


INTRODUCTION
The initial investigation of adverse effects of medical treatment (AEMT) commenced with the Harvard Medical Practice Study (HMPS) in 1984, with findings published in 1991 [1]. This research laid the foundation for the Institute of Medicine to release “To Err is Human: Building a Safer Health System” in 1999 [2]. This study highlighted significant patient safety challenges and prompted further research. Subsequent investigations revealed the substantial burden of AEMT, particularly in the United States, where medication errors are the third leading cause of death [3]. The economic impact of medication errors is considerable, with avoidable adverse drug effects constituting a large portion of this burden [4]. Moreover, healthcare-related patient harm accounts for approximately 10–15% of total healthcare expenditures [5].
To mitigate its economic burden and improve patient safety, the World Health Organization (WHO) initiated three Global Patient Safety Challenges: “Clean Care is Safer Care” and “Safe Surgery Saves Lives” in 2004, followed by “Medication Without Harm” in 2017 [6]. Furthermore, following the HMPS study, the medical record system was revised to identify triggers of adverse events, and the implementation of electronic health records was intended to enhance patient safety [7]. However, the lack of quantitative measures hinder the assessment of patient safety improvements, and insufficient routine documentation of adverse drug events in clinical practice further impedes the efforts to enhance patient safety [7].
AEMT remains a major contributing factor to morbidity and mortality [8]. However, no global studies have yet addressed the impact of AEMT as a worldwide burden, leading to a gap that hinders the ability to evaluate current initiatives and interventions related to AEMT. Such evaluation is critical for the insights for effectively addressing its global burden in future healthcare strategies. Therefore, this study aims to provide comprehensive estimates of the prevalence, incidence, disability-adjusted life years (DALYs), and mortality from 1990 to 2021, stratified by age, sex, geographical locations, Socio-demographic Index (SDI) levels, and Healthcare Access and Quality (HAQ) Index using data from the Global Burden of Disease, Injuries, and Risk Factors Study (GBD) 2021. This manuscript was produced as part of the GBD Collaborator Network and in accordance with the GBD Protocol.
METHODS
GBD 2021 overview
The GBD 2021 provides comprehensive estimates of global risk exposure and health losses due to risks, including AEMT. It is based on relevant indicators from 204 countries and regions, classified into 21 regions and 7 super-regions for the years 1990 to 2021. The GBD 2021 calculated the numbers and rates of prevalence, incidence, mortality, DALYs, years lived with disability (YLDs), and years of life lost (YLLs), with estimates organized according to a cause list [9]. The GBD cause list is hierarchically structured from level 1 to level 6, and for the 2021 study, it has been expanded to 371 causes. Additionally, data is provided by sex and age, covering the lifespan from birth to over 95 years, with the 2021 update further subdividing the under-5 age group into four categories, including a neonatal group. This study adheres to the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) guidelines [10], and further details can be found in Supplementary Appendix 1.
Case definition
Within the GBD 2021 hierarchy, injuries are categorized as a Level 1 condition. AEMT is classified as a Level 3 cause under the Level 1 category of ‘injuries’ and the Level 2 category of ‘unintentional injuries’. All input data were mapped to the GBD causes through ICD mapping, specifically utilizing International Classification of Diseases, Ninth Revision (ICD-9) and International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes. For AEMT, the mapping process was divided into fatal and non-fatal estimates [11], with a detailed classification of ICD-9 and ICD-10 codes for each category. The complete list of ICD codes mapped to AEMT is available in Supplementary Appendix 1, p. 64–123.
Overall, AEMT is defined as death or short-term or longterm disability sustained as the result of undergoing a procedure, treatment, or other exposure to the health-care system. These encompass adverse drug events (e.g., Reye’s syndrome), surgical and perioperative complications (e.g., postsurgical hypoinsulinemia), misadventure (e.g., accidental puncture or laceration of the dura during a procedure), adverse outcome from medical management (e.g., transfusion-related acute lung injury), and complications linked to medical or surgical devices (e.g., nervous system complications from surgically implanted devices) [12].
Fatal outcome estimation
Mortality rates were estimated using the cause of death ensemble model (CODEm), a methodology developed by the GBD study for analyzing cause-specific mortality [9]. CODEm utilizes out-of-sample predictive validity testing of statistical models and covariate permutations (Supplementary Appendix 1, p. 14–15). The mortality rates for AEMT were estimated using 3,653 data sources, including vital registration, verbal autopsies, and mortality surveillance, covering the period from 1990 to 2021. To ensure consistency across cause-specific models, the CoDcorrect algorithm was employed to derive the final burden estimates (Supplementary Appendix 1, p. 15). The generated mortality estimates include YLLs, calculated by multiplying the number of deaths by the standard life expectancy for each age group, stratified by cause, age, sex, location, and year.
