


INTRODUCTION
Osteoporosis is approximately two times more prevalent in patients with rheumatoid arthritis (RA) than in the general population, and RA is associated with a higher probability of fractures [1]. This is thought to be related to accelerated bone resorption by systemic and local inflammatory reactions, reduced bone formation resulting from glucocorticoid use, and limited exercise and activity owing to inflamed joints [2]. Patients with RA have lower bone mineral density (BMD) and a higher probability of bone fractures than the general population when matched for age, gender, and BMD [3]. In Korea, the Health Insurance Review Agency (HIRA) identifies patients eligible for treatment using a simplified method based on a minimum T-score (-3.0) on a BMD examination or radiographic evidence of osteoporotic fractures [4]. The fixed T-score-dependent threshold for intervention is a simple and easy method for making national reimbursement decisions, but it may not provide timely preventive intervention for the high-risk group of patients with RA. Furthermore, the difference in T-score threshold criteria between HIRA and the World Health Organization (WHO) further confuses the issue. The HIRA classification is based on a minimum T-score measured at any lumbar or femur site, and identifies different treatment populations than the method recommended by the International Society for Clinical Densitometry (ISCD), which designates the total lumbar, femur neck, or total femur as proper sites for BMD measurement [5].
Clinical risk factors are important predictors of the probability of fragility fractures independent of BMD; thus, the WHO developed the FRAX® tool to assess the 10-year probability of fracture. It is based on a large-scale, worldwide epidemiological study that included the United Kingdom, United States, Australia, Japan, and China [6]. This tool, which became available online in 2008, is based on clinical risk factors, with or without femur neck BMD measurement, and the outcome is the probability of major osteoporotic or hip fractures in individual patients in the next 10 years if not treated [7]. The WHO did not define the threshold for pharmacological intervention based on FRAX probabilities, but recommended that the treatment threshold should be defined by individual patients or national circumstances. When no precise epidemiological model is available, the WHO recommends use of the most relevant model from similar racial or geographic groups. In the United States, the National Osteoporosis Foundation (NOF) revised its guidelines in 2008 and recommended pharmacological intervention for patients with low bone mass if the FRAX probabilities were over a specific threshold and for a previously identified population with defined osteoporosis or prior osteoporotic fractures [8].
The present study aimed to determine the prevalence of osteoporosis in Korean patients with RA using a standard BMD examination and to compare the Korean guidelines for osteoporosis treatment in patients with RA with those of the FRAX tool. In addition, we investigated the difference in the treatment populations identified using the HIRA, NOF, and FRAX tool with specific thresholds of risk as defined in this study.
METHODS
Patients
In this cross-sectional epidemiological study, 234 consecutive patients with seropositive RA were recruited from a single regional rheumatism center in Korea between March and May 2010. The patients fulfilled the American College of Rheumatology (ACR) criteria for the diagnosis of RA with serological evidence of rheumatoid factor. To maintain an appropriate comparison, the patients were postmenopausal women or men > 50 years of age as specified by the FRAX and NOF guidelines [5,7,8]. Only patients with BMD examination results available within 1 year from the time of recruitment were included in the study. The time period between serial BMD examinations is usually more than 1 year as recommended by the ISCD and Korean HIRA; thus, we enrolled patients who had a BMD examination within 1 year from the time of recruitment to prevent unnecessary EXCLUSION.
Data collection
General characteristics including age, gender, body weight, and height were collected by reviewing medical charts. Patient interviews conducted by a physician provided a history of osteoporotic fractures including the hip, vertebrae, proximal upper arm, and distal forearm; a parental history of hip fracture; smoking status; and alcohol use status. The physician determined the presence or absence of each risk factor according to the FRAX criteria. Glucocorticoid use was considered to be a risk factor if the patient had a history of taking > 5 mg of a prednisone-equivalent dose of glucocorticoids daily for > 3 months. X-rays of the thoracic and lumbar vertebrae were reviewed to reveal morphometric vertebral fractures. Disease duration was calculated from symptom onset time to the date of recruitment rather than from the date of diagnosis because several patients were referred to our rheumatism center with time gap between the date of diagnosis and the actual onset of RA.
