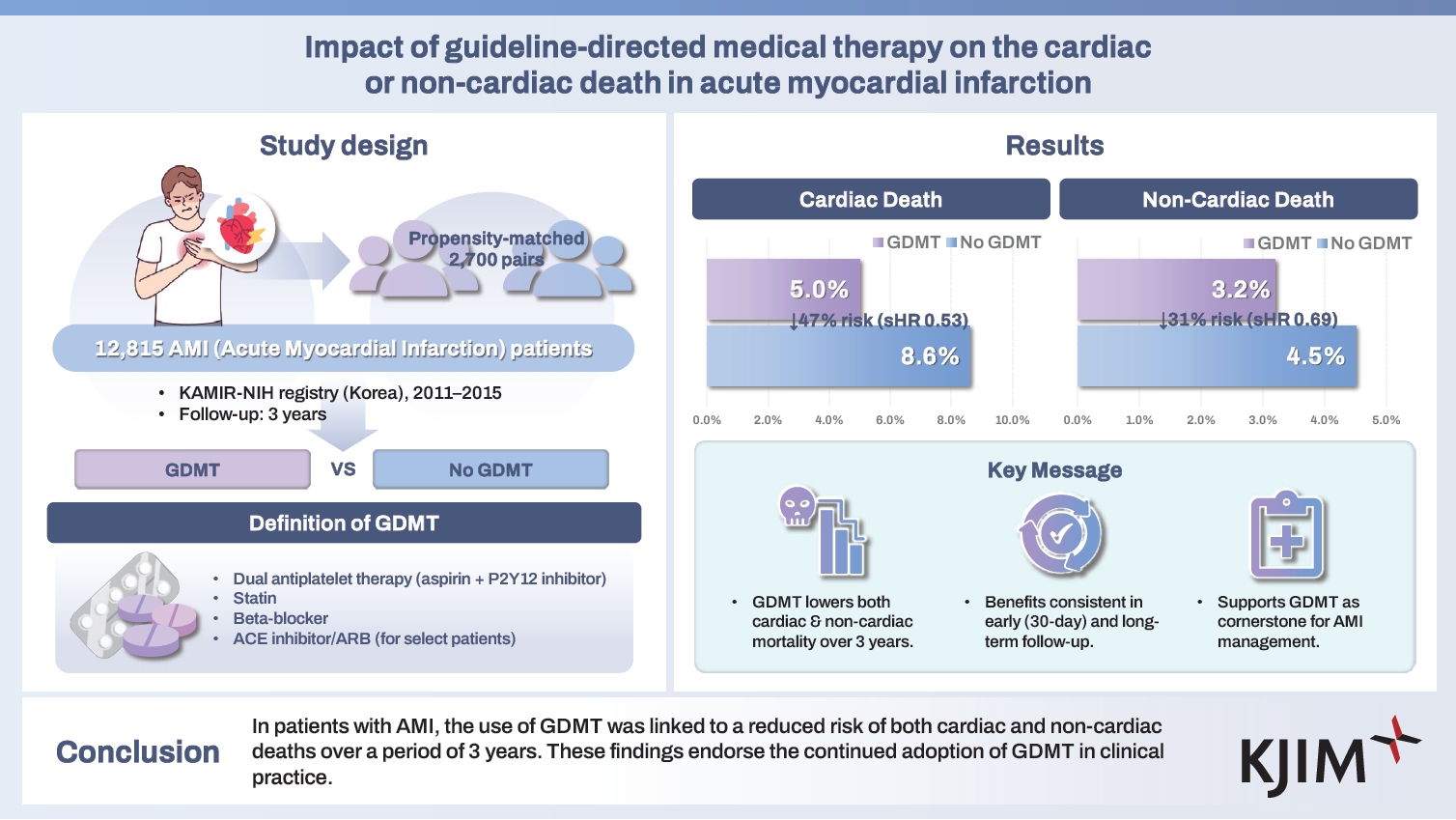
Of the 12,815 patients enrolled, 2,700 matched pairs with a mean age of 64.9 ± 12.2 years were analyzed. The cumulative incidence of cardiac death (5.0% vs. 8.6%; subdistribution hazard ratio [sHR] 0.53; 95% CI 0.43–0.67) and non-cardiac death (3.2% vs. 4.5%; sHR 0.69; 95% CI 0.52–0.92) was significantly lower in patients receiving GDMT compared to those who did not (all p < 0.05). These results were also consistent in 30-day landmark analyses.
Conclusions
In patients with AMI, the use of GDMT was linked to a reduced risk of both cardiac and non-cardiac death over a period of 3 years. These findings support the continued adoption of GDMT in clinical practice.
INTRODUCTION
Mortality following acute myocardial infarction (AMI) can result from either cardiac or non-cardiac causes. The incidence of early mortality, predominantly due to cardiac-related death, has seen a significant decline, which is largely attributed to the advancements in percutaneous coronary intervention (PCI) techniques, introduction of new devices, and the widespread adoption of guideline-recommended treatments including early reperfusion therapy and adjunctive pharmacotherapy [1,2].
Following the peri-infarct period, the likelihood of cardiac death decreases, while the proportion of non-cardiac death increases [3,4]. Evidence-based clinical guidelines strongly advocate the continuous use of guideline-directed medical therapy (GDMT) as a crucial measure for the secondary prevention of cardiovascular events or mortality for AMI patients [5,6]. Given the competing risks posed by cardiac or non-cardiac death, it is imperative to comprehensively assess the effects of GDMT on both outcomes, but it has been insufficiently understood [7]. We investigated the 3-year risk of cardiac or non-cardiac death among AMI patients and explored its association with the utilization of GDMT.
METHODS
Ethical statement
The study protocol followed the 2013 Declaration of Helsinki and was approved by the ethics committees of each participating center and the Institutional Review Board (IRB) of Samsung Medical Center (IRB No. 2022-06-147-004). Informed consent was waived due to the retrospective design.
Study patients
KAMIR-NIH registry is a nationwide, all-comer, multicenter, prospective registry that enrolled patients with AMI from 20 tertiary hospitals eligible for PCI in Korea between year 2011 and 2015. Clinical follow-up was conducted for up to 3 years after the index PCI.
Data definitions and endpoints
A detailed description of study variables has been previously reported [8]. In brief, GDMT included four main medication categories. Dual antiplatelet therapy with aspirin and a P2Y12 inhibitor, statins, and beta-blockers were mandatory. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers were recommended for patients with specific conditions, including left ventricular ejection fraction < 40%, hypertension, diabetes, or chronic kidney disease. Experienced research professionals at each participating institution evaluated GDMT usage and classified death as cardiac or non-cardiac death through an adjudication process. The primary outcome was the cumulative incidence of both cardiac and non-cardiac death.
