Reference diameter and characteristics of the distal radial artery based on ultrasonographic assessment
Article information

Abstract
Background/Aims
While distal radial artery (DRA) access is increasingly being used for diagnostic coronary angiography, limited information is available regarding DRA size. We aimed to determine the DRA reference diameters of Korean patients and identify the predictors of DRA diameter < 2.3 mm.
Methods
The outer bilateral DRA diameters were assessed using a linear ultrasound probe in 1,162 consecutive patients who underwent transthoracic echocardiography. The DRA diameter was measured by the perpendicular angle in the dorsum of the hand, and the average values were compared by sex. DRA diameter < 2.3 mm was defined as unsuitable for routine diagnostic coronary angiography using a 5 Fr introducer sheath.
Results
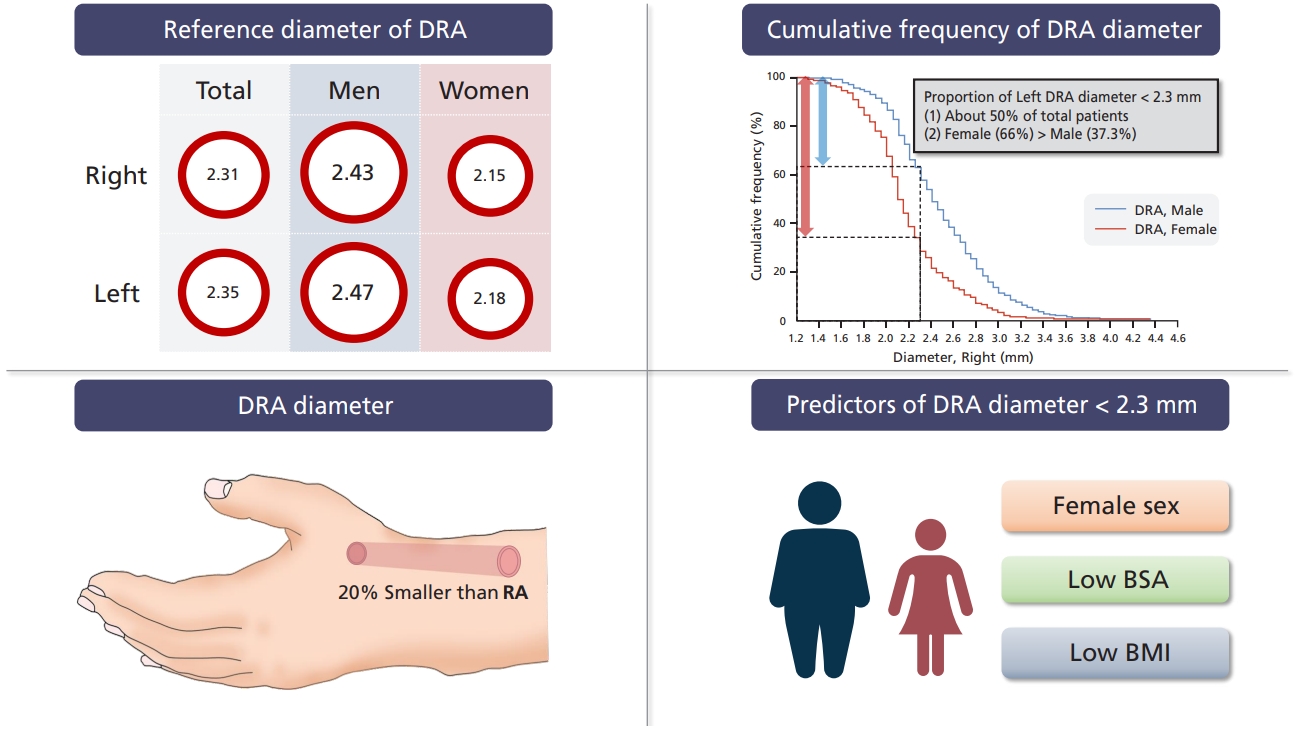
The mean DRA diameters were 2.31 ± 0.43 mm (right) and 2.35 ± 0.45 mm (left). The DRA was smaller in women than men (right: 2.15 ± 0.38 mm vs. 2.43 ± 0.44 mm, p < 0.001; left: 2.18 ± 0.39 mm vs. 2.47 ± 0.45 mm, p < 0.001). The DRA diameter was approximately 20% smaller than the radial artery diameter. A total of 630 (54.2%) and 574 (49.4%) patients had DRA diameter < 2.3 mm in the right and left hands, respectively. Female sex, low body mass index (BMI), and low body surface area (BSA) were significant predictors of DRA diameter < 2.3 mm.