BMD interpretation
The BMD examination results were reviewed according to the ISCD guidelines. Secondary changes in the lumbar area (L1 - L4) that produce false BMD measurements, such as degenerative sclerotic changes, the presence of osteophytes, aortic calcifications, collapsed compression fractures, and lumbar prosthesis were discarded from the data [5,8]. The total lumbar and lumbar minimum T-scores were recorded following these exclusions. If only one vertebra remained after the exclusions, the total lumbar T-score was considered to be missing, but the minimum Tscore was recorded based on that vertebra. The same exclusion method was used for the femur neck, trochanter, intertrochanter, and Ward's triangle, and then the T-scores of the femur neck, total femur, and femur minimum were recorded. For Koreans, the FRAX requires only raw BMD data from the femur neck (g/cm2) with the name of the manufacturer, instead of the T-score. A fan-beam dual X-ray absorptiometry unit (DXA, QDR-4500A; Hologic Inc., Bedford, MA, USA) was used to measure BMD. The default diagnostic threshold for osteoporosis was a T-score calculated from gender-matched BMD data in young Asian adults derived in Japan [9]. After acquisition of the BMD T-score, the patients were classified as having osteoporosis if the T-score of the total lumbar, femur neck, or total femur was Ōēż -2.5 [10]. To determine the most prevalent site of osteoporosis in patients with RA at the time of the examination, lumbar and femur osteoporosis were determined separately.
FRAX tool application
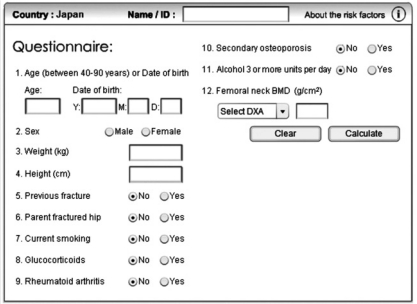
No Korean epidemiological data for the FRAX application are available; thus, we used the FRAX tool on the Internet using a Japanese model (Fig. 1) [7]. We used BMD raw data rather than the T-score and entered individual patient values and clinical risk factors with or without femur neck BMD measurements. Because our study population was patients with RA, the presence of secondary osteoporosis did not have an additional effect on the risk estimation. The output, 10-year probability of major osteoporotic and hip fracture with or without BMD data, was recorded to make a set of four probability scores for each individual. The assessment of fracture risk was performed in subgroups of age or gender. A previously defined risk threshold for osteoporosis treatment in Korea was not available; thus, we defined the threshold for pharmacological intervention as Ōēź 20% of major osteoporotic fracture probability or Ōēź 3% of hip fracture probability in the next 10 years using the FRAX tool. This was the same threshold specified by the NOF for patients with low bone mass whose T-scores were between -1.0 and -2.5.
NOF classification
In 2008, the NOF described three categories of patients eligible for pharmacological intervention [8]: patients with prior osteoporotic hip or vertebral fractures, patients classified as osteoporotic by the WHO fixed T-score-based criteria, and patients with low bone mass who had T-scores between -1.0 and -2.5 and a 10-year probability of Ōēź 20% for major osteoporotic fracture or Ōēź 3% for hip fracture. In the present study, the patients who fit any of these criteria were considered to be eligible for treatment by NOF criteria.
HIRA classification
Every Korean citizen is covered by the government National Health Insurance and their eligibility for reimbursement is reviewed by the HIRA [4]. HIRA insurance coverage for osteoporosis requires a minimum T-score of Ōēż -3.0 at any site on the lumbar or femur area, or radiographic evidence of an osteoporotic fracture.