Statistical analysis
Categorical variables are presented as frequencies and percentages, while continuous variables are expressed as means ± standard deviation (SD). Comparisons were made using relevant chi-squared or t-tests.
The association between GDMT and cardiac or non-cardiac death was assessed in three steps. First, baseline differences in clinical characteristics between patients who did and did not receive GDMT were addressed using propensity score matching to minimize imbalance. Covariate balance was confirmed by standardized mean differences < 0.10.
Second, as cardiac death and non-cardiac death are mutually exclusive competing events, an intervention that decreases the risk of cardiac death can increase the risk of non-cardiac death. When competing events are present, cause-specific hazards using Kaplan–Meier or Cox proportional hazards analyses may not precisely reflect the actual risk [9,10]. Therefore, Fine-Gray subdistribution hazard model was used to accurately assess cumulative incidence. Multivariable-adjusted cumulative incidence functions were compared using Gray’s test, and results are shown as hazard ratios with 95% confidence intervals (CI) [11,12]. Relative risk is shown with subdistribution hazard ratios (sHR) and 95% CI. Restricted mean time lost (RMTL) was additionally calculated to complement the hazard models by assessing the absolute benefit and effect sizes [13].
Finally, a 30-day landmark analysis was conducted to assess time-varying effects of GDMT, as mortality is typically highest in the early phase post-infarct.
All models were adjusted for patients' clinical characteristics using multivariable analysis, unless specified otherwise. Subgroup analyses that stratified patients by specific clinical characteristics were also performed. All statistical analyses were performed using R version 4.4 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Study flow and baseline clinical characteristics
Of the 13,104 patients initially enrolled in the KAMIR-NIH registry, 289 were excluded due to incomplete clinical data or timestamps, leaving a total of 12,815 patients for analysis (Fig. 1). At discharge, 70.2% of patients received GDMT. GDMT was more commonly prescribed to younger male patients, those with ST-elevation MI, left main or left anterior descending artery disease, radial access, or complete revascularization. In contrast, patients with comorbidities such as hypertension, diabetes, a prior MI, atrial fibrillation, or left ventricular ejection fraction < 40% were less likely to receive GDMT. These imbalances were addressed and balanced through propensity score matching (Table 1, Supplementary Fig. 1).

