


INTRODUCTION
The number of older patients presenting with glomerular disease is growing with the increasing average lifespan [1]. Membranous nephropathy (MN) is the most common diagnosis of primary glomerular disease in older patients with a nephrotic syndrome and has a prevalence higher than that in younger adults [2]. Most MN in older patients has an idiopathic cause and the accuracy of diagnosis has been improved with the increasing trend towards performing renal biopsies [3]. Therefore, in an aging population, idiopathic MN is a major component of kidney disease in older patients. The associated morbidity and mortality has attracted attention to the clinical outcomes of MN in this population [4].
The natural history of the disease is often benign; those with non-nephrotic-range proteinuria invariably presents good prognosis in that they are responsive to symptomatic management including angiotensin receptor blockers (ARBs) and diuretics, thereby achieving spontaneous complete remission (CR) [5,6]. However, the 25% to 50% of patients presenting with heavy, persistent proteinuria, progressive renal functional deterioration, and unfavorable histological alterations are associated with poor clinical outcomes and may reach end-stage renal disease (ESRD) [7,8]. In these patients, the use of immunosuppressive agents may be justified to salvage failing kidneys and even for patient survival. However, little information is available about their outcomes because physicians are reluctant to use an aggressive treatment that may compromise the residual reservoir of already aged kidneys [9-11]. Therefore, information about the clinical outcomes of older patients compared with those in younger adults is vague and appropriate treatment modalities need to be determined and targeted to this aging population.
This study aimed to investigate the clinical characteristics of idiopathic MN in older patients. We explored the influence of older age on the clinical course and treatment responses of idiopathic MN in comparison with those in younger patients. In addition, we compared the complication rates associated with different treatment modalities in older and younger patients.
METHODS
Study population
We included patients with idiopathic MN who were treated at two medical centers of the Catholic University of Korea (Seoul and Daejeon St. MaryŌĆÖs Hospitals) from September 1998 to August 2016. Patients with histologically proven MN were screened and those with potential secondary causative factors were excluded by: clinical history with regard to possible drug use; serologic tests for both infectious and connective tissue diseases including serum autoantibodies, such as antinuclear antibody, anti-double-stranded DNA antibody, anti-neutrophil cytoplasmic antibody, and rheumatoid factor and complement; and screening for hepatitis B and hepatitis C viruses. Patients who had associated malignancies at presentation were also excluded from the study. Thorough clinical examination and appropriate laboratory screening excluded those with secondary causes for MN, leaving 135 patients diagnosed with idiopathic MN. We classified the study participants into ŌĆśolderŌĆÖ and ŌĆśyoungerŌĆÖ groups, where ŌĆśolderŌĆÖ was defined as 60 years of age or older at the time of the renal biopsy [9,10].
Data collection and definitions
Data for age, sex, laboratory test results, treatment modalities, clinical responses to treatment, progression to ESRD, occurrence of infection, and patient survival were collected. Body mass index was calculated as the ratio of weight in kilograms divided by the square of the height in meters. Estimated glomerular filtration rate (eGFR) was determined from serum creatinine concentration, age, sex, and race using the abbreviated Modification of Diet in Renal Disease (MDRD) formula [12]. Protein concentration in a 24-hour urine sample or the protein-creatinine ratio of spot urine was used to estimate the amount of proteinuria. Treatment modalities were classified into four groups: conservative treatment, corticosteroids alone (at least 50 mg prednisone/day), cyclophosphamide with or without steroids (less than 15 mg prednisone/day), or cyclosporine with or without steroids (less than 15 mg prednisone/day).
Renal biopsy specimens were examined by light microscopy, immunofluorescence microscopy, and electron microscopy. Sections (2 ╬╝m) stained with hematoxylin and eosin, MassonŌĆÖs trichrome, periodic acid-Schiff, and periodic acid-silver methenamine were examined by light microscopy. The number of global or segmental sclerotic glomeruli is presented as the percentage of the total number of glomeruli in the biopsy specimen. The degree of tubular atrophy was graded from 0 to 3 (mild, moderate, and severe). Interstitial fibrosis was graded as follows: grade 0, none; grade 1, < 25%; grade 2, 26% to 50%; and grade 3, > 50%. Cryosections (4 ╬╝m) were stained with fluorescein isothiocyanate-conjugated rabbit anti-human immunoglobulin G (IgG), IgA, IgM, ╬║ and ╬╗ light chains, and complement 3 (C3), C4, and C1q.
