


INTRODUCTION
Various vaccines for coronavirus disease 2019 (COVID-19) are being developed, with some being used under emergency approval. However, most COVID-19 vaccine trials enrolled a limited number of elderly participants and patients with chronic lung diseases. Hence, ensuring the effectiveness and safety of vaccination in these populations is challenging [1]. As novel vaccines are administered worldwide, very rare but potentially serious adverse events (AEs) have been reported.
Cases of myocarditis after COVID-19 vaccination have been continuously reported in safety surveillance and published literature. Through large healthcare data analysis, the BNT162b2-mRNA vaccine was associated with a risk of myocarditis [2,3]. In contrast, vaccine-induced immune thrombotic thrombocytopenia is more relevant to adenoviral vector-based vaccines, and a convincing pathogenesis has been revealed [4–6]. However, pre-approval trials have not identified these rare AEs. Clinical trials with a limited number of participants who meet the inclusion criteria lack the power to identify these AEs [7–9]. Although scarce, the significance of AEs cannot be underestimated as a massive amount of vaccination has been conducted and might continue.
Vaccine-related lung toxicity is rare and not well known, although reports of pneumonitis after influenza vaccinations have been published, mainly in Asian countries [10]. Moreover, it may be misdiagnosed as infectious pneumonia unless suspected and not easily identified as skin AEs [11]. In mild cases, the lung parenchymal lesions could not be identified by simple chest radiography but only by computed tomography (CT) [12]. Therefore, the true prevalence of AEs is difficult to estimate. However, we recently reported a case of COVID-19 vaccine-related pneumonitis (CV-P) in an elderly patient (patient #1) [13]. Herein, we describe other Korean cases of CV-P with different clinical and radiological features and review the literature.
METHODS
We diagnosed CV-P using the clinical criteria for drug-induced pneumonitis suggested by Camus et al. [14] and the radiological criteria suggested by the Fleischner Society [12,14]. Our working definition of CV-P is shown in Table 1 and Supplementary Table 1. Patients without underlying interstitial lung disease (ILD) were classified with de novo CV-P and differentiated from patients with pre-existing ILD. As with the diagnostic process of drug-related pneumonitis, the diagnosis was reached by excluding other diseases by evaluating various possible differential diagnoses. COVID-19 polymerase chain reaction (PCR) testing (Real-Q 2019-nCoV Detection kit, BioSewoom, Seoul, Korea) was performed to confirm severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection [13] using nasopharyngeal swabs, sputum, or bronchoalveolar lavage (BAL) fluid. To exclude infectious pneumonia, conventional cultures, respiratory bacterial multiplex PCR tests (Allplex PneumoBacter Assay, Seegene, Seoul, Korea), and seasonal respiratory virus multiplex PCR tests (Real-Q RV Detection kit, BioSewoom) were performed. All microbiological tests performed for differential diagnosis are summarized in Supplementary Table 2. Bronchoscopy was recommended and performed with patients’ informed consent after considering the risk-benefit ratio. Echocardiography was performed in all patients without underlying ILD.
South Korea introduced the BNT162b2-mRNA vaccine program for the elderly (age ≥ 75 years) in April 2021; the vaccines were administered on a large scale within a short period. Since then, vaccination programs with both BNT162b2-mRNA and ChAdOx1 nCoV-19 vaccines have been extended to include younger individuals. Physicians diagnosing or treating COVID-19 vaccine-related AEs are obligated to report them to the Korea Disease Control and Prevention Agency that publishes weekly national reports on vaccine-related AEs [15]. We compared this data with that of the Public Health Agency of Canada that has a similar surveillance system and publishes weekly AE reports [16].
The study institution is the only tertiary referral hospital covering three adjacent cities (Anyang, Gunpo, and Uiwang: population, 0.98 million). The observed incidence of CV-P was calculated using the number of patients diagnosed and the number of vaccinees administered in the three cities until the date of presentation of the last diagnosed patient. The Institutional Review Board approved this study (HAL-LYM2021-08-006). We obtained written informed consent from the patients for publication of their clinical features and radiological images.