Additionally, the mortality-incidence ratios (MIRs) were utilized as an indicator to specifically assess the lethality of AEMT within certain populations [13]. The MIR was calculated as the ratio of the number of deaths due to the AEMT to the total number of incident cases (Supplementary Appendix 1, p. 32–35). The MIRs for AEMT can vary significantly based on several factors, including the medical characteristics of the population, the availability and quality of healthcare services, the effectiveness of follow-up treatments, and advancements in medical technology over time [13]. To capture temporal trends, the analysis focused on the percentage change in MIRs between 1990 and 2021, stratified by age groups and countries categorized by the SDI. This approach allowed for a detailed evaluation of how MIRs evolved over time across different demographic and socioeconomic contexts.
Non-fatal outcome estimation
The non-fatal estimates generated for GBD 2021 are incidence, prevalence, and YLDs. A total of 346 sources were used, including data from hospital and emergency department records, insurance claims, and surveys, to acquire non-fatal estimates. To model healthcare access and treatment across spatial and temporal dimensions, we employed Spatiotemporal Gaussian process regression (ST-GPR) methods. This approach facilitated the estimation of treatment rates while adjusting for biases inherent in healthcare data. Additionally, we applied the meta-regression—Bayesian, regularised, trimmed (MR-BRT) modeling to adjust epidemiological data based on the proportion of individuals with access to healthcare services. This included adjustments for inpatient and outpatient care, specifically focusing on sex-specific hospitalization rates. The integration of these two methodologies allowed for the separate modeling of the AEMT for both inpatient and outpatient populations. Finally, we estimated the prevalence and incidence of AEMT using the DisMod-MR 2.1 tool. Detailed descriptions of the methods employed are provided in Supplementary Appendix 1, p. 17–25 [11].
The prevalence and incidence of AEMT were categorized into short-term and long-term estimates, considering differences in disability weights (DWs) for the calculation of YLDs. The YLDs adjusted for DWs were ultimately aggregated into total YLDs through a comorbidity correction process (Supplementary Appendix 1, p. 26–29). AEMT cases that received treatment were assigned different DWs compared to those that did not receive treatment. The proportion of treated cases was estimated using the HAQ Index. The expected duration of injuries was applied alongside DWs to generate epidemiological estimates. For non-fatal AEMT cases, the long-term excess mortality rate was assumed to be zero [11].
HAQ Index
This study examines healthcare access and quality for AEMT within defined age groups, based on the Organisation for Economic Co-operation and Development definition of the working-age population (15–64 yr) and Nolte and McKee’s avoidable mortality age limit of 74 years [14]. The HAQ Index quantifies healthcare performance on a scale from 0 to 100, where 0 represents the lowest observed performance and 100 the highest. The index standardizes the effects of cause-specific factors and risk exposures through an average weighting system to allow meaningful comparisons across age groups, years, and countries [15]. Using the HAQ Index, this study analyzed the correlations between key AEMT metrics—prevalence, incidence, DALYs, and mortality—and healthcare quality and access. Additionally, locations were stratified into five SDI groups to examine variations in healthcare access and quality. This approach provides a comprehensive perspective on the relationship between national medical quality, accessibility, and AEMT outcomes. Further methodological details are provided in Supplementary Appendix 1, p. 34–36.
Statistical analysis
All estimates derived from the GBD 2021 include a 95% uncertainty interval (UI), which was generated as the 2.5th and 97.5th percentiles. The UI was obtained through random draws of 1,000 samples, thereby reflecting the certainty of each estimate. For every estimate, the draws were aggregated by year, sex, age group, location, and SDI. As a composite measure, a location with an SDI of 0 represents the theoretical minimum level of sociodemographic development relevant to these health outcomes, whereas an SDI of 1 indicates the theoretical maximum level of sociodemographic development pertinent to these health outcomes. The SDI was calculated in accordance with the methodology outlined in the GBD 2021. Detailed methodological information can be found in Supplementary Appendix 1, p. 30–32. To examine the correlation between epidemiological measures and the HAQ, Pearson correlation coefficient analysis and linear regression analysis were conducted. The analyses were performed stratified by quantiles and by country. All analyses were conducted using Python (version 3.12.4; Python Software Foundation, Wilmington, DE, USA) and R (version 4.4.1; R Foundation, Vienna, Austria).