Statistics
Dichotomous variables are expressed as the number and percentage and continuous variables are expressed as the mean and standard deviation (SD) or median and range according to the fitness in a normal distribution. Because the prevalence of osteoporosis increases with age, we also analyzed the data in subgroup patients Ōēż 59 and Ōēź 60 years of age, which was the mean and median age of our entire cohort. The prevalence of osteoporosis was calculated for the entire population and for age and gender subgroups, and a McNemar chi-square test was performed to compare the lumbar and femur areas within each group [11]. Overall and within-treatment group based on HIRA criteria, and the 10-year probability of major osteoporotic and hip fractures with or without BMD data were examined to determine the risk levels in Korean patients with RA. The difference among treatment groups classified using the HIRA, FRAX, and NOF criteria was determined using a Venn diagram to reveal the number of cases in each subset. The demographic data and risk factors of the discordant HIRA and FRAX populations were statistically compared using the Mann-Whitney U test for continuous variables or the chi-square test for dichotomous variables.
Cohen's kappa index was used to evaluate the concordance between each system for pharmacological intervention, and the grade of concordance was considered high when the kappa index was > 0.8 and good when it was > 0.6. The kappa index was used to examine the data according to age to evaluate the grade of discordance in the higher risk group of old age. The data were analyzed using SPSS version 14.0 (SPSS Inc., Chicago, IL, USA), and p < 0.05 was deemed to be statistically significant. All statistical comparisons were based on two-sided tests.
RESULTS
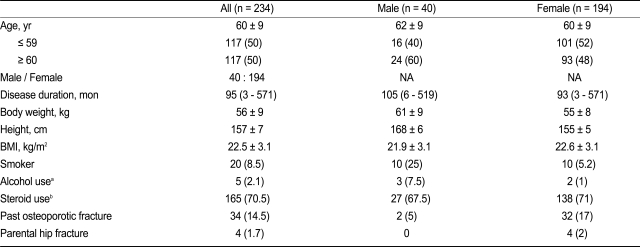
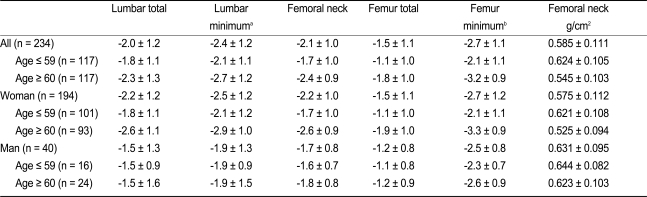
The study included 234 postmenopausal women or men > 50 years of age with seropositive RA who were recruited between March and May 2010. The patient characteristics are shown in Table 1. The mean age was 60 ┬▒ 9 years. Spinal X-rays taken within 1 year from the time of recruitment were available for 211 patients (90.2%). The study population included 40 men (17%) and 34 cases (15%) of prior osteoporotic fractures, including 32 cases of vertebral fractures and two cases of femur neck fractures. Table 2 shows the BMD T-scores for the lumbar and femur areas and a comparison of the minimum values from the entire cohort and each age and gender subgroup. The T-scores between the pair of total lumbar (L1 - L4) and lumbar minimum and between the pairs of femur neck or total femur and femur minimum were significantly different (paired t test, p < 0.001). Women had lower BMD T-scores compared to men in subgroup Ōēź 60 years of age (t test, p < 0.005), but no difference was found between women and men < 60 years of age.