Conclusions
We provided reference DRA diameters for Korean patients. Approximately 50% of the studied patients had DRA diameter < 2.3 mm. Female sex, low BMI, and low BSA remained significant predictors of DRA diameter < 2.3 mm.
INTRODUCTION
Radial access is recommended as the standard approach for coronary angiography (CAG) and percutaneous coronary intervention (PCI) based on the evidence that it is associated with reduced mortality and bleeding events compared to femoral access [1-3]. The use of distal radial access has recently increased owing to the publication of several studies that reported easy hemostasis, decreased bleeding, and low arterial occlusion rates with its use [4-6]. However, the distal radial artery (DRA) diameter is smaller than the radial artery (RA) diameter, which may limit its widespread use [5]. There is a lack of information regarding DRA diameter, which may complicate the identification of suitable patients in whom distal radial access may be adopted. This study aimed to determine the DRA reference diameter using ultrasonography in Korean patients. We also evaluated the clinical factors predictive of a DRA diameter < 2.3 mm.
METHODS
Study population
This was a retrospective observational study (DRAUS ClinicalTrials.gov identifier: NCT04303923). Between July 2017 and April 2018, 1,162 patients scheduled for transthoracic echocardiography were recruited in the echocardiography laboratory at a single center (Fig. 1). Cases with patients under 20 years of age, images of poor quality and difficult to interpret, and repeated measurements in the same patients were excluded. If a patient was scheduled for an invasive coronary procedure, that patient was moved to the catheterization laboratory after finishing the ultrasonographic evaluation in the echocardiography laboratory. Our local Institutional Review Board of Wonju Severance Christian Hospital approved the study protocol (CR318128) and waived the requirement for written informed consent due to the study’s retrospective nature.

Study flowchart.
Study endpoints
The primary endpoint was the mean DRA diameter of both hands. The secondary endpoints were the mean diameter of both RA, arterial diameter indexed according to body surface area (BSA), DRA/RA ratio, and proportion of patients with a DRA diameter < 2.3 mm. The reference diameter of 2.3 mm was derived from the average value (2.27 mm) of seven available radial introducer sheaths (Table 1). A DRA diameter < 2.3 mm was defined as unsuitable for routine diagnostic coronary angiography using a 5 Fr introducer sheath. BSA was calculated using the Mosteller formula as follows [7]:

Outer diameter of radial introducer sheaths
Assessment of arterial diameter by ultrasonography
The patients were asked to relax on a bed in a quiet room. The anatomical landmark for the DRA measurement was the dorsum of the hand in which the DRA was superficially located (Fig. 2). The RA diameter was measured as a distance of 2 to 3 cm above the wrist crease. The DRA and the cephalic vein were discriminated using color Doppler and vessel compression methods with an ultrasonographic probe. The round shape of the artery in the short-axis plane was determined by tilting of the probe. The outer diameters of the DRA and RA were assessed at a perpendicular angle, and the average values were recorded. The vessel diameters were measured twice by experienced sonographers and confirmed by a dedicated investigator using an 11L-D linear array ultrasound probe transducer (4.5 to 12.0 MHz bandwidth) with a Vivid E95 (GE Health Care, Milwaukee, WI, USA) or an L12-3 broadband linear array ultrasound probe transducer (3.0 to 12.0 MHz bandwidth) with a Philips EPIQ 7 (Philips Medical Systems, Andover, MA, USA). The intra-class correlation coefficients of intra- and interobserver variabilities in the arterial diameter measurements were 0.97 and 0.98.