Outcome measures
The primary endpoint was treatment response, which was assessed as CR, partial remission (PR), or no response (NR). CR was defined as urinary protein excretion less than 300 mg/day and stable serum creatinine level. PR was defined as urine protein excretion less than 3.5 g/day or less than 50% of baseline proteinuria with stable serum creatinine level. NR was defined when urinary protein excretion remained at over 50% of the baseline value or serum creatinine level progressively increased [4,13,14]. The secondary endpoints were progression to ESRD, the occurrence of infection and patient death. Development of infection was defined as such that required hospitalization. ESRD was considered a prerequisite for renal replacement therapies such as maintenance dialysis and kidney transplantation.
Statistical analysis
Variables are presented as the mean ┬▒ SD or as frequencies (percentage). Continuous variables were compared using StudentŌĆÖs t test, and categorical variables were compared using a chi-square test or FisherŌĆÖs exact test. To test for an independent association of older age and the occurrence of endpoints, a Cox proportional hazards model was used. Such variables that were deemed clinically significant (i.e., the presence of hypertension, proteinuria, treatment modality, and hemoglobin level) were entered into multivariate Cox regression analyses along with variables of p value less than 0.1 in univariate analyses. The cumulative event rates for the prespecified endpoint were estimated by the Kaplan-Meier method and compared using log-rank tests. A p < 0.05 was considered significant. Statistical analysis was performed using SPSS software version 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics of older and younger patients with idiopathic MN
A total of 135 patients included 77 men (57%) and 58 women (43%). The mean age was 53.7 ┬▒ 14.4 years. Eighteen (13%) and 41 patients (30%) had diabetes and hypertension, respectively. The mean eGFR was 99.0 ┬▒ 41.9 mL/min/1.73 m2 and 19 patients (14.1%) had eGFR less than 60 mL/min/1.73 m2. The amount of proteinuria ranged from 0.02 to 18.02 g/day and patients with nephrotic range proteinuria (> 3 g/day) accounted for 103 (76%). Of these patients, 48 (36%) were treated conservatively with the use of ARBs, while 87 patients (64%) were assigned to treatment with immunosuppressive agents.
A greater proportion of older patients than of younger patients had hypertension. Compared with younger patients, older patients presented with lower eGFR. There were no significant differences in serum albumin level, lipid profiles, and the amount of proteinuria. The proportion of those with nephrotic range proteinuria was more prevalent in the older group. The biopsy findings in older patients demonstrated unfavorable histologic changes (Table 1).
Comparison of clinical outcomes between older and younger patients with idiopathic MN
In the older patient group, 18 (33.3%) achieved CR, 14 (25.9%) had PR, and 22 (40.7%) had NR. Younger patients had significantly more favorable responses to treatment than older patients did (CR 61.7%, PR 11.1%, NR 27.2%, p = 0.004). The cumulative event rate for achieving CR was significantly inferior in older patients compared with younger patients (p = 0.012) (Fig. 1A). Compared to younger patients, older patients with nephrotic range proteinuria achieved less CR (30.4% vs. 54.4%, p = 0.013) and those with non-nephrotic range proteinuria had more NR (50.0% vs. 8.3%, p = 0.026).
Two deaths (3.7%) occurred in the older patient group (p = 0.158 vs. younger patients). The cumulative event rate for requiring renal replacement therapy was significantly higher in older patients (p = 0.015) (Fig. 1B). Older patients had a greater risk of infection and a significant difference was observed between the age groups in the development of infection (p = 0.005) (Fig. 1C).
Older age is an independent predictor of CR and infection
Univariate Cox proportional hazard models showed that older age and male sex decreased the odds ratio (OR) for CR and an increased eGFR was positively associated with CR from proteinuria (Table 2). After adjusting for clinically relevant factors, older age and male sex remained as significant predictors of a reduced chance of CR from proteinuria. Both univariate and multivariate models revealed older age as a robust predictor of the development of infection. In univariate models, older patients had a significantly greater risk of progression to ESRD (OR, 10.91; 95% confidence interval [CI], 2.11 to 56.36; p = 0.004), but this association was not significant in multivariate models (adjusted OR, 2.08; 95% CI, 0.26 to 16.47; p = 0.486).