RESULTS
Baseline characteristics and diagnosis
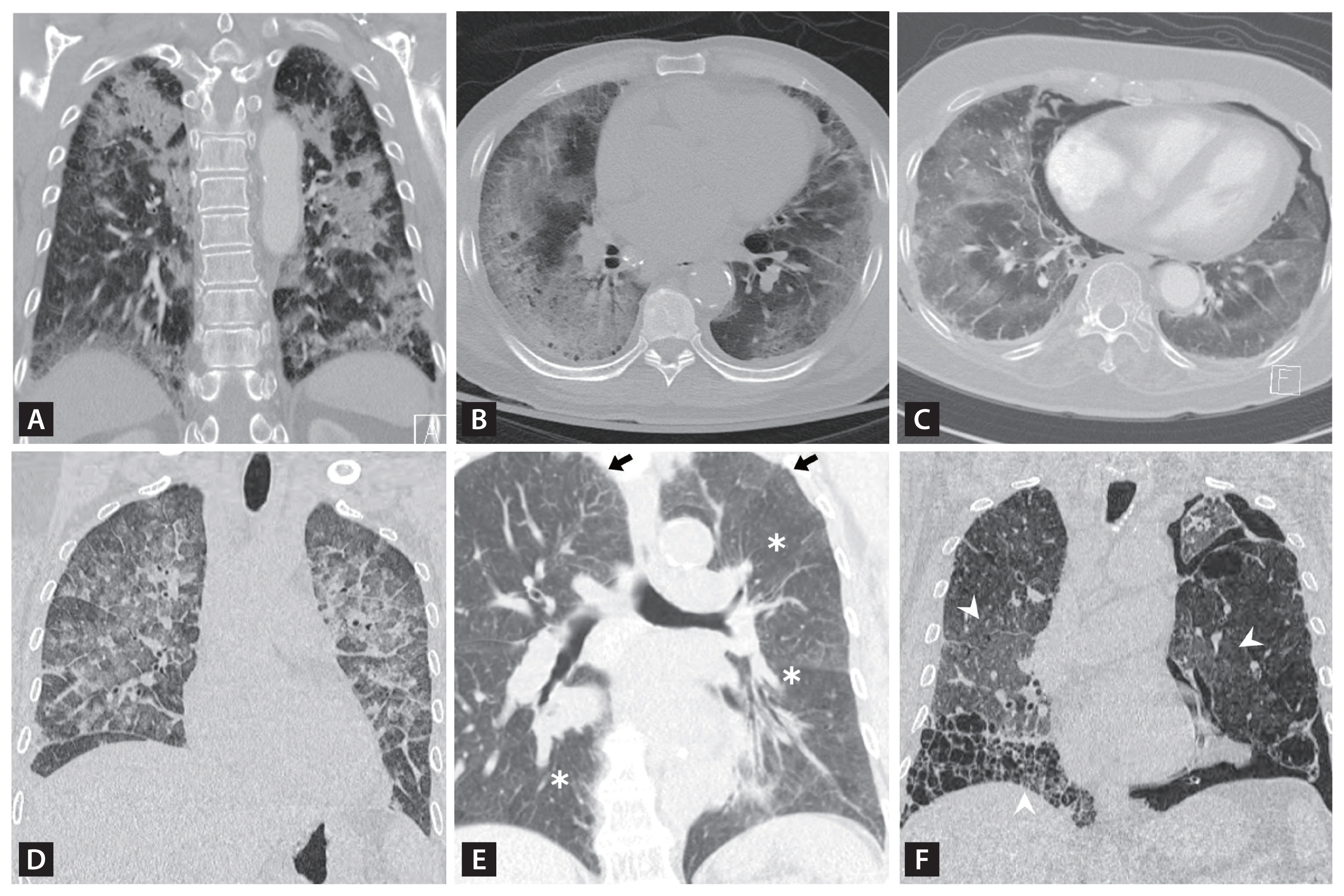
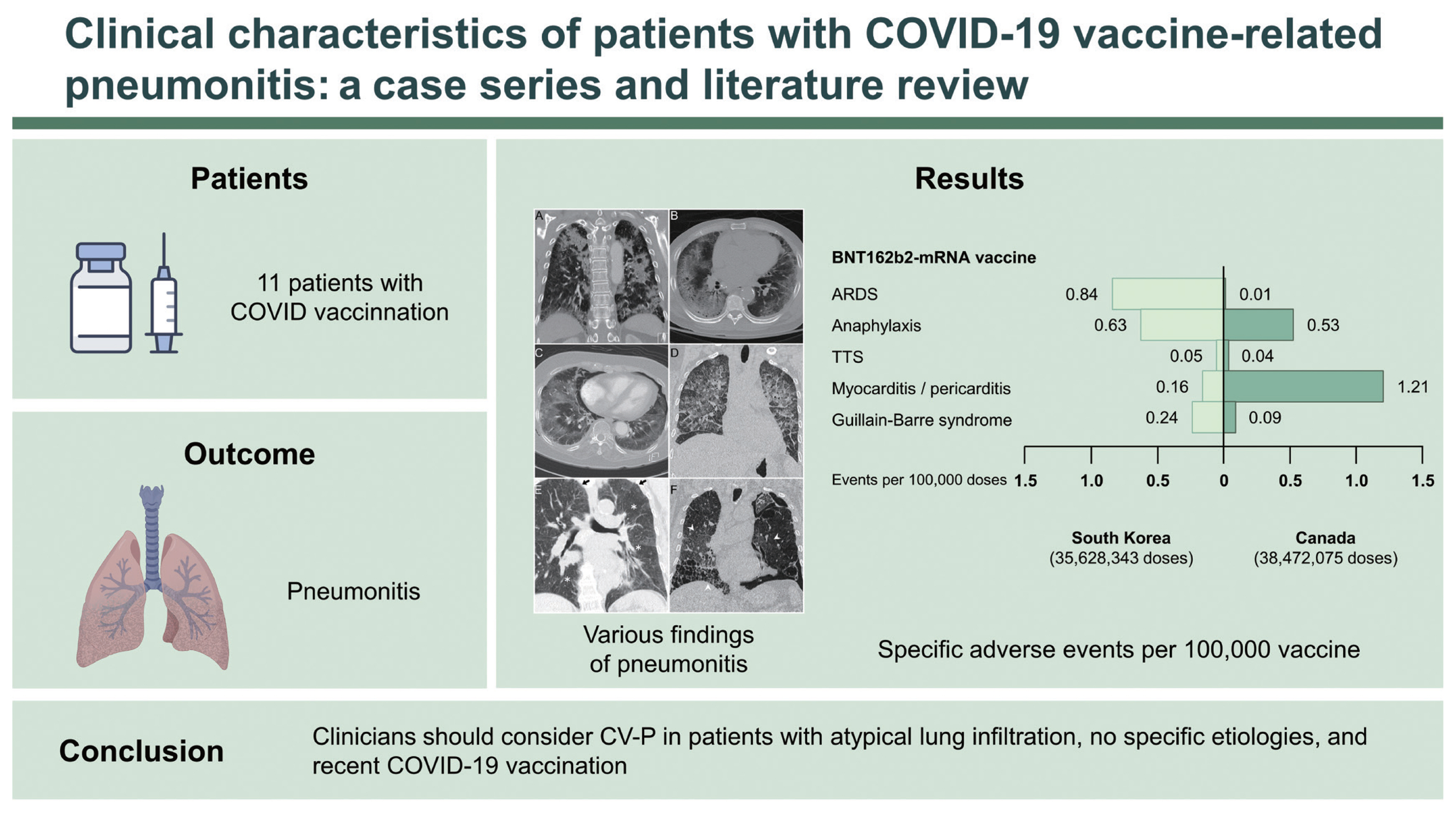
Eleven patients with CV-P were enrolled (median age, 80 years; five male and six female patients). Ten patients received the BNT162b2-mRNA vaccine (first dose: six patients), and one received the first dose of ChAdOx1 nCoV-19. No patients had been infected by SARS-CoV-2 previously or at presentation or had a history of vaccine-related AEs (Tables 2 and 3). According to the chest CT pattern, four of the eight patients with de novo CV-P were subcategorized as having organizing pneumonia and four as having diffuse alveolar damage (DAD). We confirmed the absence of underlying ILD using radiological images previously obtained for health check-ups or other medical reasons (CT, 3/8; radiograph, 8/8). Three patients had pre-existing ILD: hypersensitivity pneumonitis (HP), airspace enlargement with fibrosis, and idiopathic pulmonary fibrosis (IPF). We identified newly aggravated parenchymal lesions (increased ground-glass opacity or consolidation) through comparison with stable background ILD findings. All three patients were clinically and radiologically stable without anti-inflammatory drugs or anti-fibrotic agents before vaccination. The radiological findings of representative cases are shown in Fig. 1. Radiological images before and after CV-P of all patients except patient #1 are shown in Supplementary Figs. 1–10.