RESULTS
Global burden of AEMT
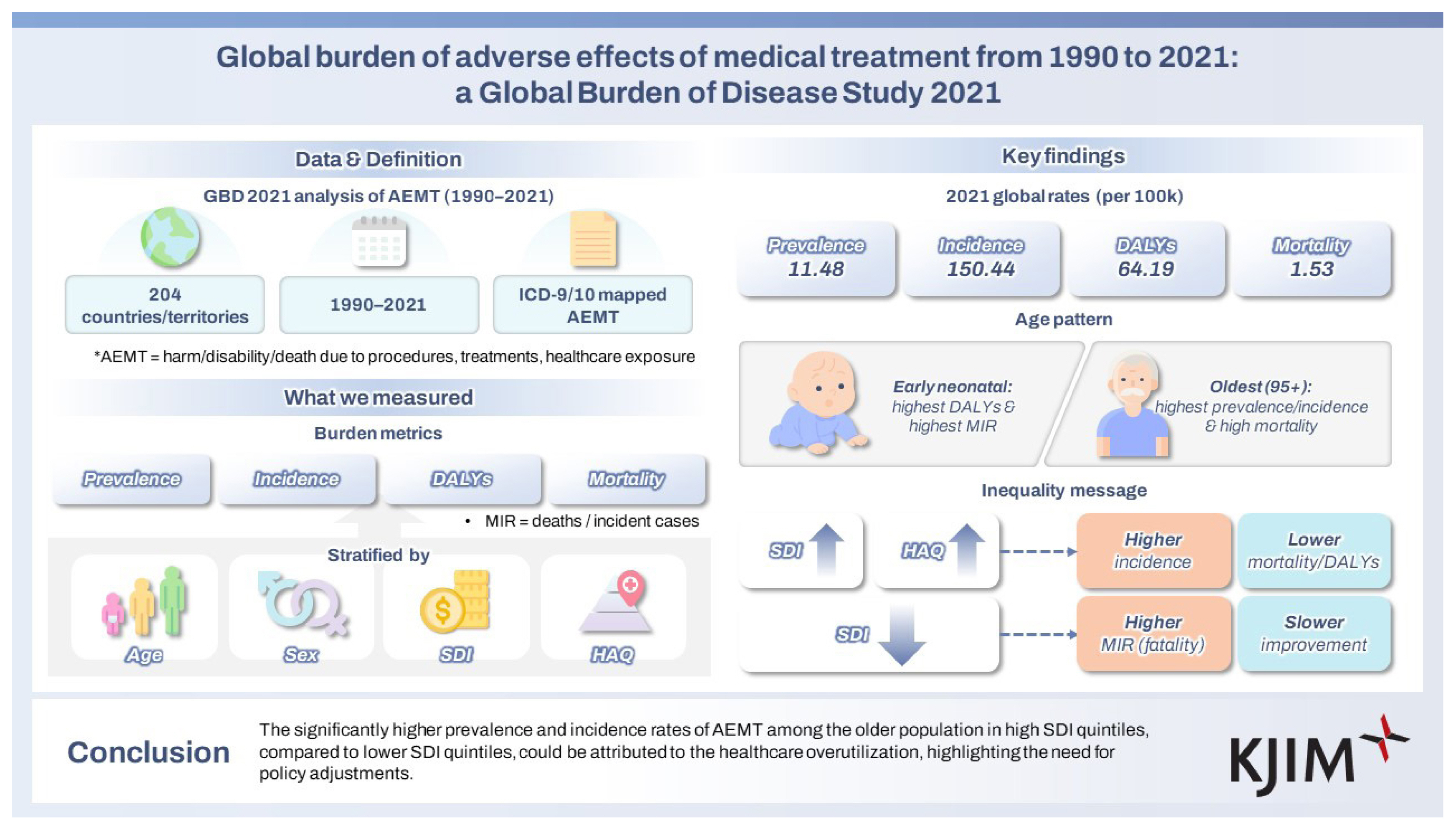
In 2021, the global age-standardized prevalence and incidence rates of AEMT were 11.48 per 100,000 population (95% UI, 8.86 to 14.13) and 150.44 (131.19 to 171.81), respectively. The age-standardized rates for DALYs and mortality were 64.19 per 100,000 population (95% UI, 51.06 to 73.11) and 1.53 (1.29 to 1.68), respectively. The national-level age-standardized rates of prevalence, incidence, DALYs, and mortality in 2021 are illustrated in Figure 1. Detailed counts and age-standardized rates for each measure at the national and regional level are presented in Tables 1. Age-standardized rates of YLDs and YLLs are shown in Supplementary Figure 1 and Supplementary Table 4. The annual percentage changes in age-standardized rates of prevalence, incidence, and YLDs per 100,000 population from 1990 to 2021 are depicted in Supplementary Figure 2 and Supplementary Table 5. The composition of DALYs by YLDs and YLLs over the same period is shown in Supplementary Figure 3 and Supplementary Table 6. Throughout the study period, over 97% of the total DALYs were consistently attributed to YLLs.
