Long-term renal outcomes of patients with non-proliferative lupus nephritis
Article information

Abstract
Background/Aims
Although non-proliferative lupus nephritis (LN) (class I, II or V) has been considered as a less severe type of LN, data on long-term renal prognosis are limited. We investigated the long-term outcomes and prognostic factors in non-proliferative LN.
Methods
We retrospectively reviewed patients with systemic lupus erythematosus who were diagnosed with LN class I, II, V, or II + V by kidney biopsy from 1997 to 2021. A poor renal outcome was defined as an estimated glomerular filtration rate (eGFR) of < 60 mL/min/1.73 m2.
Results
We included 71 patients with non-proliferative LN (class I = 4; class II = 17; class V = 48; class II+V = 2), and the overall rate of poor renal outcomes was 29.6% (21/71). The univariate analysis indicated that older age, low eGFR at 6 or 12 months, failure to reach complete remission at 6 months, and LN chronicity score > 4 or activity score > 6 were significantly associated with poor renal outcomes. The multivariate analysis revealed that low eGFR at 6 months (HR 0.971, 95% CI 0.949–0.991; p = 0.014) was significantly associated with poor renal outcomes.
Conclusions
Poor renal outcomes occurred in approximately 30% of patients with non-proliferative LN after long-term follow-up. More active management may be needed for non-proliferative LN, especially for patients with eGFR < 60 mL/ min/1.73 m2 at 6 months follow-up after LN diagnosis.

INTRODUCTION
Systemic lupus erythematosus (SLE) is a chronic systemic autoimmune disease affecting various organs [1,2]. Lupus nephritis (LN), which is a kidney manifestation and one of the major organ involvements of SLE, contributes to considerable morbidity and mortality [3].
Pathologic lesions of kidney involvement in LN are currently defined and categorized according to the International Society of Pathology/Renal Pathology Society (ISN/RPS) classification [4]. Accordingly, after excluding advanced sclerotic LN (class VI), LN can be broadly classified into non-proliferative (classes I, II, and V) and proliferative (classes III and IV) forms based on the glomerular pathologies. Most of the attention paid to LN, in previous research as well as ongoing clinical trials, has primarily focused on proliferative LN because it involves severe forms and poor renal outcomes [5,6]. In this regard, patients with class III or IV LN generally require more aggressive treatment with cyclophosphamide or mycophenolate mofetil (MMF) [7].
Non-proliferative forms of LN (classes I, II, and/or V) can occur as purely membranous (class V) or mesangial (class I or II) pathologies. These non-proliferative forms of LN have been considered to cause less severe kidney involvement with good renal outcomes; thus, cytotoxic therapy is not needed in this group [8–10]. However, data on the long-term renal prognosis of patients with non-proliferative LN (classes I, II, and/or V) are very limited [11,12]. We hypothesized that clinicopathological features including medications could be related to renal outcome, and aimed to investigate the long-term outcomes and prognostic factors in non-proliferative LN.
METHODS
Study population
Patients with SLE were retrospectively analyzed from April 1997 to October 2021 at a single tertiary care academic center. All patients were diagnosed with LN based on the renal biopsy. Only patients with classes I, II, and/or V according to the 2018 ISN/RPS classification were included, and their medical records were reviewed. This study was performed in accordance with the Declaration of Helsinki and its later amendments. The Institutional Review Board of the Asan Medical Center approved this study (IRB S2022-1537). The requirement for informed consent was waived because of the retrospective nature of the study.
Renal biopsies and pathologic parameters
Renal biopsies were performed in patients with SLE with clinical or laboratory evidence of kidney involvement: increasing serum creatinine levels without compelling alternative causes (such as sepsis, hypovolemia, and medication), confirmed proteinuria of ≥ 1.0 g/24 h, or proteinuria ≥ 0.5 g/24 h plus hematuria or cellular casts [13]. The amount of proteinuria based on the urine protein/creatinine ratio (UPCR) was also taken into account. Renal biopsies were performed by skilled radiologists or nephrologists, and all biopsies were assessed by pathologists through light microscopy and immunofluorescence. Renal biopsy findings were evaluated according to the 2018 ISN/RPS classification [4].