Assessment of the distal radial artery diameter using ultrasonography. (A) Hand position for the assessment of the distal radial artery. (B) Ultrasonographic image showing the short-axis plane of the distal radial artery between first and second metacarpal bone. (C) Schematic illustration showing the relationship between the distal radial artery and extensor pollicis longus tendon.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and compared using the two-sample t test. Categorical variables were expressed as counts and percentages, and the statistical analyses were performed using the chi-square test. Simple and multiple logistic regression analyses were used to predict a DRA diameter < 2.3 mm. Model 1 was adjusted for body mass index (BMI) and other significant variables in a simple logistic regression analysis. Model 2 was adjusted for the same variables; however, BMI was replaced with BSA. Statistical significance was set at p < 0.05. The statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and MedCalc for Windows version 19.4.1 (MedCalc Software, Ostend, Belgium).
RESULTS
Baseline characteristics
Table 2 summarizes the baseline characteristics of the enrolled patients. The mean age was 65.1 ± 13.0 years, and 671 (57.7%) were male. The female patients were older and had a similar BMI but lower BSA than the male patients. The medical histories of hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease, coronary artery occlusive disease (CAOD), old cerebrovascular accident, peripheral arterial occlusive disease, and atrial fibrillation were similar between the two groups. There were no statistical differences in the history of CAG, PCI, or the use of radial access.

Baseline patient characteristics
DRA and RA diameters and characteristics
The mean DRA diameters were 2.31 ± 0.43 mm (total patients), 2.43 ± 0.44 mm (men), and 2.15 ± 0.38 mm (women) in the right hand and 2.35 ± 0.45 mm (total patients), 2.47 ± 0.45 mm (men), and 2.18 ± 0.39 mm (women) in the left hand (Table 3). The DRA and RA sizes were significantly smaller in women (Fig. 3). However, the DRA and RA diameters indexed by BSA were similar in men and women. The DRA/RA ratios were 0.81 ± 0.12 and 0.83 ± 0.12 in the right and left hands, respectively.
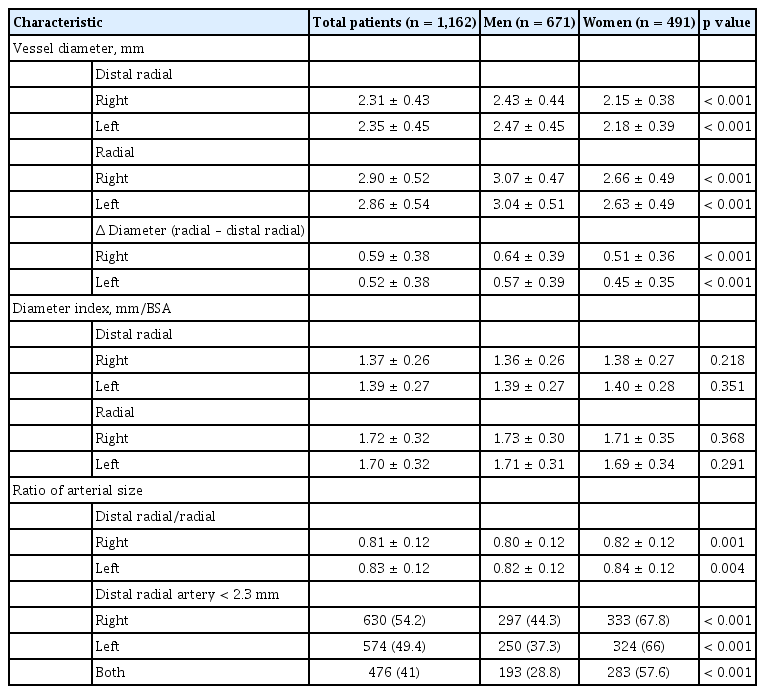
Diameters and characteristics of the distal radial and radial arteries
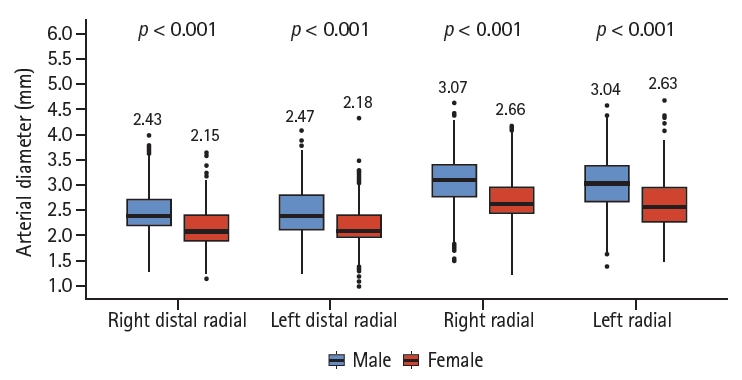
Differences in the distal radial and radial artery diameters by sex.