From 1990 to 2021, the total numbers of prevalence, incidence, and mortality cases increased. In 1990, the total prevalence was 565.62 thousand (95% UI, 438.03 to 701.01), incidence was 7,407.31 thousand (6,414.51 to 8,635.04), and mortality was 108.54 thousand (94.49 to 127.77). By 2021, these figures had risen to 919.07 thousand (95% UI, 706.95 to 1,139.54) for prevalence, 12,042.79 thousand (10,491.19 to 13,779.53) for incidence, and 123.66 thousand (105.79 to 136.36) for mortality. In contrast, the total number of DALYs showed a decreasing trend, declining from 5,745.00 thousand (95% UI, 4,914.84 to 6,594.17) in 1990 to 4,846.98 thousand (3,914.84 to 5,494.17) in 2021 (Supplementary Fig. 4 and Supplementary Table 7).
Despite these increases in total numbers, the age-standardized rates of prevalence, incidence, DALYs, and mortality all declined from 1990 to 2021. The age-standardized prevalence rate decreased from 12.12 per 100,000 (95% UI, 9.35 to 15.07) in 1990 to 11.48 (8.86 to 14.13) in 2021, peaking at 14.67 (11.32 to 18.22) in 2012. Similarly, the incidence rate declined from 158.83 per 100,000 (95% UI, 138.05 to 183.62) in 1990 to 150.44 (131.19 to 171.81) in 2021, also peaking at 192.39 (168.06 to 220.55) in 2012. Age-standardized DALY rates decreased from 106.49 per 100,000 (95% UI, 91.17 to 122.52) in 1990 to 64.19 (51.06 to 73.11) in 2021. Similarly, age-standardized mortality rates dropped from 2.40 per 100,000 (95% UI, 2.11 to 2.84) to 1.53 (1.29 to 1.68) over the same period (Supplementary Fig. 4 and Supplementary Table 8). Details on the total numbers and age-standardized rates of YLDs and YLLs are provided in Supplementary Figure 5 and Supplementary Table 9.
