


INTRODUCTION
Heart failure and coronary artery disease are major causes of death in patients with chronic kidney disease (CKD)1). Measurement of serum level of brain natriuretic peptide (BNP) is helpful for diagnosis and treatment of heart failure in patients with normal kidney function2) and is known to be a useful test for the differential diagnosis of the concurrent presence of heart failure in patients visiting emergency care centers with the chief complaint of respiratory distress3). However, as the synthesis of BNP is increased within myocardial cells and BNP clearance in the kidney is decreased due to the increased water content in the body in patients with impaired renal function, the concentration of serum BNP is elevated in comparison to patients with normal kidney function. Therefore, different criteria must be applied in subjects with impaired vs. normal renal function4, 5). It is also necessary to examine whether the concentration of serum BNP affects the survival and prognosis in patients with CKD in the same manner as in normal controls.
The present study was performed to examine the usefulness of serum BNP concentration in the diagnosis of heart failure and to determine its effects on the survival and prognosis in patients with impaired kidney function.
MATERIALS AND METHODS
Patients
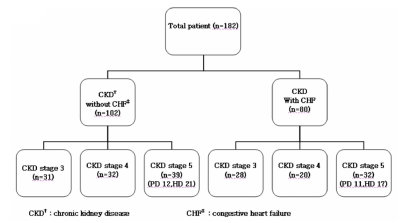
Serum BNP concentration was measured and echocardiography was performed in 182 patients with a ≥6-month history of impaired renal function (glomerular filtration rate [GFR] < 60 mL/min/1.73 m2) who had been diagnosed with CKD. The patients were recruited when they visited the Department of Internal Medicine (Division of Nephrology) between May 2001 and May 2006, with a chief complaint of respiratory distress greater than New York Heart Association (NYHA) class II. A retrospective analysis was performed. The patient diagnoses included 59 cases of CKD stage III, 52 cases of CKD stage IV, and 71 cases of CKD stage, of whom 38 and 23 were undergoing hemodialysis and peritoneal dialysis, respectively (Figure 1).
Methods
The following laboratory tests were performed: body index, ECG, chest radiography, arterial blood gas analysis, serum electrolyte, complete blood cell count, and serum chemistry for renal and hepatic function tests. Measurement of BNP level was performed at the time of initial outpatient visit for patients with CKD who were not undergoing dialysis. Measurements were performed prior to dialysis because the serum BNP concentration was reported to be elevated prior to and to decrease following dialysis as a result of the removal of fluids in dialysis patients12, 13). Blood samples of 3-5 mL were collected in test tubes containing a minimal amount of EDTA and centrifuged; the serum was isolated. Quantitative measurements were obtained by immunofluorescence labeling using a BNP kit (Triage®; Biosite, San Diego, CA, USA), with upper and lower limits of detection of 5,000 pg/mL and 5 pg/mL, respectively.
Echocardiography was performed during the hospitalization period. On M-mode test, the left ventricular diameter and ejection fraction at both end-diastole and end-systole were measured. The relaxation function was evaluated by Doppler ultrasonography. Renal function was assessed based on creatinine clearance (Ccr) in 24-h urinalysis. In accordance with the Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines, patients were classified as CKD stage III (Ccr 30-59 mL/min/1.73 m2), CKD stage IV (Ccr 15-29 mL/min/1.73 m2), and CKD stage V (Ccr < 15 mL/min/1.73 m2 or patients undergoing renal replacement therapy). Diagnostic criteria for heart failure were based on history, radiological findings, and echocardiographic findings, which included clinical symptoms fulfilling Framingham's criteria, left ventricular ejection fraction of less than 50% on echocardiography, and left ventricular diameter at end-diastole greater than 5.5 cm. Patients with past histories of chronic obstructive pulmonary disease, liver cirrhosis, malignant tumor, or multiple trauma were excluded from the present analysis. A follow-up study was performed based on hospitalization records, medical records, and telephone interview to confirm whether any of the patients had died. For analysis of patient survival, considering death as the final event, all cases in which transfer or loss to follow-up occurred were treated as having dropped out of the study. The total patient population was divided into two groups: those with impaired and those with normal heart function. The serum BNP concentration, serological and hematological findings, clinical manifestations, concurrent diseases, and echocardiographic findings were compared between the two groups, and the correlations between serum BNP concentration and other echocardiographic findings were also analyzed. Based on these findings, a retrospective analysis was performed for the factors associated with clinical course and patient survival.