De novo CV-P and aggravation of pre-existing ILD
We compared the clinical features of patients who developed de novo pneumonitis after vaccination (n = 8) with that of those with pre-existing ILD (n = 3) (Table 2). The median time from the most recent vaccination to symptom onset was 9 days in patients with de novo CV-P and 7 days in those with pre-existing ILD. All patients with de novo CV-P had dyspnea. Aggravation of cough and sputum production were the main symptoms of patients with pre-existing ILD. Fever (> 38°C) occurred in five of the eight patients with de novo CV-P; however, none developed fever in the pre-existing ILD group. The median C-reactive protein level was 3.8 mg/dL, showing a moderate increase in most cases. No patients had procalcitonin levels > 0.5 ng/mL. Echocardiography in all eight patients with de novo CV-P demonstrated normal left ventricular systolic function and wall motion. In the de novo group, antinuclear antibody was positive in three out of eight cases, and anti-SSA/Ro antibody was positive in two cases.
Management and prognosis
Systemic corticosteroids were administered after diagnosis in all patients, and the attending physician determined the starting dose. In the de novo patient group, the methylprednisolone equivalent dose was started at a median value of 57 mg/day. All patients with underlying pre-existing ILD were treated with methylprednisolone 8 mg/day. One patient with acute respiratory distress syndrome (ARDS) died despite appropriate treatment (Patient #5: DAD pattern) (Fig. 1C). All other patients responded well to corticosteroids, and improvement was maintained without sequelae during follow-up.
Observed incidence
Our observed incidence of CV-P was 1.37 per 100,000 (11/804,318 with at least one dose of COVID-19 vaccine in the three cities until November 27, 2021).
A representative case presentation and radiological features
Patient #2 (Fig. 1A): An 83-year-old woman who received the second dose of BNT162b2-mRNA vaccine presented with an organizing pneumonia pattern of CV-P. Chest CT revealed multifocal patchy consolidations, ground-glass opacifications (GGOs), and mild interlobar septal thickening in both lungs (14 days after the second dose). BAL fluid analysis revealed neutrophils (Np) 24%, lymphocytes (Lp) 32%, eosinophils (Eo) 32%, and macrophages (Mq) 12% (Supplementary Table 3). All microbiological tests in BAL specimens were negative. Intravenous methylprednisolone was initiated at 24 mg/day, and the patient had a rapid response to treatment.
Patient #6 (Fig. 1B): ARDS (DAD pattern) occurred in a 73-year-old man who received the first dose of ChAdOx1 nCoV-19 vaccine. Chest CT revealed extensive bilateral GGOs with consolidations. There were no abnormal findings in the lung parenchyma on chest CT performed 10 months prior. BAL fluid analysis revealed Np 29%, Lp 32%, Eo 2%, and Mq 37%. The interstitial lesions gradually improved with steroid treatment.
Patient #7 (Fig. 1D): A rapidly progressive DAD pattern was observed after primary BNT162b2-mRNA vaccination in a 51-year-old woman. Chest CT showed diffuse bilateral GGOs, centrilobular nodules, bronchovascular bundles, and interlobular septal thickening, but no cardiomegaly (8 days after vaccination). Small bilateral pleural effusions were present, but not shown in the current figure. BAL fluid analysis revealed Np 0%, Lp 92%, Eo 7%, and Mq 1%. Methylprednisolone was initiated at 90 mg/day; rapid clinical and radiological improvement was observed.