Burden of AEMT attributable to age and sex
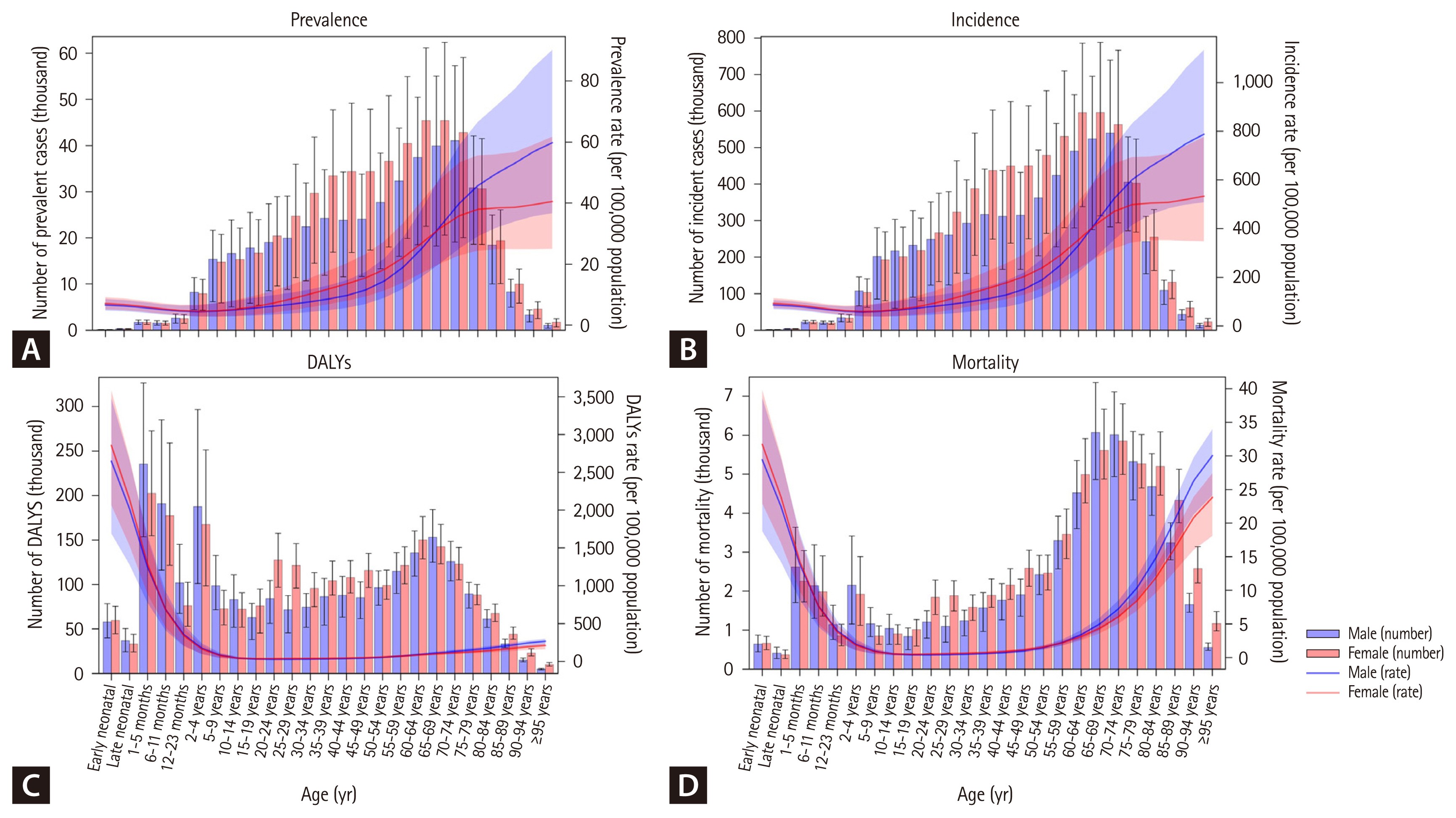
The total counts and rates of prevalence, incidence, DALYs, and mortality, stratified by age and sex, are presented in Figure 2 and Supplementary Tables 10–13. Both prevalence and incidence rates generally increase with age. For prevalence, the lowest rate was observed in the 5–9 age group, at 4.38 per 100,000 population (95% UI, 2.61 to 7.01), while the highest rate was recorded among individuals aged 95 years and older, reaching 50.28 per 100,000 population (28.98 to 79.81). Similarly, for incidence, the lowest rate occurred in the 12–23 month age group, at 52.20 per 100,000 population (95% UI, 36.41 to 69.39), and the highest incidence rate was found among those aged 95 years and older, at 661.86 per 100,000 population (389.39 to 1,012.31).
DALY rates were highest in the early neonatal group, at 4,789.47 per 100,000 population (95% UI, 3,682.00 to 5,963.30). In contrast, mortality rates followed a distinct U-shaped pattern, with higher rates observed in both the neonatal and older population groups. Specifically, mortality rates in the early neonatal group were 53.22 per 100,000 population (95% UI, 40.91 to 66.27), and in the 95+ years group, they were 31.56 per 100,000 population (23.69 to 35.88). The total counts and age-specific rates of YLDs and YLLs are provided in Supplementary Figure 6 and Supplementary Tables 14–15.