Statistical analysis
Statistical analyses were performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). All data are expressed as means±standard deviation (mean±SD). Student's t-test and the χ2 test were used for comparison of continuous and discontinuous variables, respectively, between the two groups. Multiple logistic regression analysis was performed to identify the correlations between the parameters associated with heart failure. Simple linear regression analysis was performed to identify the correlation between serum BNP concentration and renal function. An inter-group comparison of the correlation between the serum BNP concentration and echocardiographic findings was performed. To confirm the accuracy of measurement of BNP level in diagnosis of heart failure in patients with renal failure, receiver operating characteristic (ROC) curve analysis was performed. The cut-off value was defined as the value with the highest sensitivity and specificity on the ROC curve. Patients were also divided into two groups based on whether BNP level was above or below the cut-off value. In these two groups, analysis of patient survival was performed using the Kaplan-Meier method. Statistical significance was set at p<0.05.
RESULTS
Patient characteristics.
A total of 182 patients, including 99 men and 83 women with a mean age of 60±13 years, were included in the present study. Patients were divided into two groups based on the presence or absence of heart failure: the heart failure group (n=80) and the normal heart function group (n=102). Mean age was 60±15 years in the heart failure group and 60±12 years in the normal heart function group; this age difference was not statistically significant. Underlying diseases for heart failure included 41 cases of hypertension (51%), 27 cases of ischemic heart disease (33%), ten cases of dilated cardiomyopathy (12%), and two cases of valvular heart disease (4%). In the heart failure group, underlying diseases for ischemic heart disease included 19 cases of stable angina (70%), four cases of ischemic heart failure (15%), three cases of acute myocardial infarction (11%), and one case of unstable angina (4%). The most prevalent cause of kidney disease was diabetic nephropathy (97 cases, 54%), followed by hypertensive nephropathy (64 cases, 35%), glomerulonephritis (15 cases, 8%), polycystic kidney disease (two cases, 1%), and idiopathic causes (four cases, 2%). In the heart failure group, the causes of renal disease included 41 cases of diabetic nephropathy (51%), 28 cases of hypertensive nephropathy (34%), and seven cases of glomerulonephritis (9%). In the normal heart function group, the causes of renal disease included 56 cases of diabetic nephropathy (55%), 36 cases of hypertensive nephropathy (35%), and eight cases of glomerulonephritis (7%). Thus, diabetic nephropathy was the most prevalent cause of renal disease in both groups. Twenty-eight (35%), 20 (25%), and 32 (40%) patients in the heart failure group, and 31 (30%), 32 (31%), and 39 (39%) patients in the normal heart function group had stage 3, stage 4, and stage 5 CKD, respectively (Figure 1).
Vital signs and clinical symptoms (Table 1)
In the total patient population, mean systolic blood pressure was 150.2±22.6 mmHg and mean diastolic blood pressure was 87.8±13.5 mmHg. There were no significant differences in systolic or diastolic pressure between the heart failure and normal heart function groups (146±20.9 mmHg vs. 152.3±23.2 mmHg, p=0.078, and 87.2±13.5 mmHg vs. 88.1±13.5 mmHg, p=0.684, respectively). The difference in number of patients with left ventricular hypertrophy on ECG between the heart failure and normal heart function groups was not significant (29 vs. 50, respectively, p=0.375). Plain chest radiography findings suggestive of pulmonary edema were observed in 42 patients in the heart failure group and in 29 patients in the normal heart function group; this difference was significant (p=0.001). In addition, findings suggestive of cardiac hypertrophy were observed in 47 patients in the heart failure group and in 37 patients in the normal heart function group; this difference was significant (p=0.0001).