The proportion of patients with a DRA diameter < 2.3 mm in the right and left hands was 54.2% and 49.4%, respectively. The proportion of women with a DRA diameter < 2.3 mm was greater than that of men (67.8% vs. 44.3%, p < 0.001 in the right hand; 66% vs. 37.3%, p < 0.001 in the left hand). Fig. 4 shows the cumulative frequency of the DRA and RA diameters for men and women.

Cumulative frequencies of the distal radial artery (DRA) and radial artery (RA) diameters (A) in the right and (B) left hands of men versus women.
Clinical predictors of a DRA diameter < 2.3 mm
In the simple logistic regression analysis, female sex, BMI, BSA, CAOD, and history of PCI were the common predictors of a DRA diameter < 2.3 mm (Table 4). In the multiple logistic regression analysis, female sex (odds ratio [OR], 2.740; 95% confidence interval [CI], 2.135 to 3.516) and BMI (OR, 0.931; 95% CI, 0.899 to 0.964) were significant predictors of a right DRA < 2.3 mm in Model 1. Age (OR, 0.987; 95% CI, 0.976 to 0.997), female sex (OR, 1.851; 95% CI, 1.387 to 2.471), and BSA (OR, 0.148; 95% CI, 0.066 to 0.334) were significant predictors of a right DRA diameter < 2.3 mm in Model 2. The predictors of a left DRA diameter < 2.3 mm were similar.
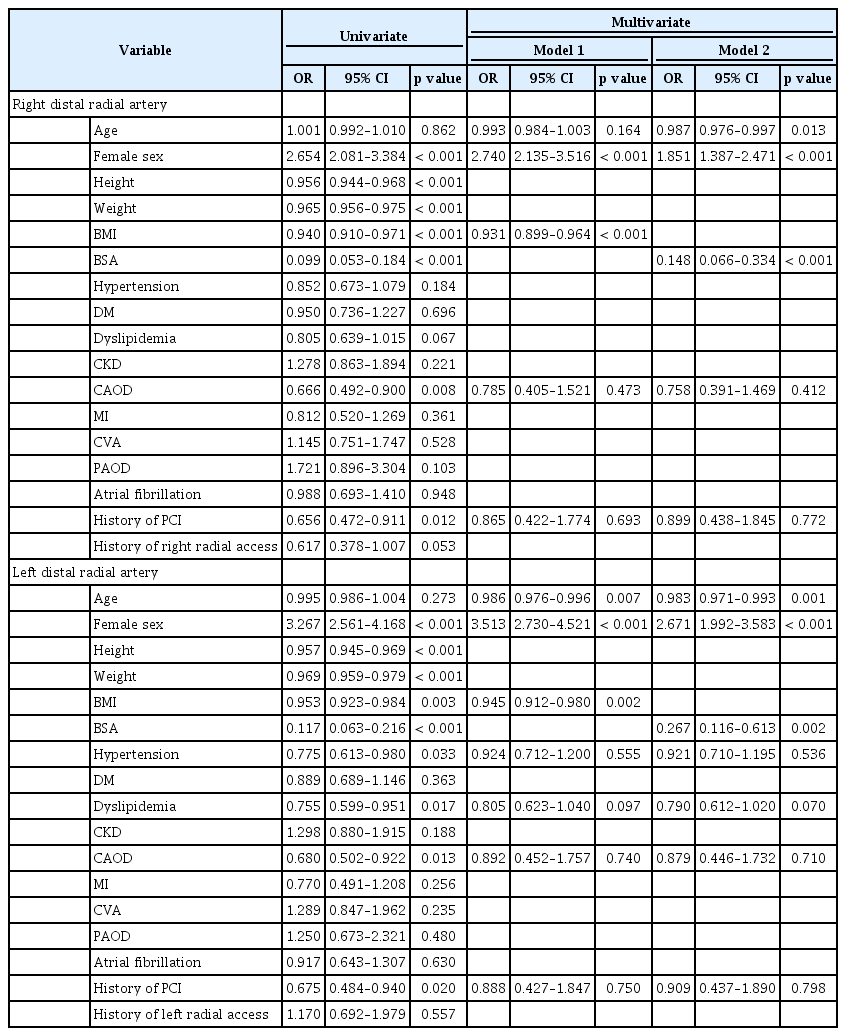
Predictors of a distal radial artery < 2.3 mm
DISCUSSION
The main aim of this study was to determine the DRA reference diameter in Korean patients. The mean DRA diameters were 2.31 ± 0.43 mm (right) and 2.35 ± 0.45 mm (left). Women had a smaller DRA than men (2.15 ± 0.38 mm vs. 2.43 ± 0.44 mm in the right hand; 2.18 ± 0.39 mm vs. 2.47 ± 0.45 mm in the left hand). The other major findings were as follows: (1) DRA diameter was approximately 20% smaller than RA diameter; (2) female patients had a smaller DRA diameter than male patients; (3) approximately 50% of patients had a small DRA (< 2.3 mm); and (4) female sex, low BMI, and low BSA were predictors of a DRA diameter < 2.3 mm.
Several studies have reported on DRA diameter (Table 5). Mizuguchi et al. [8] evaluated the DRA at two available puncture points (within and outside the anatomical snuffbox [on the dorsum of the hand]) using ultrasonography in 228 patients. The measured DRA diameter was similar to that observed in the present study. The DRA increased in size the day after the procedure and then returned to the baseline