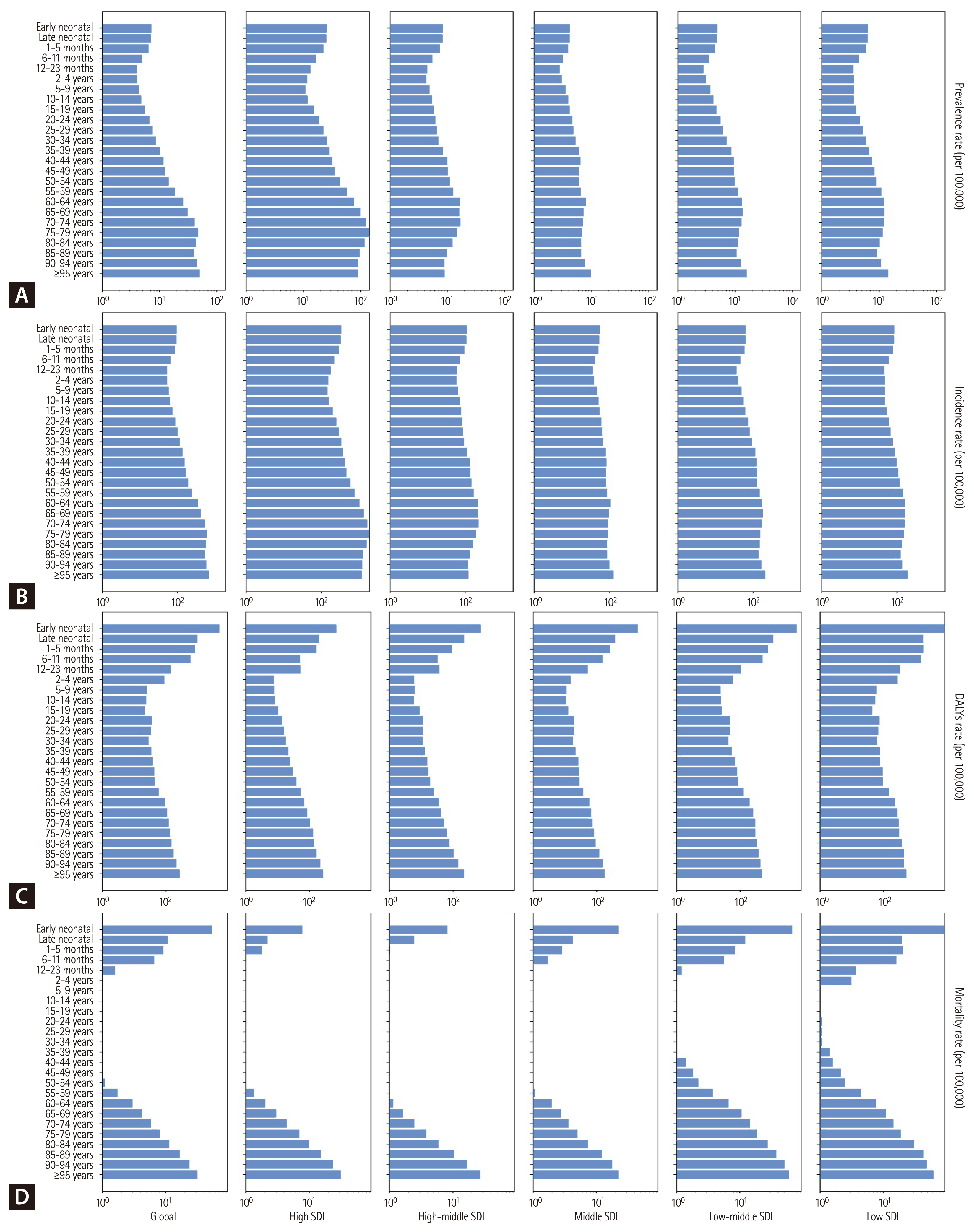
The specific rates of prevalence, incidence, DALYs, and mortality according to each age group, stratified by SDI quintiles are presented in Figure 3 and Supplementary Tables 16–19. Prevalence and incidence rates are highest in all age group in high SDI quintiles compared to lower SDI quintiles. However, DALY and mortality exhibit lower rates in high SDI quintiles in all age group compared to lower SDI quintiles. The specific rates of YLD and YLL according to each age group, stratified by SDI quintiles are presented in Supplementary Figure 7 and Supplementary Tables 20–21.
MIRs of AEMT stratified by age, SDI, and year
In 2021, the MIR was highest at both ends of the age spectrum: the early neonatal group (0.576 [95% UI, 0.551 to 0.580]) and the 95+ age group (0.048 [0.035 to 0.061]). This pattern was consistent across all SDI quintiles, with higher MIRs observed in lower SDI quintiles. For example, in the early neonatal group, the MIR was 0.023 (95% UI, 0.021 to 0.027) in the high SDI quintile, 0.077 (0.071 to 0.082) in the high-middle SDI quintile, 0.402 (0.374 to 0.425) in the middle SDI quintile, 1.062 (1.003 to 1.055) in the low-middle SDI quintile, and 1.123 (0.971 to 1.344) in the low SDI quintile. In the 95+ age group, the MIR followed a similar trend: 0.027 (95% UI, 0.020 to 0.034) in the high SDI quintile, 0.229 (0.189 to 0.250) in the high-middle SDI quintile, 0.174 (0.142 to 0.207) in the middle SDI quintile, 0.286 (0.236 to 0.340) in the low-middle SDI quintile, and 0.328 (0.325 to 0.419) in the low SDI quintile (Figure 4A and Supplementary Table 22).
