


INTRODUCTION
Intrahepatic cholangiocarcinoma (ICC), the second-most common primary hepatic tumor (after hepatocellular carcinoma [HCC]), accounts for approximately 3% of all gastrointestinal tumors and 10% to 15% of primary liver malignancies [1,2]. The incidence and mortality rates of ICC have been increasing globally in recent decades. ICC is a lethal malignancy, with a median survival of 6.5 months from the time of diagnosis in untreated patients [3]. However, the etiology of cholangiocarcinoma remains unclear. The primary risk factor for ICC is primary sclerosing cholangitis. Obesity, inflammatory conditions of the biliary tract, ulcerative colitis, smoking, CaroliŌĆÖs disease, exposure to radiopaque medium thorium dioxide (Thorotrast, Testagar & Co. Inc., Detroit, MI, USA), and diabetes have also been proposed as risk factors [1,3]. Hepatitis viruses, including hepatitis B virus (HBV) and hepatitis C virus (HCV), are causative agents of HCC. Recent studies have shown that both HBV and HCV infections can cause ICC [4,5], which may explain its increasing incidence. Regardless of etiology, surgical resection offers the only prospect of cure; however, only a small percentage of patients with ICC have resectable cancer at the time of diagnosis.
Given the increasing incidence of ICC, its poor prognosis, and the lack of adequate treatment options, further studies exploring its risk factors, prognostic indicators, and outcomes are required. While several recent studies have indicated that HBV and HCV infections have prognostic significance for ICC [6,7], the prognostic impact of such infections remains controversial. Therefore, we performed a retrospective study of all patients with ICC treated between 2005 and 2018 at a single institution to evaluate the prognostic value of hepatitis virus infection status and to identify other prognostic factors that affect survival in patients with ICC.
METHODS
Patients
A retrospective chart review was performed for patients diagnosed with ICC between August 2005 and December 2018 at Konkuk University Medical Center. All patients with an intrahepatic mass were evaluated for operability by computed tomography (CT), magnetic resonance imaging (MRI), endoscopic retrograde cholangiopancreatography, or magnetic resonance cholangiopancreatography. Ultrasound-guided biopsies were performed to confirm the pathologic diagnosis when patients were assessed with unresectable ICC by radiologic examination. Patients with HCC-cholangiocarcinoma mixed type, intraductal papillary biliary neoplasm, periductal infiltrative cholangiocarcinoma, or intraductal growing type were excluded. Only the mass-forming type was included. Patients with extrahepatic or hilar cholangiocarcinoma, neuroendocrine tumor, or sarcoma were excluded. Serologic tests were performed for hepatitis B surface antigen (HBsAg), anti-HCV, indicators of liver function, carbohydrate antigen 19-9 (CA 19-9), and ╬▒-fetoprotein (AFP) level. Tumor-node-metastasis (TNM) staging of ICC was performed according to the 7th edition of the American Joint Committee on Cancer (AJCC) staging systems. Surgical procedures were divided into major and minor resections. Major resection included hemihepatectomy and central bisectionectomy, while minor resection included sectionectomy and segmentectomy. This study was approved by the Institutional Review Board of Konkuk University Medical Center (KUH 1010778). Written informed consent by the patients was waived due to a retrospective nature of our study.
Statistical analysis
Statistical analyses were performed using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was defined as p < 0.05. Survival of patients in the study group was measured from the time of diagnosis. The study groups were compared using the chisquare test or FisherŌĆÖs exact test for categorical variables and WilcoxonŌĆÖs rank-sum test for continuous variables. Overall survival with HBV infection status was calculated using the Kaplan-Meier method. Log-rank tests were used to assess differences. Univariate and multivariate analyses were performed using the Cox proportional-hazards model, with the backward Wald procedure.
