


A 23-year-old male presented with exertional chest pain that began a month prior. He had undergone patent ductus arteriosus closure in the neonatal period and exhibited no significant findings on physical examination except for a shallow chest cavity.
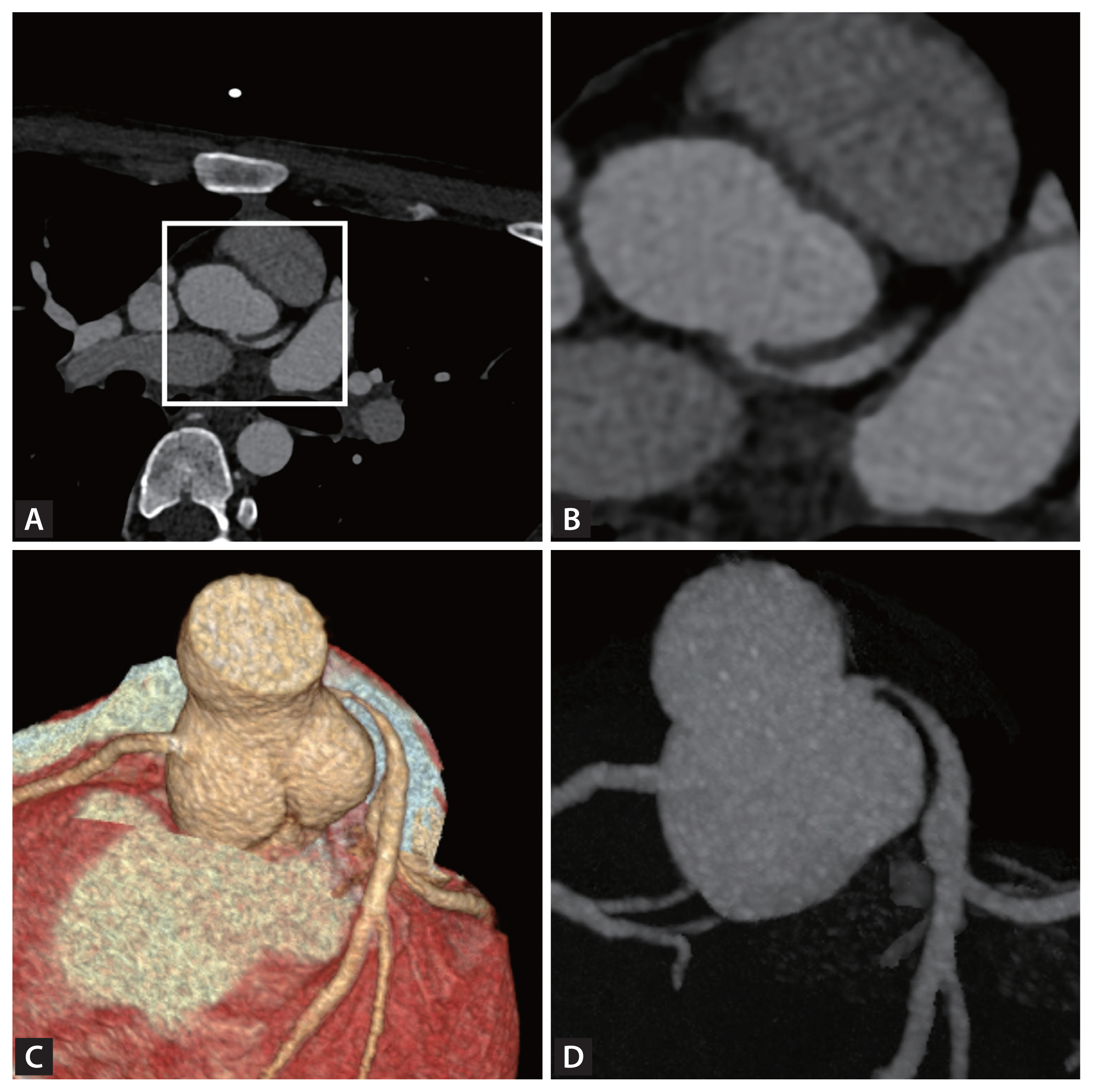
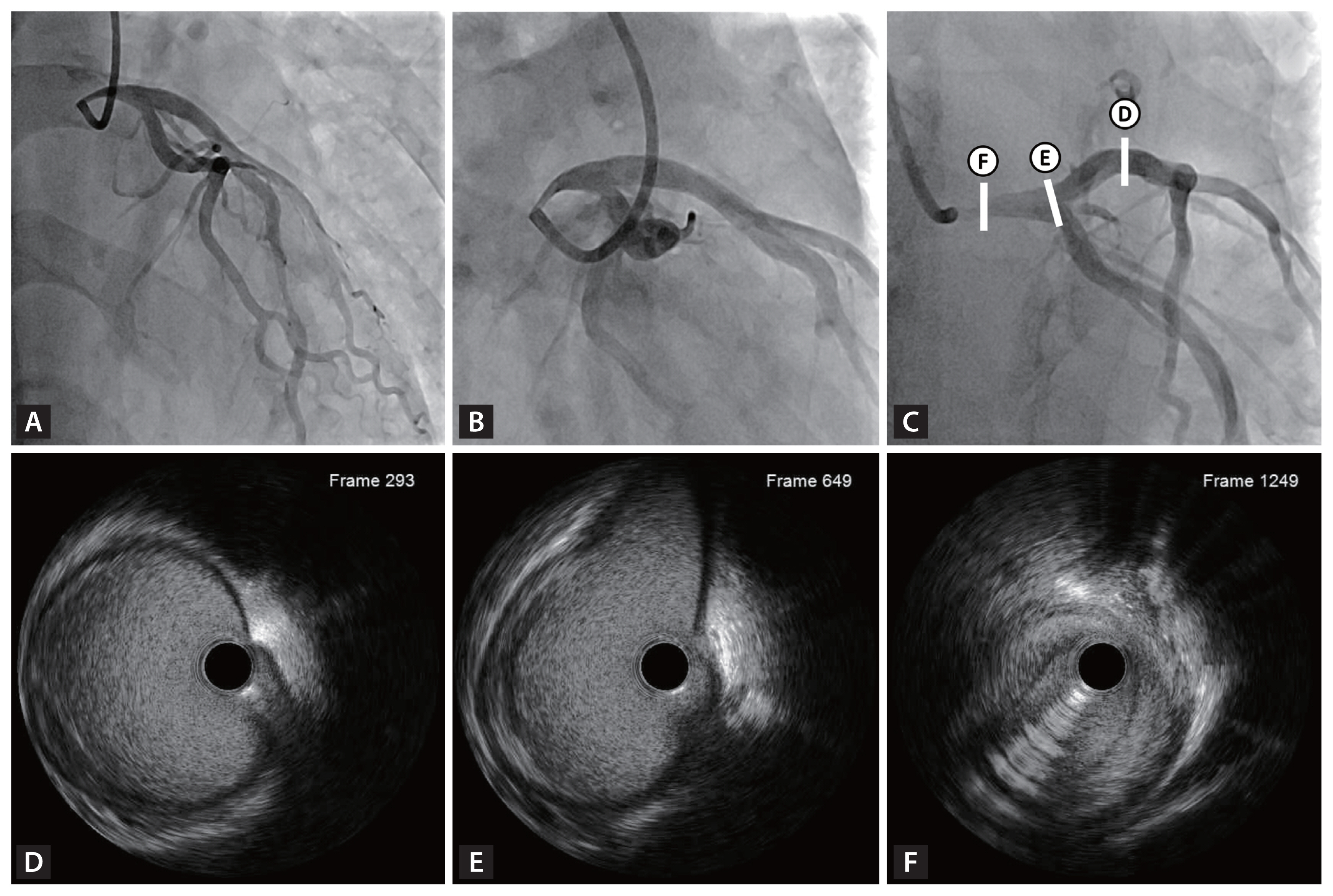
Electrocardiography and echocardiography results were within normal limits. However, cardiac computed tomography angiography revealed significant left main coronary artery (LMCA) stenosis due to an acute angle and relatively high takeoff of the LMCA, coursing between the aorta and pulmonary trunk (Fig. 1, Supplementary Video 1). Subsequent coronary angiography confirmed significant LMCA stenosis, and intravascular ultrasound demonstrated gradual narrowing of the proximal vessel lumen compared to distal reference, suggesting extrinsic compression rather than plaque accumulation. (Fig. 2). Considering the patient’s overall clinical assessment and multimodal imaging findings, he underwent coronary artery bypass graft surgery and recovered uneventfully.
Coronary compression due to unfavorable anatomy has been associated with anomalous aortic origin of a coronary artery [1–3]. While uncommon, this condition can manifest as exertional chest pain in adolescence and can lead to coronary compromise, including sudden cardiac death [1–3]. Although this case does not fit within the category of congenital anomaly, it shares anatomical characteristics affecting the takeoff and course of the LMCA. Furthermore, LMCA compression, though extremely rare, is clinically significant. Therefore, in young patients with exertional chest pain, early imaging is crucial to distinguish extrinsic vascular compression from primary coronary artery disease and to guide appropriate management.
Informed consent was obtained from patients.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement video 1
Supplement video 1 Print
Print