measurement after 1 month. The DRA diameter in the anatomical snuffbox was greater in a Japanese study than that observed in our study [9]. Based on the quantitative coronary angiography data obtained by Kim et al. [6], the DRA size after the injection of spasmolytics (nitroglycerin and verapamil) was similar to that reported by Norimatsu et al. [9] and was greater than that noted in our study. The smallest DRA diameter was reported by Naito et al. [10] (2.04 ± 0.60 mm in men and 1.96 ± 0.44 mm in women). The angiographic evaluation of 52 patients from Italy revealed a mean DRA diameter of 2.22 ± 0.14 mm after the administration of a vasodilatory cocktail containing 2.5 mg of verapamil, 1 mL of lidocaine hydrochloride, and 1 mL of bicarbonate [11]. The inconsistent values may be attributed to disparate definitions of vessel diameter and different points of measurement among investigators. Naito et al. [10] measured the vessel diameter of the tunica media, while we measured the outer surface of the vessels because the ultrasonographic resolution was not optimal to clearly define the inner wall of the DRA. The anatomical landmarks for the measurement of vessel diameter may also differ among investigators. To the best of our knowledge, our study included the largest number of patients to evaluate the DRA diameter. Furthermore, this study provides information on the DRA and RA diameters.

Comparison of distal radial artery diameters among studies
There is no consensus regarding the ideal method for assessing DRA diameter. The arterial diameter may be affected by emotional status, room temperature, vasospasm during skin preparation with cold antiseptic agents (povidone-iodine, betadine, and chlorhexidine gluconate), the use of spasmolytics before measurement, ultrasonographer’s technical skills, and discordance between ultrasonography and angiography measurement methods. Accordingly, a systematic protocol for assessing DRA diameter from the time of adopting the initial approach during follow-up, especially using ultrasonography, would aid in popularizing this novel approach based on the anatomic and physiological rationale [12,13]. Of note, the diameter of the actual punctured site of the DRA may be equal to or greater than the measured value because the needle usually punctures the vessel wall in an area proximal to the measured area [8].