Patient #9 (Fig. 1E): An 80-year-old woman was diagnosed with HP following mold exposure 2 years prior. She changed her living accommodations and received corticosteroid therapy for 3 months resulting in complete remission, and was relapse-free after discontinuation of steroids. Cough with sputum production developed 7 days after BNT162b2-mRNA vaccination, and chest CT showed recurrence of centrilobular nodules, GGOs, and a mosaic pattern of HP. She improved with steroid treatment and is without recurrence even after discontinuation of steroids.
Patient #11 (Fig. 1F): Acute exacerbation of IPF was observed in an 80-year-old man who received BNT162b2-mRNA vaccine (first dose). He discontinued pirfenidone 1 year before vaccination due to adverse skin reactions and anorexia. Four days after COVID-19 vaccination, chest CT revealed new bilateral GGOs superimposed on reticular opacities and honey-combing with spontaneous pneumothorax. The patient improved with steroid treatment and chest tube management and was discharged with no acute exacerbation thereafter.
Differential diagnosis process
We evaluated the differential diagnoses and potential other triggers of ILD. Various laboratory tests were performed to rule out infectious lung disease; all of the results were negative (Supplementary Table 2). The following clinical features support the diagnosis of CV-P. No patients had upper respiratory symptoms, such as a runny nose and sore throat, suggestive of viral infection. In macroscopic bronchoscopy findings, there was no purulent secretion or diffuse bronchitis, suggestive of infectious etiologies. Cell differential counts of BAL fluid in five cases showed lymphocytic or eosinophilic inflammatory patterns. The procalcitonin level was low compared to extensive radiologic lesions. Since most patients improved rapidly with steroid treatment, it was strongly suggested to be an inflammatory lesion rather than an infection. From an epidemiologic point of view, the incidence of seasonal respiratory viral infections significantly decreased in Korea during the COVID-19 pandemic [17,18].
Autoantibody tests were performed to differentiate rheumatic diseases (Supplementary Table 2). Patients who tested positive for any autoantibodies consulted with a rheumatologist; however, none were suspected or met the diagnostic criteria for autoimmune disease. None of the patients showed dry eye, dry mouth, arthritis, or Raynaud’s phenomenon. During the outpatient follow-up after the discontinuation of steroids, no additional clinical findings suitable for rheumatic diseases were observed. No patients were exposed to novel environments, inhaled antigens, or inorganic particulate matter. Patients with underlying conditions were taking medications with no recent changes. Patients maintained these medications during and after the course of CV-P (Supplementary Table 4). In addition, there were no other triggers of ILD exacerbation, such as aspiration events or surgical procedures.
DISCUSSION
In all patients, the only newly administered agent before CV-P onset was the COVID-19 vaccine, which shows a clear temporal relationship. Other diseases causing lung infiltration were methodically ruled out [10]. We identified various manifestations of CV-P ranging from transient pulmonary infiltrates with mild symptoms to life-threatening ARDS, as well as aggravation of underlying ILD. The findings of the present cases are similar to those of previously reported cases of pneumonitis associated with influenza vaccines and novel cancer therapies [8,9], suggesting that pathogenic mechanisms might vary.
Although the pathophysiology in the current cases remains unclear, there are several noteworthy findings. First, we found lymphocytic alveolitis (32%–92%), either pure or associated with eosinophilic inflammation (2%–32%), from the BAL fluid in five patients with de novo CV-P. As a potential mechanism, an aberrant innate immune response to a vaccine molecule (e.g., mRNA) may be considered in individuals with a specific immunogenetic predisposition [19]. Another mechanism is molecular mimicry, in which the antibody against the spike protein of SARS-CoV-2 has cross-reactivity with human tissue antigens [20]. The rate of antinuclear antibody positivity reported herein was higher than what is expected among the general population [21]. Although this finding could be incidental, a heightened immune response after vaccination in patients with potential autoimmune diathesis may play a role. Autoantibodies are being evaluated as potential mechanisms for various AEs following COVID-19 vaccination, including myocarditis, thrombosis with thrombocytopenia syndrome, and glomerulonephritis [3,22,23].