Activity and chronicity indices were scored according to the National Institutes of Health LN Index. Activity and chronicity were scored as follows: the activity index included cellular crescents, endocapillary hypercellularity, leucocyte infiltration, subendothelial hyaline deposits, fibrinoid necrosis/karyorrhexis, and interstitial inflammation, whereas the chronicity index included glomerular sclerosis, fibrous crescents, interstitial fibrosis, and tubular atrophy.
Laboratory findings and renal outcomes
Laboratory data including levels of serum creatinine, estimated glomerular filtration rate (eGFR), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), complement (C3 and C4), anti-double-stranded DNA (anti-dsDNA) antibodies, and albumin were collected from the electronic medical records. Complete remission was evaluated at 6 and 12 months after LN diagnosis, and it was defined as proteinuria of < 0.2 g/day with stable eGFR if normal at baseline or increase in eGFR by 25% if abnormal at baseline [14]. Regarding renal prognosis, a poor renal outcome was defined as an eGFR of < 60 mL/min/1.73 m2. Data on the use of medications, such as angiotensin II receptor blockers or angiotensin-converting enzyme inhibitors, hydroxychloroquine, corticosteroid, calcineurin inhibitor, MMF, and azathioprine, were also collected.
Statistical analyses
The Mann–Whitney U and Fisher’s exact tests were used for statistical analyses, as appropriate. Cox proportional hazard regression models were used to analyze the risk factors associated with poor renal outcomes. Multivariate tests were performed by selecting factors with a p value of < 0.05 in the univariate tests through a forward stepwise approach. For all analyses, significance was set at p < 0.05. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 21 (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics of the patients with non-proliferative LN
A total of 71 patients with non-proliferative LN were included in this study, and the baseline characteristics of these patients at the time of LN diagnosis are presented in Table 1. The median age was 35.7 years, and 84.5% (60/71) were female patients. The median Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) score was 20 (interquartile range [IQR] 16–24), and the extrarenal SLEDAI score was 9 (IQR 5–12). As regards the pathologic classification based on the ISN/RPS system, the most common form was class V LN (n = 48); 4 patients had class I, 17 had class II, and 2 had a combined form of class II+V. The median eGFR level was 109.69 mL/min/1.73 m2 (IQR 82.90–133.80 mL/min/1.73 m2) at diagnosis. The median amount of proteinuria was 3,716 mg/g (IQR 1,337–4,614 mg/g) in the observed UPCR, and 59 (83.1%) patients presented with severe proteinuria (> 1 g/g) at LN diagnosis. After therapy mainly with corticosteroids, 81.7% (58/71) of the patients obtained complete remission at 6 months follow-up.

Characteristics of patients with non-proliferative LN at the time of LN diagnosis
Table 2 shows the details of the renal pathology findings of all patients with non-proliferative LN. The activity index was 5 (IQR 3–7); 6 patients had fibrinoid necrosis, 3 had cellular crescents, and 32 had interstitial inflammation. The median chronicity index was 4 (IQR 3–5), including global glomerulosclerosis (n = 31), fibrous crescents (n = 6), tubular atrophy (n = 23), and interstitial fibrosis (n = 16).
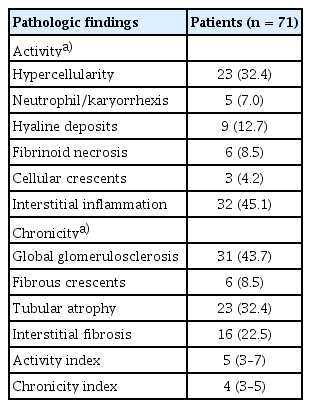
Renal pathology findings of all patients with non-proliferative LN
Long-term renal outcomes of patients with non-proliferative LN
We examined the long-term renal outcomes during the median follow-up of 103 months (IQR 27–185 mo). Figure 1 shows the detailed outcomes of all patients according to their renal function. Poor renal outcomes (eGFR < 60 mL/ min/1.73 m2) were observed in 29.6% (21/71) of the patients, including two patients with end-stage renal disease on hemodialysis. Three patients had stage 4 chronic kidney disease (defined as < 30 mL/min/1.73 m2 of eGFR).