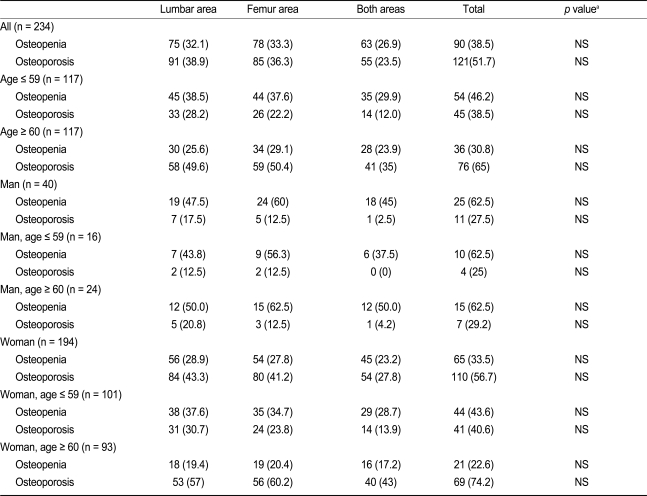
Table 3 shows the overall prevalence of osteoporosis and osteopenia in the entire cohort and in the age and gender subgroups. The results are based on the criteria of a T-score Ōēż -2.5 in the total lumbar, femur neck, or total femur, as indicated by the WHO and ISCD guidelines. Overall, 52% of the patients were classified as having osteoporosis and 39% were classified as having osteopenia. When grouped by gender, the prevalence of osteoporosis in women was 57%, but men had a prevalence of only 28%. As expected, the prevalence increased with age in women, but this relationship was not evident in men in our study, perhaps because of the small number of male patients with RA. To determine the site-specificity of osteoporosis in patients with RA, we compared individual sites of osteoporosis in the lumbar and femur areas. A McNemar chi-square test was performed to evaluate the two correlated proportions [11]. Osteoporosis was slightly more prevalent in the lumbar area than in the femur area in women < 60 years of age, but the difference was not significant (p = 0.248).
The comparison of the WHO T-score system and the HIRA minimum T-score system indicated that 110 patients (91%) among 121 patients classified as having osteoporosis according to the WHO criteria could be included in the treatment-eligible group using HIRA criteria.
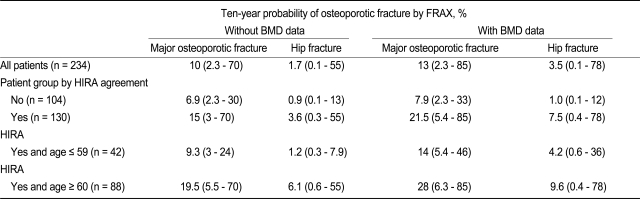
The overall median 10-year probability of major osteoporotic and hip fracture based on femur neck BMD was 13% and 3.5%, respectively (Table 4). This was higher than the probability when femur neck BMD was not evaluated. The HIRA treatment group had a median probability of 21.5% for major osteoporotic fractures and 7.5% for hip fractures.
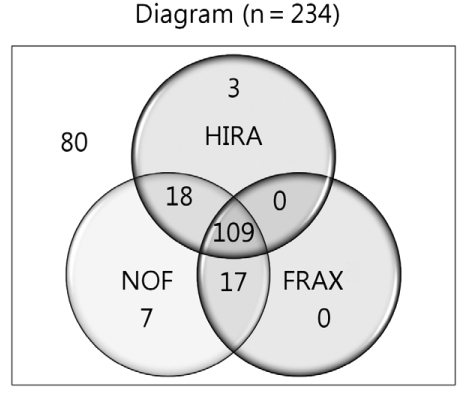
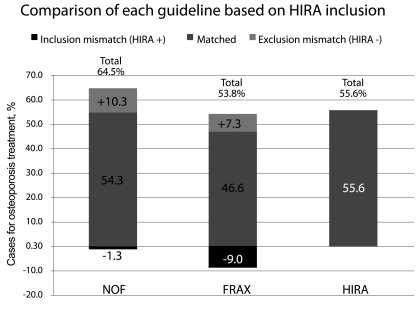
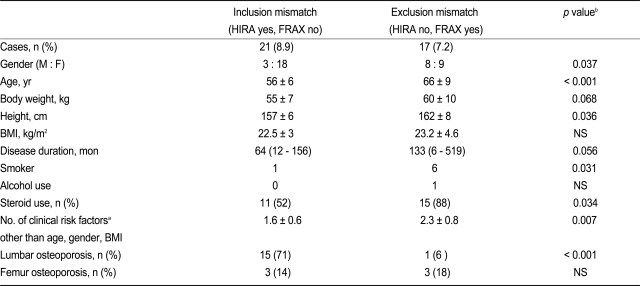
We used the HIRA and NOF criteria and the defined threshold of FRAX with BMD to classify the patients as eligible or not eligible for treatment (Fig. 2). As shown in the diagram, 109 patients (47%) were included in the treatment group by all three guidelines and 80 patients (34%) were not eligible for treatment according to all three guidelines. Fig. 3 shows the number patients eligible for treatment in the FRAX and NOF compared to those included using the HIRA criteria. The NOF criteria included the largest number of patients in the eligible for treatment group as it included 10% more patients than HIRA and excluded 1.3% of patients included by HIRA. The FRAX tool included 7.3% more patients than HIRA, but excluded 9% of the patients included in the HIRA treatment group. Thus, we found a small but significant number of discordant treatment-eligible patients