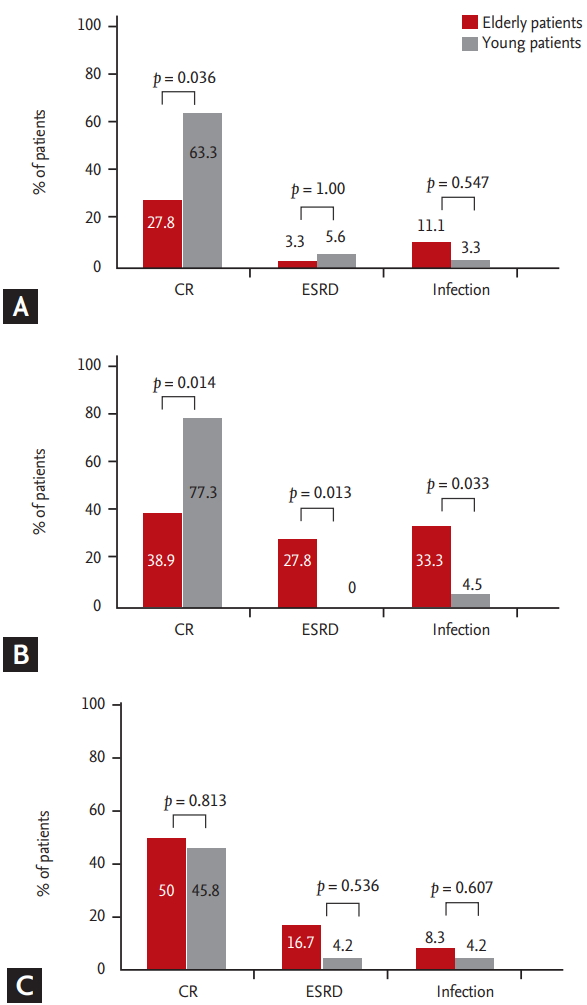
Comparison of clinical outcomes in older and younger patients based on treatment modalities
The effectiveness of different treatment strategies in older and younger patients was analyzed in terms of CR attainment, development of ESRD, and infection. Conservative treatment was associated with a significantly lower remission rate in older patients (Fig. 2A). No significant differences were observed between the age groups in terms of renal progression and occurrence of infectious complications in patients managed with conservative treatment. Corticosteroid treatment was less effective in the older patient group (n = 18) in achieving CR and preventing progression to ESRD, and moreover was associated with a greater frequency of infectious complications (Fig. 2B) than in the younger patient group (n = 22). Cyclosporine showed comparable effectiveness for achieving CR and in preventing renal functional deterioration and infectious complications between older and younger patients (n = 12 and n = 24, respectively) (Fig. 2C). The number of patients treated with cyclophosphamide was limited, but this treatment was associated with comparable rates of CR (50.0% vs. 80.0%, p = 0.545) and infectious complications (16.7% vs. 0.0%, p = 1.00) in older and younger patients (n = 6 and n = 5, respectively).
DISCUSSION
Our study demonstrated that older patients with idiopathic MN had a lower CR rate, higher rates of progression to ESRD, and greater frequency of infectious complications than younger patients. Of the treatment modalities, conservative treatment was less effective in achieving CR in older patients and corticosteroid therapy had less clinical benefit. These findings suggest that older patients with idiopathic MN have an unfavorable clinical course compared with that of younger patients and that treatment modalities affect the outcomes of older patients differently from younger patients.
The commonest manifestation of idiopathic MN is nephrotic syndrome with preserved kidney function [15,16]. The clinical presentation of older patients is not so much different from that of younger adults in that heavy proteinuria with the presence of edema is the most prominent finding at the time of renal biopsy [17], which is consistent with the results of this study because both patients had heavy proteinuria and comparable levels of serum cholesterol and albumin. However, these older patients had a significantly lower eGFR and a higher prevalence of hypertension, with a greater proportion of glomerular sclerosis and more severe grades of tubular atrophy and interstitial fibrosis on renal biopsies. These findings suggest that older patients are predisposed to a higher risk of progression to ESRD than younger patients, despite the similar initial clinical presentation of idiopathic MN in the two groups.
In the present study, we found that older patients showed a lower rate of CR than younger patients did, and that age was independently associated with an inferior CR rate. In addition, a higher rate of progression to ESRD was observed in older patients, although the treatment modalities and the frequency of their use were similar to those of younger patients. These findings suggest that treatment response is significantly inferior in older patients than in younger patients. Contemplating on the reasons for poorer treatment response in the older group, we suggest that the higher proportion of those with nephrotic-range proteinuria at presentation may contribute to lower treatment response. Moreover, it is presumed that appropriate timing for the initiation of immunosuppressive agents may have been delayed in the older group (data not shown; 0.9 ┬▒ 2.2 months vs. 5.8 ┬▒ 18.0 months, p = 0.057). These findings suggest that treatment strategy for dealing with older patients needs to be more active than current clinical practice.
