


INTRODUCTION
Pulmonary adenomas usually include several diverse histological types such as bronchial adenoma, alveolar adenoma, papillary adenoma and adenomas of the salivary gland1, 2). Among these tumors, primary pulmonary pleomorphic adenoma is a neoplasm that shows some features of salivary gland-type pulmonary adenoma and also the pleomorphic histological appearance of several types of tumor tissues. This tumor is exceedingly rare, with less than 15 cases having been reported in the literature and they have predominately occurred in the proximal airway3). To the best of our knowledge, only a few cases of primary pleomorphic adenoma in the lung periphery have been reported. Herein, we report on this unusual case of radiographically and pathologically proven primary pulmonary pleomorphic adenoma.
CASE REPORT
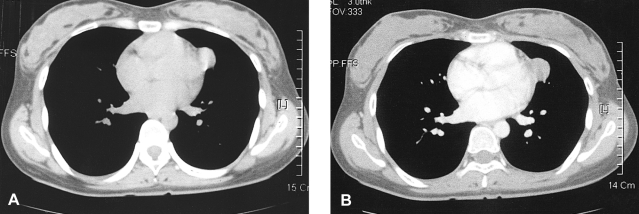
A 25-year old woman was referred to our hospital for evaluation of an abnormal chest radiograph. There was no prior family history of respiratory or salivary problems and she had no respiratory or salivary gland symptoms. The laboratory studies, including the peripheral blood counts and biochemical examinations, showed no abnormalities. The tumor markers were found to be within the normal ranges. The results of the pulmonary function tests and bronchoscopic examination were all normal. A chest radiograph showed the presence of a solitary pulmonary nodule that blunted the left cardiac border in the left lung field. A non-enhanced CT scan revealed the existence of a 2.5 ├Ś 2 cm, mild cystic mass abutting the mediastinum, which had the appearance of a pericardial or dermoid cyst (Figure 1A). Contrast-enhanced CT scans showed a mildly enhancing nodule with a well defined margin; this had the appearance of a fried egg (Figure 1B).
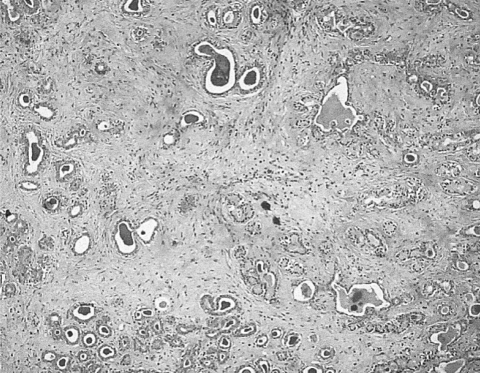
The radiographic findings were suggestive of a benign process, so video-assisted thoracoscopic surgery was performed for the histological confirmation. On the gross pathology, the left lingular segment contained a well-demarcated solid mass that was light gray in color and 2.4├Ś2.8├Ś2.8 cm in size, and nodular appearance was observed on the cut surface. The light microscopic findings revealed that the nodule was a well circumscribed and encapsulated lesion. There were no visible bronchi connected to the tumor, and the tumor principally consisted of nodules formed from strands of several types of tumor cells with a hyalinized cartilaginous stroma (Figure 2).
DISCUSSION
Pleomorphic adenoma is also named mixed tumor, and this is the most common neoplasm of the salivary glands; it usually develops in the palate, tongue, nasopharynx or larynx. It can also occur as a type of pulmonary adenoma and especially in association with the bronchial glands4-7). However, pleomorphic adenoma of the lung is very rare, so that its incidence and etiology are unknown; there is no obvious sex predominance. This tumor is thought to constitute about 1% of all the cases of primary lung adenoma8).
The histological appearance of primary pulmonary pleomorphic adenoma is produced by a mixture of luminal-type ductal epithelial cells, myoepithelial tissues and tissues that have a myxochondroid, mucoid or chondroid appearance9, 10). Further, these tumors are typically well-circumscribed. Although the radiological findings are not well known, this tumor is thought to have a preference for a solitary, peripheral or subpleural location and to have a smooth margin. This tumor is slow growing and it occasionally has malignant potential5, 6).
In our case, it was very difficult to differentiate between a peripheral lung mass and a mediastinal mass on the radiographs because the tumor was located in the peripheral lung near the mediastinal pleura and it had the appearance of a fried egg. The contrast-enhanced CT scans showed a mildly enhancing nodule with a well defined margin; the appearance was similar to that of a benign mediastinal nodule. For a case like this, pathologic confirmation should be performed when abnormal radiographic findings are detected. However, several diverse possibilities for the differential diagnosis, including pulmonary pleomorphic adenoma, should be considered before conducting invasive diagnostic procedure.
In conclusion, we report here on a rare case of a primary pleomorphic adenoma that mimicked a mediastinal mass located in the lung periphery.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