Globally, the MIR decreased by 33.11% (95% UI, 35.21 to 36.67) from 1990 to 2021 across all age groups. While the highest MIRs persisted in the early neonatal and 95+ age groups across all SDI quintiles, the reductions were smallest in the low and low-middle SDI quintiles. In the early neonatal group, MIR decreased by 11.37% (95% UI, 12.92 to 13.45) in the low-middle SDI quintile and by 12.21% (2.95 to 12.08) in the low SDI quintile, compared to reductions of 40.10% (38.23 to 38.52) in the middle SDI quintile, 72.81% (71.32 to 72.60) in the high-middle SDI quintile, and 41.30% (37.53 to 45.97) in the high SDI quintile. In the 95+ age group, MIR increased slightly in the low-middle SDI quintile (0.64% [95% UI, −15.79 to 1.47]) and in the low SDI quintile (12.22% [−6.45 to 10.11]) (Figure 4B and Supplementary Table 23). The global trend in MIR from 1990 to 2021 is shown in Supplementary Figure 8.
Burden of AEMT correlation with HAQ index
Prevalence and incidence rates are positively correlated with HAQ Index (prevalence rate, r = 0.403, p < 0.0001; incidence rate, r = 0.403, p < 0.0001), while DALY and mortality rates are negatively correlated with HAQ Index (DALY rate, r = −0.657, p < 0.0001; mortality rate, r = −0.585, p < 0.0001) (Fig. 5). Correlation of YLD and YLL rates with HAQ Index are presented in Supplementary Figure 9. Age-stratified analysis revealed that the HAQ Index was most strongly and positively correlated with AEMT incidence rates in the 65–74-year age group, followed by the 15–64 and 0–14 age groups (Supplementary Fig. 10).
DISCUSSION
Key finding
From 1990 to 2021, global AEMT incidence and prevalence rates peaked in the early 2010s before declining, while DALY and mortality rates steadily decreased throughout the period. Both prevalence and incidence rates increased with age, reaching their highest levels in the older population. This trend was most pronounced in the high SDI quintile, which exhibited significantly higher prevalence and incidence rates across all age groups, particularly in the neonatal group. However, only the high SDI quintile indicated notably low MIRs in the neonatal group, while other quintiles experienced the highest MIRs during the early neonatal period. Lower SDI quintiles showed limited reductions in MIRs for the neonatal group from 1990 to 2021 compared to higher SDI quintiles, underscoring persistent disparities in AEMT outcomes by socioeconomic context.
These findings underscore the impact of excessive healthcare utilization in high SDI quintiles, particularly among the older population, and emphasize the need to reduce the burden of AEMT in children under two by improving neonatal care in lower SDI quintiles. Additionally, while prevalence and incidence rates increase with higher SDI levels, the inverse relationship between SDI and overall MIRs, DALYs, and mortality indicates that improved follow-up care for AEMT could substantially reduce mortality and DALYs, as observed in high SDI quintiles.
Plausible underlying mechanism
The elevated burden of AEMT in populations under two years and over 65 years of age can be attributed to several factors. First, older population frequently has multiple prescriptions due to a higher prevalence of comorbidities, and experience physiological changes due to aging [16]. Additionally, they generally experience reduced physical function and subsequent diminished capacity for postoperative recovery. These render old patients susceptible to the adverse effect of drugs and postsurgical complications [17]. In the pediatric population, choosing and dosing of medication require special consideration for pediatric physiology, and the complexity is inherent in pediatric surgical conditions [12]. Kaushal and colleagues also illustrated that perioperative adverse events, along with drug dosage effects, are among the primary causes of high mortality in pediatric populations [18]. Moreover, the use of off-label or unlicensed drugs in neonates and infants is frequent, because of limited studies on pharmacokinetics in neonates, further contributing to the increased DALYs and mortality rates [19].
Several factors may contribute to notably high prevalence and incidence rates of AEMT in older populations within the high SDI quintile. First, high-income countries tend to have a larger proportion of older individuals and a higher prevalence of chronic comorbidities within this age group [20]. Since AEMT occurs more prevalently in conjunction with chronic conditions [21], this could partly explain the elevated rates. Another possible factor is increased healthcare access in high SDI countries [15], which may lead to higher healthcare overuse among the older population, even in cases of non-essential care. For instance, in countries with national health insurance systems, such as South Korea, excessive healthcare use among the older population has become a recognized issue [22]. Moreover, the HAQ Index for individuals aged 65 to 74 years exhibited the strongest positive correlation with AEMT incidence rates, further suggesting that healthcare overutilization among the older population may contribute to the burden in countries with higher HAQ Index values. This finding aligns with previous research indicating a positive association between the proportion of older populations and public healthcare expenditure in high-income countries, as well as the widespread overuse of medical services observed in these settings [23].