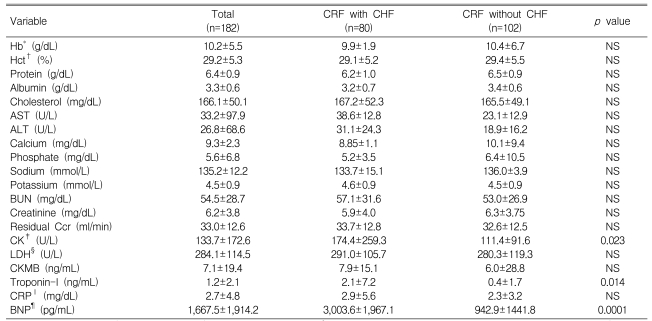
Laboratory findings (Table 2)
Mean hemoglobin level in the total patient population was 10.2±5.5 g/dL. It was 9.9±1.9 g/dL in the heart failure group and 10.4±6.7 g/dL in the normal heart function group; this difference was not statistically significant (p=0.533). On liver function test, there were no significant differences in the mean levels of the following parameters between the heart failure group and the normal heart group, respectively: total protein (6.4±0.9 g/dL; 6.2±1.0 vs. 6.5±0.9 g/dL, p=0.257); total albumin (3.3±0.6 g/dL; 3.2±0.7 vs. 3.4±0.6 g/dL, p=0.082); total cholesterol (166.1±50.1 mg/dL; 167.2±52.3 vs. 165.5±49.1 mg/dL, p=0.827); and triglyceride (141.7±79.6 mg/dL; 134.8±81.5 vs. 145.6±78.6 mg/dL, p=0.395). On kidney function test, there were no significant differences between the heart failure group and the normal heart group, respectively, in the mean levels of BUN (54.5±28.7 mg/dL; 57.1±31.6 vs. 53.1±26.9 mg/dL, p=0.388) or creatinine (6.2±3.8 mg/dL; 5.9±4.0 vs. 6.3±3.7 mg/dL, p=0.543). Furthermore, the mean serum electrolyte concentrations were as follows for the heart failure group and the normal heart group, respectively: Na+, 135.2±12.2 mmol/L; K+, 4.5±0.9 mmol/L; Cl-, 104.3±6.4 mmol/L; Ca2+, 9.3±2.3 mmol/L; and PO4 3-, 5.6±6.8 mmol/L. There were no significant differences in these values between the two groups. Mean concentration of serum BNP was 1,667.4±1,914.1 pg/mL, and this parameter showed a significant difference between the heart failure group and the normal heart group, respectively (3,003.5±1,967.1 pg/mL vs. 942.8±1,441.8 pg/mL, p=0.0001). The overall glomerular filtration rate (GFR) was 33.1±12.6 mL/min on average, and was not significantly different between the heart failure group and the normal heart group, respectively (33.7±12.8 mL/min vs. 32.6± 12.5 ml/min, p=0.584).
Other concurrent diseases
Cerebral infarction and stroke were concurrently present in eight patients in the heart failure group and in 18 patients in the normal heart function group. However, this difference was not significant (p=0.612). Cardiac arrhythmia was more prevalent in the heart failure group (five cases) than in the normal heart function group (two cases) (p=0.032). Peripheral vascular occlusive diseases were concurrently present in two patients in each groups, but this difference was not significant (p=0.536). Thirty-seven patients in the heart failure group and 59 patients in the normal heart function group had a history of smoking; this difference was not significant (p=0.341). Thirty-five and 55 patients in the heart failure group and the normal heart function group, respectively, had a past history of alcoholism; this difference was not significant (p=0.298).
Drug use history
Nitrate drugs were administered to 38 patients in the heart failure group and 33 patients in the normal heart function group. The difference between the two groups was not significant (p=0.229). Angiotensin converting enzyme inhibitor (ACE-I) was administered to 65 patients in the heart failure group and 78 patients of the normal heart function group, and the difference between the two groups was not significant (p=0.344). Angiotensin receptor blocker (ARB) was administered to 41 patients in the heart failure group and 45 patients in the normal heart function group, and the difference was not significant p=0.873). Both beta blockers and diuretics were administered at significantly higher frequencies in the heart failure group than in the normal heart function group (63 vs. 57 patients, p=0.017, and 67 vs. 48, p=0.003, respectively).
