


To the Editor,
Scrub typhus is an acute febrile illness caused by Orientia tsutsugamushi, which is found over a wide area of eastern Asia and the western Pacific regions. The gold standard test for the serologic diagnosis of scrub typhus is the indirect immunofluorescence assay (IFA). However, while sensitive, the IFA is expensive and requires considerable training. Moreover, the IFA results are delayed several days in most clinics and hospitals in Korea because the tests are performed in external commercial laboratories rather than in in-house facilities. Therefore, alternative diagnostic methods are needed. In the past two decades, the passive hemagglutination assay (PHA) has been used widely for this purpose, but it has a lower sensitivity, especially during the acute phase of the infection [1,2].
Recently, the immunochromatographic test (ICT) to detect antibodies against O. tsutsugamushi was introduced as a rapid diagnostic test to replace the PHA in Korea. Commercially available ICT kits have been evaluated for early rapid diagnosis at the time of hospital admission of febrile patients in Southeast Asia [3,4]. To our knowledge, the performance of the ICT has not been evaluated in Korea where the predominant genotype of O. tsutsugamushi differs from that found in other geographical areas. To evaluate the diagnostic utility of the ICT in Korea, we assessed the diagnostic sensitivity of the ICT for early rapid diagnosis of scrub typhus in Korean patients.
This study included patients with IFA-confirmed scrub typhus who underwent the ICT at the time of hospital admission/visit from September to November 2012 at five hospitals in Korea. IFA tests were performed at the Green Cross Reference Laboratory (Yongin, Korea) to detect IgG, IgM, and IgA antibodies against the standard O. tsutsugamushi antigens from the Gilliam, Karp and Boryong strains. A four-fold rise in IFA titer or a single titer Ōēź 1:160 was determined as the diagnostic criterion for scrub typhus [2]. The ICT was performed in the microbiology laboratory at each hospital using commercial kits (SD Bioline Tsutsugamushi Assay, Standard Diagnostics, Yongin, Korea). This test employed the 56-kDa major surface protein antigens from representative O. tsutsugamushi including Gilliam, Karp, and Kato strains to detect IgG, IgM, and IgA antibodies to O. tsutsugamushi. Baseline testing was performed using blood samples collected on the same calendar day. Our study was approved by the Institutional Review Board at each hospital.
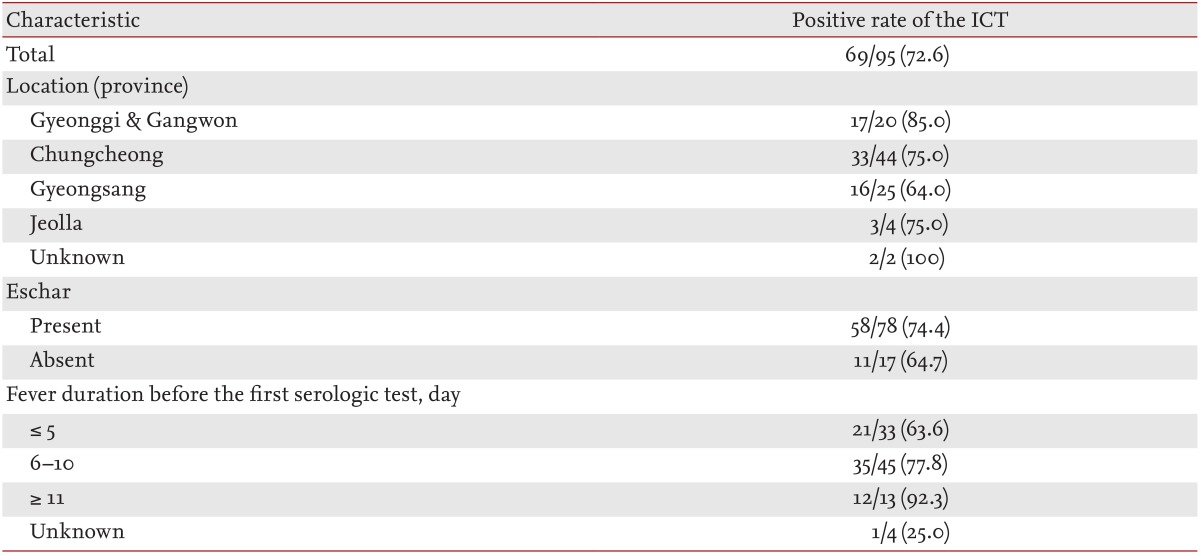
A total of 273 patients with suspicion of scrub typhus were seen during the study period. Of these, 96 patients had IFA-confirmed scrub typhus; 95 of these underwent an ICT and were enrolled in the study. The median age of the participants was 64 years (interquartile range [IQR], 55 to 73), and 50 patients (52.6%) were female. Of the 95 participants, 78 (82.1%) had eschar. The median fever duration before the first serologic test was 7 days (IQR, 5 to 9). The overall sensitivity of the ICT was 72.6% (Table 1). The positive rate of the ICT increased with the fever duration before the first serologic testing.
Previous studies evaluating the diagnostic accuracies of different ICTs found that the sensitivities and specificities ranged from 46.3% to 67.9% and 67.9% to 95.1%, respectively, depending on the assay kit [3]. These earlier studies were conducted in Thailand where the Gilliam and Karp strains dominate; using the SD Bioline assay kit, the sensitivity and specificity were 66.7% and 98.4%, respectively [4]. In contrast, the SD Bioline test in our study showed slightly higher sensitivity (72.6%) in Korea where the Boryong strain dominates. The package insert of the SD Bioline test displays high positive results with a sensitivity of 99% and specificity of 96% in Korean patients. The discrepancy in the sensitivities of this SD Bioline test between Southeast Asia and Korea cannot be explained by the different distribution of epidemic strains because the SD Bioline test uses Gilliam, Karp, and Kato antigens. The results of this study showed that the SD Bioline test might be more sensitive than the PHA. Previous studies reported that the detection rates of PHA at the acute stage of illness were as low as 41.5% to 54.3% [1].
The results of this study showed that fever duration before the first serologic testing can affect the ICT results. Other studies using the ICT also demonstrated a low sensitivity at the time of admission, but showed a trend of gradual increase in positivity [3,5]. Therefore, when interpreting the ICT results, clinicians should exercise caution because a substantial number of patients with confirmed scrub typhus were negative for this test, particularly in the early days of illness, as with PHA [1,2].
Our study has several limitations. First, a selection bias might have been present since not all patients seen during the study period received both IFA and ICT. Second, we did not confirm the serotype or genotype of the etiologic organisms, and it is possible that the sensitivities of the serologic tests might vary with the type. Third, we could not determine the specificity and positive or negative predictive values because we did not investigate the incidence of the disease. Lastly, interobserver and intraobserver variability might have been introduced in the interpretation of these tests, which were not performed simultaneously at the same laboratory.
Nevertheless, we found that the ICT had moderate sensitivity in Korean patients with scrub typhus, but it might have limited utility at the time of an initial visit. Additional studies to assess the accuracy of the ICT in Korea are required for proper use.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