Long-term outcomes according to the renal function in total patients with non-proliferative lupus nephritis. ESRD, endstage renal disease; eGFR, estimated glomerular filtration rate (mL/ min/1.73 m2).
Comparison of patients with and without poor renal outcomes
We subsequently compared the baseline characteristics of patients according to the development of poor renal outcomes (Supplementary Table 1). No significant differences were found in the demographic and clinical features, including age, sex, and SLE disease activity, between patients with and without poor renal outcomes. In addition, no significant differences in the levels of ESR, CRP, or anti-dsDNA antibodies were found between the two groups. However, patients with poor renal outcomes had significantly lower eGFR levels at the time of LN diagnosis than those without poor renal outcomes (p = 0.03). In addition, significantly lower eGFR levels at 6 and 12 months were found in patients with poor renal outcomes than in those without poor renal outcomes. Although significance was not reached, the group with poor renal outcomes tended to have a lower rate of complete remission at 6 months than the group without poor renal outcomes (14/21 [66.7%] vs. 44/50 [88.0%], p = 0.075).
Lastly, Cox proportional hazard regression analyses were performed to investigate the risk factors associated with the development of poor renal outcomes in non-proliferative LN (Table 3). The results of the univariate analysis showed that old age (hazard ratio [HR] 1.046, 95% confidence interval [CI] 1.003–1.091), low eGFR at 6 months (HR 0.967, 95% CI 0.948–0.986) and 12 months (HR 0.964, 95% CI 0.947–0.981), failure to achieve complete renal remission at 6 months (HR 0.332, 95% CI 0.119–0.924), activity score > 6 (HR 20.510, 95% CI 2.131–197.37), and a chronicity score > 4 (HR 3.805, 95% CI 1.192–12.144) were significantly associated with poor renal outcomes. The results from univariate analysis established that both eGFR (p = 0.001) at 6 months and attainment of complete remission at 6 months (p = 0.035) have significant impact on poor renal outcomes. In order to derive the most meaningful results in multivariate analysis, we applied the eGFR at 6 months with p value of 0.001 and activity score with p value of 0.009 as values for multivariate analysis. Finally, the results of the multivariate analysis showed that low eGFR at 6 months (HR 0.971, 95% CI 0.949–0.991, p = 0.014) was significantly associated with the development of poor renal outcomes in patients with non-proliferative LN during the follow-up period.

Univariate and multivariate Cox proportional hazard regression analyses of the factors associated with poor renal outcomes
DISCUSSION
For the analysis of long-term outcomes and prognostic factors in non-proliferative LN, this study included a total of 71 patients with class I, II, and/or V LN, followed for a median of 103 months (IQR 27–185 mo). We found that poor renal outcomes (defined as eGFR < 60 mL/min/1.73 m2) occurred in 29.6% (21/71) of the patients, and low eGFR levels at 6 months were significantly associated with the development of poor renal outcomes.
The ISN/RPS classification recognizes different classes of immune complex-mediated glomerular pathology based on the corresponding biopsy findings in LN [15]. Class I LN represents mild glomerular lesions of immune deposits limited to the mesangium without associated mesangial hypercellularity. In class II LN, the mesangial deposits detected by immunofluorescence or electron microscopy are accompanied by mesangial hypercellularity. Purely mesangial LN (classes I and II) has a better prognosis than proliferative forms (class III or IV) of LN [16]. Class V, which is a membranous LN, includes subepithelial deposition of immune complexes as the defining feature and is usually superimposed on a base of mesangial hypercellularity or mesangial immune deposits [17]. In general, because good long-term renal outcomes are expected, patients with non-proliferative LN (classes I, II, and/or V) generally do not need immunosuppressive agents [18,19]. However, according to a previous study, in purely mesangial LN (class I and II), only renin-angiotensin-aldosterone blockade therapy would be enough, but comparatively aggressive treatment could be considered in patients with class V LN with substantial proteinuria because of their potential to have poor renal outcomes [20–22]. However, despite these general concepts on the management for class I, II, or V LN, few studies have observed the long-term renal outcomes of patients with non-proliferative LN. The results of the present study included all classes of non-proliferative LN (classes I, II, V, and II + V). Thus, the findings of the present study indicated that the mesangial form (class I or II) of LN did not seem to lead to a better prognosis than class V LN. Although the included number of patients was not enough to draw a conclusion, the results of this study provide a significant reference in the long-term prognosis of all forms of non-proliferative LN.