RESULTS
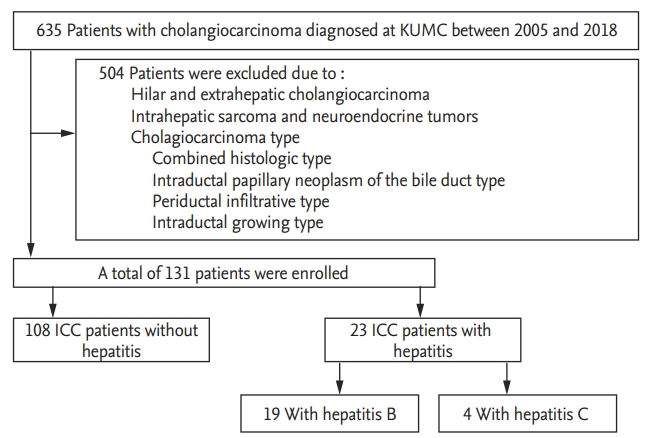
Of the 635 patients diagnosed with cholangiocarcinoma during the study period, 131 patients had ICC (Fig. 1). Table 1 describes the clinical features of the patients in the study group. It included 74 males and 57 females, with a mean age of 66.6 ┬▒ 11.7 years. Among these, a total of 17.6% (23/131) were positive for either HBsAg (19/23) or anti-HCV (4/23). The distribution among the seven different AJCC stages was as follows: I (14.5%), II (9.9%), III (2.3%), IVa (34.4%), and IVb (38.9%). Of the 131 patients, 37 underwent curative surgery (29.1%). In 16 patients (12.7%), surgery was followed by adjuvant chemotherapy. The median overall survival of patients with ICC was 213 days.
The clinical features of hepatitis-B-associated ICC are listed in Table 2. Hepatitis B-associated ICC patients were significantly younger (6.75 [interquartile range, IQR, 60.5 to 76] vs. 57 [IQR, 52.0 to 64.0], p = 0.002) with higher albumin (3.6 [IQR, 3.3 to 4.0] vs. 3.9 [IQR, 3.4 to 4.3], p = 0.044) and higher AFP (3.0 [IQR, 2.5 to 5.0] vs. 7.0 [IQR, 3.0 to 190.8], p = 0.016) than those without hepatitis. There were no significant differences in other clinical indices, including bilirubin level, CA 19-9 level, or TNM stage. Hepatitis-C-associated ICC patients were not significantly different in clinical indices.
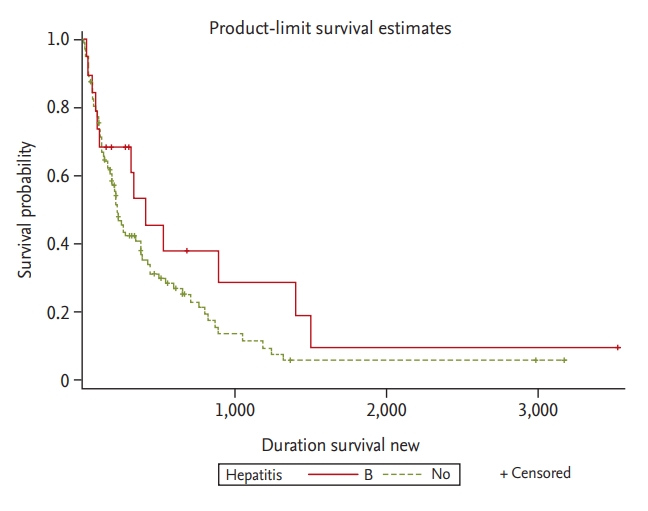
Overall survival rates of ICC patients with and without hepatitis were not significantly different (p = 0.279). In addition, there was no significant difference in overall survival with HBV infection status (p = 0.164) (Fig. 2). Table 3 describes the prognostic factors for survival identified in the study group. In univariate analyses, factors associated with survival included age Ōēź 65 years (p = 0.005), albumin Ōēź 3.5 g/dL (p = 0.025), CA 19-9 Ōēź 100 ng/mL (p < 0.001), T stage (T1ŌĆōT3) at diagnosis (p < 0.001), presence of lymph node invasion (p < 0.001), presence of metastases at diagnosis (p < 0.001), adjuvant chemotherapy after surgery (p = 0.004) and curative surgery (p < 0.001). The median survival of ICC patients with and without hepatitis was 280 and 213 days, respectively. Survival rates did not differ significantly between the two groups (p = 0.279). In addition, the median survivals of patients with hepatitis B, hepatitis C, and without hepatitis were 302, 128.5, and 213 days, respectively. Survival rates did not differ significantly among the three groups (p = 0.166 vs. p = 0.603). In multivariate analyses, CA 19-9 < 100 ng/mL (p < 0.001), T stage (T1ŌĆōT3) at diagnosis (p = 0.042), the absence of lymph node invasion (p = 0.043), and curative surgery (p = 0.033) were significant and independent predictors of a more favorable outcome.