Older patients demonstrated greater cumulative event rates for the development of infection. In addition, time to the occurrence of infectious complications was more extended than that of younger patients (data not shown; 34.0 ┬▒ 36.4 months vs. 5.7 ┬▒ 5.0 months, p = 0.038). Among a total of 36 elderly patients who had taken immunosuppressant, eight developed infectious complications. Four of them developed infection while on drugs, and the other four showed signs of infection after finishing the intake of immunosuppressive agents. These results suggest that elderly patients were at higher risk for infection than younger patients and that cautious observation is necessary even after the patient have finished the prescribed dose of immunosuppressant.
About 50% of idiopathic MN patients with persistent high-grade proteinuria eventually progress to ESRD and aggressive therapy is usually initiated in this context [18]. The present study suggests that because older patients were associated with poorer renal outcomes with respect to increased event rates for renal replacement therapy, these patients should be eligible to receive aggressive treatment regimen to preserve renal function. However, our study also demonstrated that older patients are exposed to greater risks of infectious complications during treatment [13]. These findings suggest that an aggressive treatment strategy should be individualized in older patients to balance the risks and benefits of treatment.
The natural history of idiopathic MN in older patients is often benign, with some individuals eventually experiencing spontaneous remission of nephrotic syndrome [19]. Therefore, it is reasonable to prefer conservative treatment in older patients when we consider their higher potential risk of infectious complications. In this study, while symptomatic treatment resulted in comparable rates of infectious complications and ESRD progression in older and younger patients, CR was achieved in only 20% of older patients, which was significantly lower than the rate in younger patients. These findings suggest that conservative treatment was ineffective in achieving CR in older patients and that immunosuppressant should be considered as a treatment option in this context. We suggest that conservative treatment is effective in those with a high risk of infectious complications or with limited lifespan that reduces their risk of developing ESRD [20].
Several randomized trials have failed to demonstrate the efficacy of glucocorticoid monotherapy in the treatment of idiopathic MN, despite early encouraging studies involving patients of Asian ancestry that reported its potential benefit [21-23]. Our study demonstrated that corticosteroid treatment in older patients was associated with unfavorable clinical outcomes including lower CR rates and greater risks of progression to ESRD and development of infectious conditions compared with younger patients. These findings confirm that corticosteroid monotherapy has limited value as a treatment option in older patients and that it is associated with a higher complication rate [15,24,25]. In contrast, cyclosporine use showed comparable results in older and younger patients with respect to achievement of CR, progression to ESRD, and occurrence of infectious complications. On these grounds, we cautiously infer that cyclosporine may produce comparably favorable outcomes for renal aspects and therefore, it may be considered an alternative first-line treatment option for older people who are vulnerable to infections.
Our study has limitations. First, it was based on retrospective data analysis. Treatment modality was not standardized; rather it was based on an individual practitionerŌĆÖs decision depending on patientsŌĆÖ clinical setting. Therefore, there are unmeasured biases in evaluating primary and secondary outcomes. Second, patients clearly were not randomized to immunosuppressive modalities, and potential confounders may exist. We adjusted for relevant key clinical parameters in the analyses, but there may be factors influencing treatment decisions that were included in our models. Therefore, prospective randomized controlled studies are required to compensate for these flaws. Third, we could not evaluate the effect of mycophenolate mofetil owing to insurance policy, and no patients received the cyclic therapy of corticosteroid and cyclophosphamide.
In conclusion, older age in patients with idiopathic MN was associated with an inferior clinical course and worse treatment responses. The achievement of CR, progression to ESRD, and occurrence of infectious complications for each treatment regimen was significantly altered in older patients compared with younger patients. The use of corticosteroid therapy was associated with minimal clinical benefit, but cyclosporine treatment is predicted to have the potential to lead to a better prognosis. Therefore, our study provides valuable information that helps to improve the clinical outcomes in older patients with idiopathic MN.
KEY MESSAGE
1. Cumulative event rate for achieving complete remission was inferior and that for requiring dialysis, and infection was higher in older patients.
2. Old age per se was independently associated with inferior clinical outcomes in patients with idiopathic membranous nephropathy.
3. Cyclosporine treatment is predicted to be more useful than corticosteroids in older patients

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