Study flow. The 3-year clinical outcomes of patients receiving GDMT were compared with those not on GDMT. A propensity score-matched cohort of 2,700 pairs of patients was included in the analysis. AMI, acute myocardial infarction; GDMT, guideline-directed medical therapy.

Baseline characteristics of patients with GDMT and those without GDMT
Risk of cardiac or non-cardiac death in patients with GDMT versus those without GDMT
In the analysis of the entire cohort, there were 1,398 documented deaths: 923 attributed to cardiac causes and 475 to non-cardiac causes over the 3-year follow-up. Overall, the unadjusted 3-year cumulative incidence of cardiac death was higher than that of non-cardiac death (7.5%, 95% CI 7.0–7.9% vs. 3.9%, 95% CI 3.6–4.3%, p < 0.001) (Fig. 2).

Unadjusted cumulative incidence rates of all-cause, cardiac, and non-cardiac deaths. In the analysis of all patients, the unadjusted 3-year cumulative incidence of all-cause, cardiac, and non-cardiac deaths were 11.4% (95% CI 10.8–11.9%), 7.5% (95% CI 7.0–7.9%), and 3.9% (95% CI 3.6–4.3%), respectively. The difference between cardiac death and non-cardiac death was statistically significant (p < 0.001). CI, confidence intervals.
Patients receiving GDMT had a lower risks of both cardiac death (cumulative incidence: 5.6%, 95% CI 5.2–6.1% vs. 10.2%, 95% CI 9.5–11.0%; sHR: 0.50, 95% CI 0.43–0.57; RMTL difference: 37.8 days, 95% CI 30.0–45.6 days; all p < 0.001) and non-cardiac death (cumulative incidence: 3.5%, 95% CI 3.1–4.0% vs. 4.5%, 95% CI 3.9–5.2%; sHR: 0.77, 95% CI 0.63–0.94; RMTL difference: 6.9 days, 95% CI 0.9–12.8 days; all p < 0.05) compared to those without GDMT (Fig. 3).

Adjusted cumulative incidence rates of cardiac death (A) and non-cardiac death (B) according to the use of GDMT. In the analysis of all patients, those receiving GDMT exhibited a lower risk of both cardiac death and non-cardiac death compared to those without GDMT. Subdistribution hazard ratios (sHR) with 95% confidence intervals (CI) between the two groups and multivariable-adjusted cumulative incidences of each group are shown. Detailed numerical results are listed in Table 3. GDMT, guideline-directed medical therapy.
In the analysis of propensity score-matched cohort, patients receiving GDMT again showed a lower risk of both cardiac death (cumulative incidence: 5.0%, 95% CI 4.3–6.0% vs. 8.6%, 95% CI 7.7–9.7%; sHR: 0.53, 95% CI 0.43–0.67; RMTL difference: 28.5 days, 95% CI 17.3–39.7 days; all p < 0.001) and non-cardiac death (cumulative incidence: 3.2%, 95% CI 2.5–3.9% vs. 4.5%, 95% CI 3.8–5.2%; sHR: 0.69, 95% CI 0.52–0.92; RMTL difference: 8.9 days, 95% CI 1.6–16.2 days; all p < 0.05) (Fig. 4A, B). The 30-day landmark analysis of the propensity score-matched cohort also showed a lower risk of both cardiac death (cumulative incidence: 4.4%, 95% CI 3.5–5.1% vs. 5.7%, 95% CI 4.9–6.6%; sHR: 0.75, 95% CI 0.58–0.97; RMTL difference: 8.6 days, 95% CI 0.5–16.7 days; all p < 0.05) and non-cardiac death (cumulative incidence: 3.0%, 95% CI 2.3–3.6% vs. 4.3%, 95% CI 3.5–5.2%; sHR: 0.70, 95% CI 0.52–0.93; RMTL difference: 8.0 days, 95% CI 0.7–15.3 days; all p < 0.05) in patients with GDMT (Fig. 4C, D). Detailed clinical outcomes and statistical results are shown in Table 2 and 3.

Propensity score-matched adjusted cumulative incidence of cardiac death and non-cardiac death according to the use of GDMT. In the analysis of propensity score-matched patients, those receiving GDMT again exhibited a lower risk of both cardiac death and non-cardiac death compared to those without GDMT (A, B). The results of a 30-day landmark analysis were consistent with these findings (C, D). Detailed outcomes are listed in Table 3. GDMT, guideline-directed medical therapy; sHR, subdistribution hazard ratios; CI, confidence intervals.