Echocardiography (Table 3)
On echocardiography, mean overall ejection fraction (EF) in the total study population was 56.0±15.6%; the value was significantly lower in the heart failure group than in the normal heart function group (39.5±10.4% vs. 59.3±8.8%, respectively, p=0.00). Mean overall left ventricular mass index (LVMI) in the total study population was 176.6±48.9 g/m2, and the value was significantly higher in the heart failure group than in the normal heart function group (186.5±46.2 vs. 166.1±50.7 g/m2, respectively, p=0.04). Mean overall left ventricular end-systolic diameter (LVESD) was 3.8±0.9 mm (4.7±0.8 vs. 3.4±0.6 mm); mean overall left ventricular end-diastolic diameter (LVEDD) mm was 5.5±0.7 mm (5.9±0.7 vs. 5.3±0.6 mm); mean overall left ventricular interseptal thickness at end-systole was 1.1±0.2 mm (1.0±0.2 vs. 1.2±0.2 mm); and mean overall left ventricular posterior wall thickness at end-diastole was 1.1±0.2 mm (1.0±0.2 vs. 1.2±0.2 mm). The differences in these parameters between the two groups were all statistically significant (p=0.00). Mean overall fractional shortening (FS) was 31.8±10.3%, and was significantly lower in the heart failure group than in the normal heart function group (20.9±6.6 vs. 37.5±6.7%, p=0.00). Local motor disturbances were more prevalent in the heart failure group than in the normal heart function group (30 vs. 15 cases, respectively, p=0.00). The numbers of cases in which pericardial effusion was classified as "mild" or "severe" were 28 and 3 in the heart failure group and 28 and 4 in the normal heart function group, respectively; these differences were not statistically significant (p=0.542)
Causes of death
Of the total of 80 patients in the heart failure group, 38 had died, six were lost to follow-up, and 36 were currently being followed-up at the Outpatient Clinic of the Department of Nephrology. Of the total of 102 patients in the normal heart function group, 31 had died, eight were lost to follow-up, and 63 were currently being followed-up at the Outpatient Clinic of the Department of Nephrology. The most prevalent cause of death was cardiovascular disease, accounting for 30 deaths in the total study population (26 vs. 4 cases in the heart failure and normal heart function groups, respectively). This was followed by 14 cases of sepsis (3 vs. 11 cases), 11 of idiopathic causes (3 vs. 8 cases), six cases of cachexia (all in the normal cardiac function group), five cases of stroke or cerebrovascular hemorrhage (4 vs. 1 case), one case of gastrointestinal bleeding (in the normal heart function group), and one case of malignant tumor (in the heart failure group).
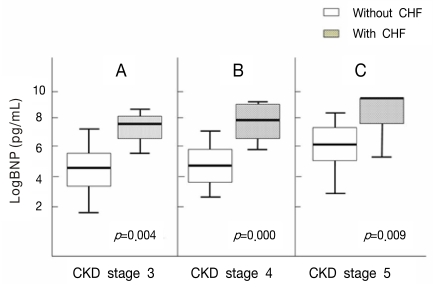
Correlation between renal function and serum BNP concentration (Figure 2)
(1) Difference in serum BNP concentration between the two groups in patients with CKD stage 3
The serum BNP concentration was 205.7±273.4 pg/mL in the normal heart function group and 1,618.4±1,237.7 pg/mL in the heart failure group. Thus, it was significantly elevated in the heart failure group (p=0.004).
(2) Difference in serum BNP concentration between the two groups in patients with CKD stage 4
The serum BNP concentration was 284.0±435.6 pg/mL in the normal heart function group and 2,713.0±2,023.3 pg/mL in the heart failure group. Thus, it was significantly elevated in the heart failure group (p=0.000).
(3) Difference in serum BNP concentration between the two groups in patients with CKD stage 5
The serum BNP concentration was 1,275.3±1,634.5 pg/mL in the normal heart function group and 3,519.1±1,935.8 pg/mL in the heart failure group. Thus, it was significantly elevated in the heart failure group (p=0.009).
(4) Serum BNP concentration depending on hemodialysis
A comparison of BNP level depending on hemodialysis was performed in all patients with renal failure, without considering heart function. The results indicated BNP levels of 2,008.4± 2,036.1 pg/mL and 1,319.0±1,723.3 pg/mL in patients who were and who were not receiving hemodialysis, respectively (p=0.015).
(5) Difference in serum BNP concentration depending on CKD stage in the normal heart function group
In patients in the normal heart function group with chronic renal failure, the concentrations of serum BNP at CKD stages 3, 4, and 5 were 205±273.4, 284±435.6, and 1,275±1,634.5 pg/mL, respectively. There was no significant difference between CKD stage 3 and stage 4. However the differences between CKD stage 4 and stage 5 and between CKD stage 3 and stage 5 were significant (p=0.018 and p=0.006, respectively).