based on the HIRA and FRAX criteria (n = 38, 16.3%). The characteristics of the mismatched patients in the HIRA and FRAX group are shown in Table 5. The FRAX included more patients who were older, male, cigarette smokers, steroid users, taller, and had more clinical risk factors compared to the HIRA. In contrast, the HIRA included more patients who were younger, female, had lumbar osteoporosis, and fewer risk factors. The men in our study had a higher BMD than the women, and their fracture risk was underestimated by the fixed T-score assessment of the HIRA criteria. Thus, the higher BMD in men who were excluded from the HIRA fixed T-score system permitted inclusion in the group eligible for treatment according to FRAX criteria (Table 5).
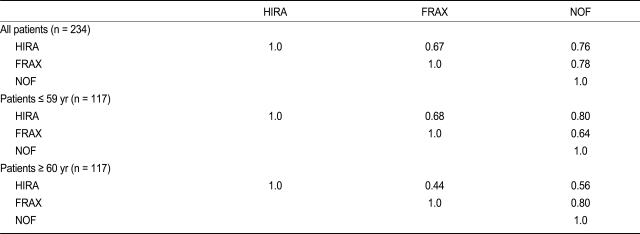
The concordance between each guideline was assessed using Cohen's kappa index. The values showed overall fair concordance (0.67 - 0.78). As expected by the differences in treatment eligibility according to each guideline, HIRA had a lower kappa index value for age > 60 years compared to the other measures (0.44 with FRAX and 0.56 with NOF; Table 6).
DISCUSSION
Our cross-sectional epidemiological study of Korean postmenopausal women and men > 50 years of age with seropositive RA found that approximately one-half of the participants were osteoporotic according to standard BMD measurements and the WHO criteria. The number of patients considered eligible for treatment differed for each set of guidelines. Several patients who had a high risk of fracture were not classified as eligible for treatment according to the fixed-T-score system used by the HIRA, but were included when the risk score system of the WHO and NOF was used.
In the present study, we selected postmenopausal women and men Ōēź 50 years of age not only because FRAX is intended for them but because the ISCD and NOF recommend BMD measurements to determine the risk of fractures in that population based on clinical profile, whereas BMD in the general population is measured only in postmenopausal women Ōēź 65 years of age or men Ōēź 70 years of age [5]. Thus, the patients in the current study may be representative of the RA population with a fracture risk that requires evaluation in daily practice.
Rheumatoid factor positivity is associated with a poor RA prognosis, and reduced bone mass is more frequently found in patients with RA who are seropositive than in those who are seronegative. One of the goals of our study was to examine the relevance of the various treatment-eligibility criteria for patients with RA at high risk for a fracture; thus, we recruited only the patients who were seropositive. Furthermore, we are satisfied that the patients enrolled in the study were homogeneous.