Second, three patients with underlying ILD developed CV-P. In previous studies, pre-existing ILD was a risk factor for drug-induced lung toxicity, including that of immune checkpoint inhibitors [12,24]. CV-P with pre-existing ILD was milder than a typical ILD exacerbation in terms of symptoms, laboratory findings, and radiological extent. Additionally, these patients improved with lower doses of corticosteroids than those with de novo CV-P. However, this could be due to selection bias, as patients with underlying ILD might undergo imaging evaluation more frequently, even with milder symptoms.
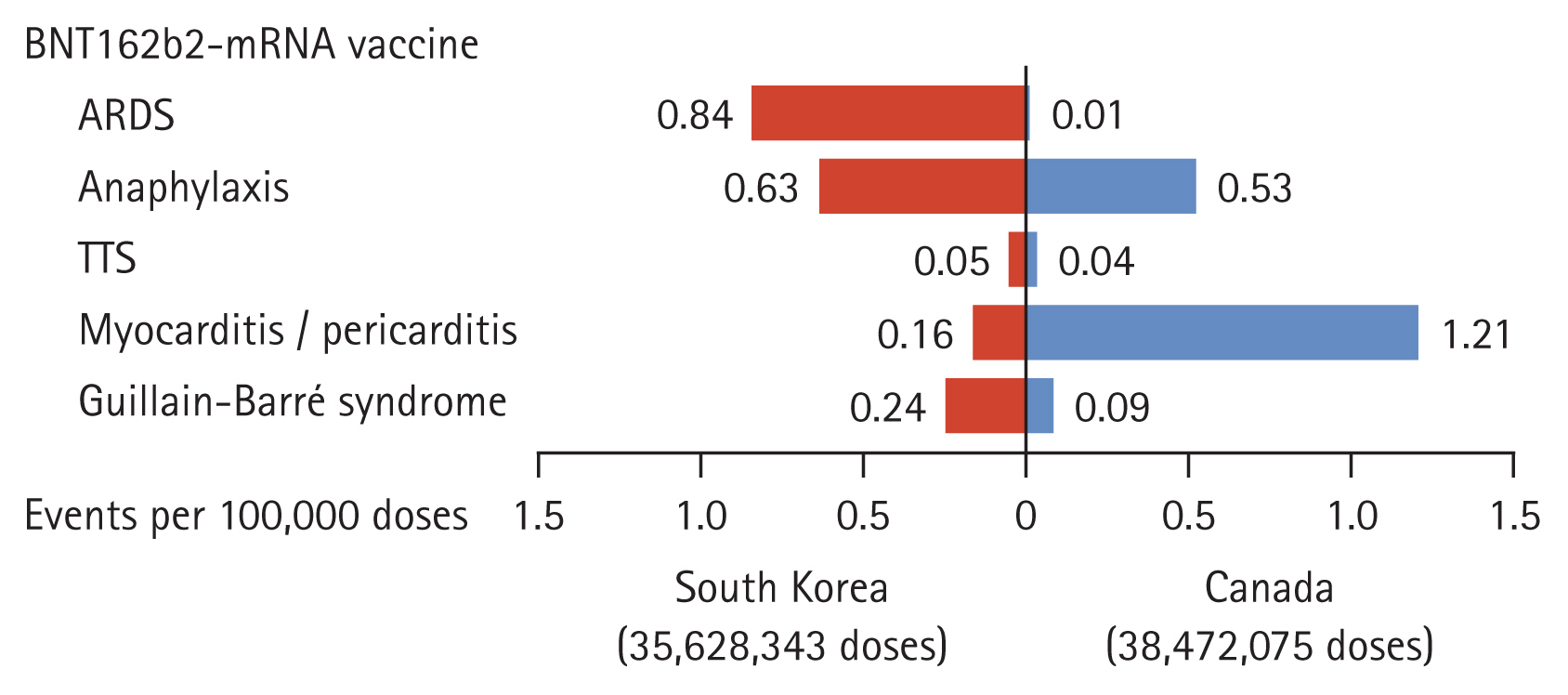
Fig. 2 shows the national data of reported AEs after the BNT162b2-mRNA vaccinations in South Korea and Canada. As both reports are based on passive surveillance, there is a significant likelihood of under-reporting and biases; nevertheless, the frequency of reporting ARDS in South Korea is much higher than that in Canada. Differences in ethnicity should be considered; however, the differences might also be because the vaccine was first administered to the elderly in South Korea. Old age has been reported as a risk factor for drug-related pneumonitis [24]. However, these hypotheses and causality cannot be proven by our limited report. Therefore, active surveillance through prospective cohorts in different populations is necessary for evaluating the incidence, prognosis, and risk factors for CV-P.