(6) Difference in serum BNP concentration depending on CKD stage in the heart failure group
In patients in the heart failure group with chronic renal failure, the concentrations of serum BNP at CKD stages 3, 4, and 5 were 1,618±1,237.7, 2,713±2,023.3, and 3,519±1,935.8 pg/mL, respectively. There were no significant differences between CKD stage 3 and stage 4 or between CKD stage 4 and 5. However, the difference between CKD stage 3 and stage 5 was significant (p=0.011).
Correlations between serum BNP concentration and other parameters (Figure 3)
(1) Correlation between serum BNP concentration and left ventricular ejection fraction on echocardiography
There was a significant inverse correlation between serum BNP concentration and left ventricular ejection fraction in patients with CKD (R2=0.172, p=0.001).
Diagnostic value of BNP level in detecting heart failure in patients with renal failure (Figure 4)
(1) ROC curve of total patient population
In the total patient population, when BNP level was 858.5 pg/mL and the area under the curve (AUC) was 0.823, a diagnosis of heart failure was made with sensitivity of 77% and specificity of 72%.
Analysis of patient survival (Figure 5)
(1) In all patients (CKD stage 3-5), patient survival was significantly lower in the group with BNP level higher than 858.8 pg/mL (p=0.012).
(2) In patients who underwent renal replacement therapy, survival analysis showed that patient survival was significantly lower in the group with BNP level higher than 1,650 pg/mL (p=0.004).
Multivariate analysis (Table 4)
In all patients, group assignment was made based on the cut-off value of BNP level of 858.5 pg/mL obtained from the ROC curve. Multivariate analysis was performed to identify the independent factors affecting patient survival in each group. In the group with BNP level exceeding 858.5 pg/mL, the factors associated with patient survival included BNP level and age. In this group, however, sex, diabetes mellitus, left ventricular mass index, left ventricular ejection fraction, and residual renal function were not independent factors affecting patient survival. In the group with BNP level less than 858.5 pg/mL, the factors associated with patient survival were age and albumin level. In this group, however, other parameters were not independent factors affecting patient survival.
DISCUSSION
In patients visiting the outpatient clinic with a chief complaint of respiratory distress, it is critical to determine whether the etiology is of cardiogenic or non-cardiogenic origin to decide on an appropriate treatment plan and to estimate prognosis. Respiratory distress symptoms are of nonspecific origin, which cannot be differentially diagnosed based on an interview or routine laboratory tests. Echocardiography is costly and requires highly trained personnel. Accordingly, simplified methods have been developed for measurement of serum BNP concentration and their use has become widespread in the assessment of cardiac function6, 7). BNP is a peptide hormone that is secreted in response to muscular relaxation in the left ventricle and is converted to two biologically active forms: c-BNP and N-terminal pro-BNP. N-terminal pro-BNP has a longer half-life and is more biologically stable than c-BNP, and it has greater clinical significance8). Recent studies have shown that these natriuretic peptides accurately indicate the treatment response and prognosis as well as fulfill the requirements for a diagnosis of heart failure9).
Left ventricular hypertrophy and left ventricular dysfunction are present concurrently in 60-80% and approximately 15% of patients with CKD, respectively. A number of studies have been performed to examine the diagnostic value of BNP level in detecting cardiogenic respiratory distress10). In some studies, the serum BNP concentration was not increased in comparison to the normal value in patients with chronic renal diseases who had normal kidney function and showed no left ventricular hypertrophy on echocardiography5). According to most of these studies, however, the volume of water content was elevated and renal clearance of BNP was decreased in patients with CKD compared to patients with normal kidney function. It has also been reported that serum BNP concentration is elevated in patients with chronic renal failure compared to those with normal kidney function11, 12). However, the serum BNP concentration has also been shown to be associated with left ventricular dysfunction and left ventricular hypertrophy in patients with CKD or end-stage renal disease. Similar to observations in patients with normal kidney function, the serum BNP concentration has been reported to be a prognostic indicator of the occurrence of cardiovascular disease and death in patients with CKD or end-stage renal disease13-15).