The prevalence of osteoporosis in patients with RA cannot be readily determined because each study population has diverse characteristics regarding age and gender, menopausal status in women, disease activity, and disease duration. Moreover, the method and the site of BMD examination are not standardized, increasing the difficulty in making direct comparisons between studies [2]. Joo et al. [12] estimated the prevalence of osteoporosis in 134 Korean patients with RA to be 13.4% (age range, 21 to 80 years). The prevalence was 28.8% in the 59 postmenopausal women included in their study. They reported 88.8% rheumatoid factor positivity compared to the 100% positivity we observed in the present study. Joo et al. [12] conducted their study prior to development of the current ISCD guidelines, and total lumbar BMD was measured only in the L2 - L4 area, excluding the L1 area. Furthermore, BMD was measured at the neck, trochanter, and Ward's triangle of the femur, which is not an indexed area according to the current WHO criteria. However, the prevalence of osteoporosis reported by Joo et al. [12] was similar to that found in another cohort in which approximately 30% of older patients or postmenopausal women were classified as having osteoporosis [2]. Clearly, additional studies on osteoporosis in Korean patients with RA are warranted. An Italian multicenter study of 925 patients with RA, of which 73% were postmenopausal women, reported the prevalence of lumbar and femur osteoporosis as 28.8% and 36.2%, respectively [1]. The Norwegian national registry cohort, thought to be free of selection bias, included 394 patients with RA between the ages of 20 and 74 years. The prevalence of osteoporosis in the lumbar and femur areas of this cohort was reported to be 16.8% and 14.7%, respectively, and when the analysis was limited to patients > 60 years of age, the prevalence was 31.5% and 28.6%, respectively [13]. The overall prevalence of osteoporosis in either the lumbar or femur area was not reported in the Norwegian study. In our study of patients with RA who were seropositive and had a mean age of 60 years, the prevalence of osteoporosis in the lumbar and femur areas was 38.9% and 36.3%, respectively, but the prevalence of osteoporosis in either area was 51.7%. Note that a significant percentage of the patients in our study were in the transitional period in which they had osteoporotic BMD in one area only. Recently, the Korean government, Korean Ministry of Health, Welfare and Family (MHW), and the Centers for Disease Control and Prevention (CDC) initiated a national survey of the prevalence of osteoporosis; the first report was released in December 2009 based on the results of the survey in 2008 with more than 4000 respondents [14]. The report indicated that the overall prevalence of osteoporosis was 19.3% among people Ōēź 50 years of age and that the prevalence of osteoporosis was as high as 32.6% in postmenopausal women in the general population regardless of risk factors. Our study was directly comparable to this survey in several ways: the diagnosis of osteoporosis was based on the WHO criteria using the standard diagnostic method of BMD measurement, the government survey employed the same device to measure BMD and standard BMD data from young Asian adults was used for the T-score, and the study population was postmenopausal women and men > 50 years old. The higher prevalence of osteoporosis in our study may have occurred because many of our patients were in the transitional stage between osteoporosis in one area to that in both the lumbar and femur, and because the prevalence of osteoporosis among postmenopausal women in the general population exceeds 30% prevalence if the current criteria and standard methods of BMD are applied.
In the present study, the FRAX Japanese model was selected because no epidemiological FRAX data for a Korean cohort exist. The FRAX for the Japanese model was constructed by the Hiroshima cohort and validated by the Miyama cohort [15]. The WHO recommends the application of FRAX based on a country's own epidemiological model, but if one is not available, they recommend use of the most suitable model of the geographically nearest location or racial similarity. By changing the epidemiological data, the relative attribution of each clinical risk factor to the probability of fractures would be maintained, but the absolute risk would change. The absolute risk of fracture, as represented by 10-year probability, is highest in the Swedish and American models, high in the United Kingdom and Italian models, and moderate in the Chinese, Spanish, French, and Japanese models. The lowest output of risk was shown in the Turkish model [16]. Which FRAX country model is the most appropriate to estimate the risk of fracture in the Korean population is not yet known. We used the Japanese model as one of the nearest countries with similar ethnicity.