We found 12 cases of CV-P in previously published reports through a review of the literature (Table 4) [25–33]. Eleven patients developed CV-P after receiving the BNT162b2-mRNA vaccine and one after receiving the first dose of the Ch- AdOx1 nCoV-19 vaccine. The median age of these patients was 65 years, and 11 were male. The date of symptom onset was median 2 days after the most recent vaccination. Among the cases, seven were smokers, and four had underlying ILD. Fever and shortness of breath were the most common symptoms. The cell differential counts of BAL fluid reported in five cases showed a lymphocytic or eosinophilic inflammatory pattern. Although two patients spontaneously improved without medication, all other cases were treated with corticosteroids. The outcome of all reported cases was favorable. There were no unique diagnostic findings in these reported cases, but the clinical features and imaging findings are similar to our current case series. Most patients show bilateral GGO infiltration with or without interlobular thickening. The symptoms and pulmonary parenchymal lesions did not respond to antibiotics; however, they responded to systemic corticosteroids. In particular, it is characteristic that most CV-P cases developed after BNT162b2-mRNA vaccination.
The limitations of this study are as follows. First, we could not directly prove the definitive pathophysiology of CV-P. However, we reached the diagnosis through extensive differential diagnosis processes and multidisciplinary discussion. We also hypothesized a pathologic mechanism and identified a therapeutic response that was non-specific but commensurate with our hypothesis. Second, the possibility of idiopathic exacerbations of pre-existing ILD could not be absolutely ruled out. In general, acute exacerbations of ILD may be triggered or idiopathic. In patients classified as idiopathic, it is not clear whether there is an undiscovered intrinsic factor or inciting event (external factor) has not been found [34]. We meticulously ruled out other possible triggers. All CV-P cases being stable without additional measures after complete steroid treatment might be indirect evidence that the vaccines have been the trigger. In the patient with de novo CV-P, we confirmed that there was no underlying ILD through previous chest radiologic images. Third, although extensive evaluations were performed on most patients to differentiate infections, not all identical tests were performed on all patients; the tests were selected according to the attending physician’s judgment. In patients who missed specific tests, we determined that the corresponding infection was unlikely by evaluating other clinical parameters (symptoms, laboratory tests, radiologic tests, and clinical course).
In conclusion, although rare, reports of pneumonitis related to the new COVID-19 vaccine continue to increase and should be defined as an ‘AE of special interest’ with continuous safety monitoring. Clinicians should have a high index of suspicion in patients who develop atypical pneumonitis after vaccination without any specific etiologies. However, COVID-19 vaccination, including booster doses, must be continued as the expected benefits far outweigh the risks. For safe administration of these vaccines, further investigation to elucidate the association of these vaccines with lung toxicity is required.
KEY MESSAGE
1. We identified various patterns of coronavirus disease 2019 (COVID-19) vaccine-related pneumonitis (CV-P), including transient infiltration, life-threatening acute respiratory distress syndrome, and aggravation of underlying interstitial lung disease.
2. Most patients with CV-P showed favorable outcomes with good responses to systemic corticosteroid
The potential pulmonary toxicities of COVID-19 vaccines are very rare; however, clinicians should consider the differential diagnosis for patients with atypical lung infiltration without specific etiologies.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