There is still a great deal of controversy regarding the cut-off value of BNP level in the diagnosis of heart failure in patients with CKD. Only a small number of studies have examined the effects of BNP level on survival rate in these patients. Kim et al.7) maintained that a diagnosis of cardiac failure could be made with sensitivity and specificity of 77% and 71%, respectively, using a BNP cut-off value of higher than 600 pg/L in patients with chronically impaired kidney function. McCullough et al.2) reported that it would be appropriate to apply a diagnostic value of approximately 200 pg/mL in cases with GFR lower than 60 mL/min/1.73 m2. Wang et al.10) noted that a diagnosis of cardiac failure could be made with sensitivity and specificity of 66% and 70%, respectively, using a BNP cut-off value of higher than 829 pg/L in patients with CKD in whom systolic heart failure was absent. According to these authors, when the renal function was classified as moderate renal failure (60>Ccr≥30 mL/min), severe renal failure (30>Ccr≥15 mL/min) and end-stage renal failure (Ccr<15 mL/min), comparison of BNP level can be problematic. In cases with concurrent heart failure, however, the serum BNP concentration was significantly elevated in patients with renal failure of corresponding severity (1,183±1,056, 2,205±1,470, 3,209±1,900 pg/mL). In the present study, a diagnosis of heart failure could be made with sensitivity and specificity of 77% and 72%, respectively, in the total CKD patient population when the concentration of serum BNP exceeded 858.5 pg/mL. In comparison with other studies, our figures were relatively high. This may be explained by the fact that McCullough et al. excluded the dialysis group, unlike the present study, and Kim et al. used a BNP upper limit of 2,000 pg/mL (vs. 5,000 pg/mL in the present study). In our series, BNP level depending on the CKD stage was elevated with no relation to cardiac dysfunction in CKD stage 5. This may have been due to the effects of left ventricular hypertrophy, impairment of relaxation function, hemoglobin, albumin, and drugs used in treatment4).
There have been many recent studies of the correlations between BNP level, cardiac function, and patient prognosis. Kim et al.7) and Takayoshi et al.14) reported that the concentration of serum BNP was inversely correlated with left ventricle ejection fraction. Nitta et al.15) reported that the mean serum BNP concentration was higher in hemodialysis patients than in normal healthy subjects, and there was an inverse correlation between the serum BNP concentration and the left ventricular function. The results of the present study also indicated an inverse correlation between the serum BNP concentration and left ventricle ejection fraction on echocardiography. This study also indicated that serum BNP concentration shows an inverse correlation with patient survival and a positive correlation with left ventricular mass index (LVMI).
In the present study, the cumulative survival rates were calculated based on the serum BNP concentration, which can be used for diagnosis of heart failure. The results revealed a significant difference in patient survival, indicating that the concentration of serum BNP is a prognostic indicator for prediction of patient survival in patients with chronic renal failure as well as those with normal kidney function. In another study examining the correlation between serum BNP concentration and patient survival in patients with CKD, Yoichi et al.5) analyzed the incidence of heart disease in patients with CKD who had normal heart function. These authors reported significant differences in the incidence of cardiac disease and patient survival based on a BNP cut-off value of 150 pg/mL. Wendy et al.12) reported that the incidence of heart disease increased and there are significant differences in patient survival based on a cut-off value of 175 pg/mL. Moreover, other studies have also indicated that the serum BNP concentration is a useful indicator for diagnosis of left ventricular hypertrophy or left ventricular dysfunction in hemodialysis patients with CKD. Furthermore, it has also been reported that the serum BNP concentration is a powerful indicator for prediction of prognosis in patients in whom cardiovascular diseases are accompanied by left ventricular hypertrophy or left ventricular dysfunction17, 18).
In the present study, the serum BNP concentration showed a positive correlation with that of serum creatinine in patients with CKD. Here, the cut-off value of BNP level was 858.5 pg/mL. In addition, there were significant differences in serum BNP concentration depending on the presence of heart failure at identical CKD stages. In patients with CKD stage 5, however, the serum BNP concentration was relatively high with no relation to the presence of heart failure, in comparison to those with CKD stage 3 or 4. These results indicate that assessment of cardiac function based on the concentration of serum BNP depending on each CKD stage will be useful for determining prognosis as well as for planning treatment in patients with CKD.






 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