Three-year clinical outcomes

Risk of cardiac or non-cardiac death of patients with GDMT compared to those without GDMT
In the exploratory subgroup analysis, the results for all patients (Supplementary Fig. 2A, B) and the propensity score-matched patients (Supplementary Fig. 2C, D) were largely consistent with the primary analysis. In the 30-day landmark analysis of the propensity score-matched patients, the overall benefit of GDMT appeared to diminish, showing heterogeneity among subgroups (Supplementary Fig. 2E, F).
The key findings of the study results are summarized in the Central Illustration.
DISCUSSION
This study investigated the 3-year outcomes of a nationwide AMI registry and revealed that the use of GDMT was associated with a reduced risk of both cardiac and non-cardiac death.
In addition to the association of GDMT with a lower risk of cardiac death, its correlation with a reduced risk of non-cardiac death warrants discussion. A recent analysis of ISCHEMIA trial reported lower medication adherence among patients with poor health status [14]. Patients without GDMT may face disadvantages such as unfavorable clinical conditions, drug intolerance, or major non-cardiovascular illness, which could hinder their ability to adopt GDMT. GDMT may enhance cardiovascular health and potentially reduce the risk of non-cardiac death through various mechanisms, including decreased thromboembolism in patients at risk of peripheral artery occlusive disease or stroke, protection or slowing of disease progression in those with chronic kidney disease, or mitigation of cardiotoxicities from anticancer drugs in patients undergoing chemotherapy [15-17]. These hypotheses require validation through in-depth investigations that incorporate comprehensive clinical data.
The rate of cardiac death declines over time, with non-cardiac causes becoming the predominant cause of later death following AMI [18]. In this study, the unadjusted 3-year cumulative incidence of cardiac death (7.5%) remained higher than that of non-cardiac death (3.9%). Since the risk of non-cardiac death is known to catch up with that of cardiac death approximately 6 to 7 years later, additional long-term studies are required to investigate the ongoing risks of both cardiac and non-cardiac death in this population [4,19].
This study utilized competing risk analysis and demonstrated that GDMT, primarily targeting cardiovascular disease, appears to reduce non-cardiovascular mortality as well. These findings highlight the potential importance of continued long-term use of GDMT following AMI. As subgroup analyses showed heterogeneity in the association between GDMT and clinical outcomes especially regarding non-cardiac death, the implementation of long-term GDMT may need to be individualized rather than universally applied for AMI patients.
Limitations
The major limitation of our study was its observational design, which restricts the ability to establish robust causal relationships. This study did not capture detailed information regarding medication adherence as proposed by the Non-Adherence Academic Research Consortium [20]. Details of interventional procedure were not included, albeit the majority of cardiac death is known to be unrelated to them [18]. The causes of non-cardiac deaths and systematic data on non-cardiac comorbidities, such as extent of cancer, functional status, socioeconomical status, and the Charlson Comorbidity Index, were not reported. Statistical adjustment through propensity score does not guarantee the absence of residual confounding bias. Considering the declining mortality associated with AMI in recent decades, it is crucial to interpret our findings in the context of the ongoing advancements in healthcare technologies [21].
In this real-world AMI registry, GDMT was associated with a lower risk of both cardiac and non-cardiac death over a 3-year period. These findings provide further evidence of the clinical benefits of GDMT, emphasizing its importance as a cornerstone of the long-term management for AMI.
KEY MESSAGE
1. Propensity score-matched 2,700 matched pairs of AMI patients (mean age 64.9 years) derived from the KAMIR-NIH registry (2011–2015) were evaluated for 3 years.
2. Both cardiac death (5.0% vs. 8.6%; subdistribution hazard ratio [sHR] 0.53) and non-cardiac death (3.2% vs. 4.5%; sHR 0.69) were significantly lower in GDMT recipients than in non-recipients.
3. The utilization of GDMT was associated with both cardiac and non-cardiac mortality, supporting its continued use in AMI management.
Notes
CRedit authorship contributions
Jin-Ho Choi: conceptualization, methodology, investigation, formal analysis, software, writing - original draft, writing - review & editing, visualization; Dahee Hyun: conceptualization, methodology, investigation, formal analysis, software, writing - original draft, writing - review & editing, visualization; Seung Ho Hur: conceptualization, methodology, investigation, writing - original draft, writing - review & editing; Seung Woon Rha: conceptualization, validation, writing - original draft, writing - review & editing, supervision; Seung Jae Joo: conceptualization, writing - original draft, project administration; Hyo-Soo Kim: conceptualization, validation, writing - original draft, supervision; Myung Ho Jeong: writing - original draft, supervision, project administration
Conflicts of interest
The authors disclose no conflicts.
Funding
This study was supported by the National Institute of Health Research Project, No. 2016-ER6304-02.