DISCUSSION
The incidence of ICC is increasing, generating clinical interest in improving outcomes and identifying prognostic factors. Recently, many studies have indicated that HBV and HCV infection are statistically associated with ICC [4,5,8]. HBV and HCV infection are endemic in Korea. In our study, 17.6% of patients with ICC (23/131) were positive for HBV or HCV infection. Although we explored the prognostic value of hepatitis virus infection, we found no significant difference in overall survival between ICC patients with and without hepatitis, although some clinical features did differ between the two groups.
Cholangiocarcinoma is more common in older patients [9]. ICC typically presents sporadically as a discrete intrahepatic mass in patients over 65 years of age [10]. In our study, the mean age of patients at the time of ICC diagnosis was 66.6 years; in patients with underlying HBV infection, ICC diagnosis occurred at an earlier age, with a mean age at presentation of 57.0 years (p = 0.002) (Table 2). Although these patients were diagnosed at an earlier age, most had metastatic disease or unresectable tumors at the time of diagnosis. This may be due to specific mechanisms induced by hepatitis virus infection, but this remains unclear. In several recent studies, HBV nucleic acid and HCV ribonucleic acid (RNA) have been identified in cholangiocarcinoma cells. These findings indicate that hepatitis viruses may induce cholangiocyte proliferation and dysplasia that leads to ICC development [11-14]. AFP is the most common marker for fetal hepatoblasts, hepatic progenitor cells (HPCs), or HCC. This study found that serum AFP levels > 20 ng/mL were present in about 30.4% of hepatitis-positive ICC patients [15]. HBV and HCV cause viral hepatitis and may cause cancer by inducing chronic inflammation in both hepatocytes and cholangiocytes, leading to high levels of serum AFP. Recently, two clinical studies implied that both hepatitis-associated ICC and HCC share a common carcinogenesis process and that both arise from HPC [11,15]. In this study, the incidence of AFP > 20 ng/mL was much higher in hepatitis-associated ICC than in ICC patients without hepatitis (30.4% vs. 9.3%). These findings may imply that, during the process of malignant transformation, HPCs retain their ability to produce AFP.
Based on gross morphological features, ICC can be classified into three subtypes: mass-forming, periductal-infiltrating, and intraductal. Etiologies involving distinct molecular pathways may be associated with ICC subtypes. For example, ICC associated with hepatolithiasis and Clonorchis sinensis infection nearly always has an intraductal growth pattern [16]. In our study, although six patients were excluded based on exclusion criteria, we found that hepatitis-associated ICC tended to be of the mass-forming type (23/29). As noted above, it has been suggested that hepatitis-associated ICC and HCC share a common disease mechanism.
In our study, approximately 75% of patients had TNM stage III or IV and unresectable tumors at the time of diagnosis. Better survival was observed in patients with CA 19-9 < 100 ng/mL, with T stage 1 to 3 at diagnosis, and without lymph node invasion. In addition, curative surgery was better for survival if curative surgical resection was possible. Tumor size, tumor differentiation, anatomical resection, perineural invasion, presence of vascular invasion, and cirrhosis, which have been reported to be associated with prognosis in previous studies, were not statistically significant in our study [17-22].
In conclusion, ICC is associated with a poor prognosis; therefore, an improved understanding of the factors that determine patient outcomes is required. In many recent studies, HBV and HCV are possible risk factors for ICC development. In this study, we did not find a prognostic value for hepatitis virus status in ICC patients; however, patients with hepatitis-associated ICC showed several clinical features that differed from those in patients without hepatitis. The limitations of this study include its small sample size and retrospective nature. Therefore, a larger prospective study is needed to clarify the prognostic role of HBV and HCV infection for ICC.
KEY MESSAGE
1. Hepatitis B virus (HBV) or hepatitis C virus (HCV) may be involved in the development of intrahepatic cholangiocarcinoma (ICC).
2. While hepatitis influenced a number of clinical features in ICC patients, it did not affect survival rate.
3. Prognostic factors inf luencing survival outcomes with ICC were carbohydrate antigen 19-9 level, T stage, the presence of lymph node metastasis, and curative surgery.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