In this study, the DRA diameter was apparently associated with a low BMI and a low BSA. BMI was significantly correlated with DRA diameter (r = 0.66, p < 0.0001) in a Japanese study of 142 patients [9]. However, another Japanese study of 120 patients did not report an association between vessel diameter and clinical variables, including BMI, in multivariate analysis [10]. In our study, a low BMI was a significant predictor of a DRA diameter < 2.3 mm in both hands. Moreover, female sex and a low BSA were strong predictors of a DRA diameter < 2.3 mm. The association between sex and RA diameter was reported in several studies. In a large-scale study evaluating RA diameter that included 1706 patients from Indonesia, India, and Macedonia, female sex was associated with a small RA (diameter < 2.8 mm) (OR, 1.72; 95% CI, 1.40 to 2.12; p < 0.001); however, a BMI < 25 kg/m2 was not a predictor for a small RA (OR, 1.0; 95% CI, 0.82 to 1.22; p = 0.93) [14]. A study conducted of a population in the United States (n = 175) reported that female sex was the only predictor of a small RA diameter [15]. Data showing an association between a low BSA with a small DRA are not available except in the current study. However, there were no sex-based differences in the indexed DRA diameter by BSA. It is worth remembering the guideline for echocardiography, which states that the cardiac volume, dimension, and valve area should be indexed with BSA for comparison with individuals with different body sizes [16-18]. From this viewpoint, a smaller DRA may be present in women with a small body size, indicating a low BSA.
A small DRA diameter is a natural limitation that should be overcome for routine CAG and PCI. An international consensus paper on preventing radial artery occlusion (RAO) after transradial angiography and interventions reported that RAO was significantly associated with an RA/sheath ratio < 1 as well as female sex, a low BMI, age, and ethnicity [19]. Miniaturized devices with a hydrophilic coating, such as the sheathless guiding catheter (Asahi Intecc, Nagoya, Japan) and the Glidesheath slender sheath (Terumo, Tokyo, Japan), may increase the possibility of using the distal radial access in patients with a small DRA and reduce the risk of DRA occlusion. A randomized study comparing distal radial access and radial access is warranted to delineate the clinical benefits and disadvantages of this alternative route.
This study has several limitations. First, the arterial diameters might have been underestimated because vasodilators were not intended to be used before measurements were taken in the echocardiography laboratory. Second, the measured DRA diameters do not reflect normative values in the general population. However, patient-level data may be valuable for individuals scheduled to undergo invasive coronary procedures. Third, there was a discrepancy between the actual puncture site and the point of measurement. A standardized protocol for assessing the DRA diameter is warranted. Fourth, technical difficulties in identifying the true inner lumen may lead to vessel size overestimations and an increased risk of arterial occlusion.
In conclusion, here we provided the DRA reference diameters of Korean patients. Approximately 50% of patients had a DRA diameter < 2.3 mm. Female sex, a low BMI, and a low BSA remained significant predictors of a DRA diameter < 2.3 mm. Ultrasonographic evaluations with clinical assessments may guide the use of distal radial access.
KEY MESSAGE
1. This study provides the distal radial artery (DRA) reference diameters of Korean patients. The mean DRA diameters were 2.31 ± 0.43 mm (total patients), 2.43 ± 0.44 mm (men), and 2.15 ± 0.38 mm (women) in the right hand and 2.35 ± 0.45 mm (total patients), 2.47 ± 0.45 mm (men), and 2.18 ± 0.39 mm (women) in the left hand.
2. The DRA diameter was approximately 20% smaller than the radial artery diameter. Approximately 50% of patients had a DRA diameter < 2.3 mm.
3. Female sex, a low body mass index, and a low body surface area were strong predictors of a DRA diameter < 2.3 mm.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
We thank Ji Eun Sim for allowing us to take representative images for assessment of the distal radial artery diameter using ultrasonography. This study was funded by a grant from Yonsei University Wonju College of Medicine (YUWCM-2020-38).