The HIRA has adopted a simple fixed T-score system to select patients eligible for pharmacological intervention. However, the minimum T-score threshold has been criticized for having a lower score (-3.0) than the standard T-score used by the WHO (-2.5), and for producing unreliable data at the different measurement sites. The difference between the threshold for diagnosis and threshold for treatment was not based on the exact cost-effectiveness data. The present study found no significant difference between guidelines in the number of patients with RA who were eligible for treatment: the HIRA criteria included 55.6% of the patients, and 51.7% of the patients were classified as having osteoporosis using the WHO criteria. This finding may be explained by the use of a minimum T-score in any lumbar or femur site rather than a standard site as specified by the WHO criteria. Furthermore, the current HIRA policy includes patients with prior osteoporotic fractures. Thus, the total number of patients deemed eligible for osteoporosis treatment may not differ between guidelines; the more significant issue is the composition of the target treatment group. In addition to BMD, the risk of fragility fracture increases with age, prior fracture history, use of corticosteroids, and the presence of RA [3]. Thus, while the FRAX estimated risk for patients with RA may not be completely accurate for the Korean population, risk factors other than BMD should be considered when planning preventive intervention for osteoporosis. Our comparison of the FRAX and HIRA criteria in patients with RA has demonstrated that high-risk patients, such as those who are older or use steroids, may be overlooked in the current system based on T-score alone.
Although FRAX has been validated and recommended by the NOF in the United States and other countries as an ideal tool for fracture risk assessment in patients with low bone mass, it has some barriers to application in practice as previously noted [17]. One limitation is its complexity. Several reports suggest that a simplified FRAX or alternative scoring system be used in practice [17,18]. An additional problem is that the size of the treatment group has increased. After modification of the NOF guidelines with FRAX in the United States, the widespread adoption of new guidelines was estimated to result in recommending pharmacological treatment for at least 72% of US white women Ōēź 65 years of age and 93% of those Ōēź 75 years of age, which is a larger inclusion than prior guidelines [19]. To decrease the extra cost of applying new inclusion, some trade-off between low-risk and high-risk treatment groups must exist; however, this may not be acceptable because the critical T-score is still the strongest predictor for fractures.
Alternatively, the economic problem may be alleviated by using the FRAX as an assessment tool to select patients for a BMD examination. Treating high-risk patients without a BMD examination and selecting an intermediate risk group for a BMD examination may be more cost-effective than recommending BMD measurements for all patients [20].
In the present study, we examined the discrepancy originating from the BMD difference between the lumbar and femur areas when FRAX was applied to the previous HIRA treatment group. We identified 15 patients (6%) with high femur neck BMD who were not classified as eligible for treatment despite having a low lumbar area BMD. Without treatment, these patients are at significant risk during the transient period when they show only one area of osteoporosis. The FRAX criteria use femur neck BMD as a reference because it is a reliable marker for osteoporotic fractures in other areas, and it is the strongest predictor for hip fractures [3]. Fusiwara et al. [15] showed the validity of using the femur neck BMD in FRAX to predict major osteoporotic fractures other than femur fractures in the Japanese model.
In the present study, we could not examine the validity of FRAX to predict fracture risk of Korean patients with RA, but we could examine the feasibility of the risk score system compared to the present T-score system for threshold of intervention. We also compared the size of the treatment group identified by each system.
In conclusion, nearly one-half of postmenopausal women and men > 50 years of age with seropositive RA in Korea have osteoporosis requiring treatment. Because the current fixed T-score-dependent classification excludes high-risk patients from pharmacological intervention, the adoption of a risk scoring system should be considered to prevent RA comorbidities. Further studies are needed to validate an osteoporosis risk scoring system for Koreans.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