LN classifications are not static entities and may evolve from one class to another spontaneously or after therapy [23,24]. In a review of more than 700 patients with LN who underwent repeat biopsies during their disease courses, 52.6% of cases demonstrated class switch (“transformation”) [25–27]. In our study, repeat biopsies were performed in only seven patients because of continuous proteinuria or other clinical deterioration, and 4 of the 7 patients had transformation to proliferative LN. Class switching is crucial for non-proliferative LN because it indicates a clinically significant change from a low-risk group that does not require immunosuppressive therapy to a high-risk group requiring aggressive treatment. In this regard, this study has limitations because re-biopsy was performed with only a few patients. Thus, future studies with larger numbers of patients who underwent repeated biopsies will be needed to know the significance of class transformation in the long-term prognosis of non-proliferative LN.
In this study, we found that eGFR at 6 months, but not eGFR at LN diagnosis (at biopsy time), was a significant factor for the development of poor renal outcomes. While previous studies demonstrated that eGFR levels at the time of LN diagnosis can predict poor renal outcomes, defined as doubling of serum creatinine levels or survival rate in LN [28,29], this study found significant effects of eGFR at 6 and 12 months on poor renal outcomes. Previous studies have compared non-proliferative LN to proliferative LN, in which the majority of the participants had proliferative LN and a relatively small number of patients had non-proliferative LN [30,31]. Thus, this study on the long-term renal outcomes of only non-proliferative LN would provide valuable information for the management of LN. Further prospective studies should be conducted to accurately analyze the risk factors and determine if there is a causal relationship in the results observed in the present study.
Knowing the optimal treatment for patients with LN including non-proliferative forms is important. The medication used for non-proliferative LN was highly varied in this study because of the retrospective and real-world nature of this study. In addition, we could not provide sufficient evidence for how each drug affected renal outcomes, in part due to the small number of patients to whom each drug was administered. For example, in the case of MMF, the univariate analysis showed a p value of 0.057 (Table 3), but only five patients received this drug (Table 1). Considering the lack of data on the proper management but the occurrence of poor renal outcomes in non-proliferative LN, further studies including drug randomization trials are desirable.
In conclusion, the results of this analysis of patients with non-proliferative LN showed that poor renal outcomes (eGFR of < 60 mL/min/1.73 m2) occurred in approximately 30% of patients after a long-term follow-up period. We found that eGFR values at 6 months significantly influence the development of poor renal outcomes. Thus, more active follow-up and management should be considered for patients with non-proliferative LN having a poor renal function at early time points.
KEY MESSAGE
1. After long term follow-up, about 30% of non-proliferative LN patients had poor renal outcomes (eGFR of < 60 mL/min/1.73m2).
2. Low eGFR levels at 6 months was significantly associated with poor renal outcomes.
3. More active management may be needed for non-proliferative LN patients, especially for those who have low eGFR.
Notes
Conflicts of interest
The authors disclose no conflicts.
CRedit authorship contributions
Eunsong Kang: conceptualization, data curation, formal analysis, methodology, visualization, writing - original draft, writing - review & editing; Soo Min Ahn: conceptualization, project administration; Ji Seon Oh: project administration; Yong-Gil Kim: methodology, project administration; Chang-Keun Lee: conceptualization, project administration; Bin Yoo: conceptualization, project administration; Seokchan Hong: conceptualization, formal analysis, funding acquisition, methodology, project administration, visualization, writing - review & editing
Funding
This study was supported by a grant (2022IP0062-1) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.