Clinical and policy implications
The notably high prevalence and incidence rates of AEMT in older populations within high SDI quintiles are concerning. While it is expected for older individuals with healthcare needs to utilize services, in high-income countries, healthcare utilization by those without critical need may contribute to elevated rates of AEMT and place strain on healthcare systems. Studies indicate that one-fifth to one-third of patients receive unnecessary healthcare services, which may be potentially harmful [24]. Baicker and colleagues suggest that reducing overall testing by 46.8 percent, including a 62.4 percent reduction for low-risk patients, who comprise the majority, and a 15.6 percent increase in testing for high-risk groups would help alleviate the burden of adverse events [25]. Patients often seek additional healthcare services when their personal financial contribution is minimal [25]. However, this issue is not solely patient-driven; clinician incentives also play a role. Clinicians may underutilize high-value resources when compensation is insufficient and overutilize low-value resources when financial returns are higher [26]. Addressing this imbalance requires fostering clinician ethics and establishing a more equitable compensation structure. At a societal level, increasing the proportion of primary care physicians may help curb healthcare overuse [27]. Furthermore, implementing a standardized index to monitor unnecessary healthcare usage and adopting community-based case management for medical aid beneficiaries could reduce the strain of excessive healthcare utilization [28].
The global decline in MIR across all SDI quintiles indicates that the burden of AEMT can be effectively mitigated with the implementation of appropriate interventions. In this regard, it is notable that there was the greatest reduction in MIR in neonatal groups, while MIR among older populations has remained steady. This finding indicates that the observed decline in age-standardized DALY and mortality rates could be primarily attributable to improved survival rate of AEMT in neonatal groups. Additionally, MIR in neonatal groups is the highest across all SDI quintiles, except for the high SDI quintile, further emphasizing the need to reduce the burden of AEMT in neonatal populations across lower SDI quintiles. Previous study reporting many adverse events in neonatal group results in permanent harm and most of them preventable [29]. Also, the higher rates of AEMT in preterm birth, but relative lack of resources and lower quality of neonatal cares in low-income countries compared to high-income countries, emphasize the need to develop interventions of neonatal cares particularly in low-income countries [30]. Achieving outcomes similar to those seen in high SDI regions could be a key target for global policy initiatives aimed at addressing the burden of AEMT worldwide.
Despite previous safety initiatives and interventions so far, the limited impact on patient safety can be attributed to the failure to address multiple contributory factors within the healthcare system [31]. A comprehensive approach combining individual, system, and organizational-level measures is necessary [5]. At the individual level, practitioner education serves as an effective intervention [5]. System-level measures include prospective reporting, which can identify preventable adverse events, provide practical warning systems, and improve the reliability of judgements on the medical errors [32]. Additionally, implementing a dependable system for screening polypharmacy and comorbidities would further strengthen system-level interventions [33]. At the organizational level, fostering a safety culture within healthcare institutions can improve clinicians’ behaviors towards patient safety, thus reducing adverse events and mortality [34]. Furthermore, differences in healthcare systems among high-income countries may also influence the burden of AEMT. For example, variations in insurance coverage, reimbursement structures, and care delivery models could shape patterns of healthcare utilization and adverse outcomes [35]. Future comparative analyses across advanced health systems would provide valuable insights into how institutional contexts modify the risk of AEMT.
Strengths and limitation
Despite the advantages of utilizing GBD 2021 for measuring AEMT, several limitations persist. Firstly, in countries/territories with underdeveloped medical registries, AEMT cases may be underreported due to poor identification processes [36], and estimates of the national and regional burden might rely on modelling data based on neighboring countries or a limited number of organizations, potentially reducing accuracy [37]. Second, unlike prior study conducted in the United States, this analysis did not investigate each AEMT subtype separately (adverse drug events, surgical and perioperative AEs, misadventure, AEs associated with medical management, AEs associated with medical or surgical devices, others) [12]. As noted in the first limitation, compared to the United States, medical registries in non-high-income countries and territories are less developed. Consequently, the classification of AEMT subtypes may lack precision. Therefore, focusing on the overall AEMT estimate offers a more stable and reliable measure in a global context. This approach acknowledges the trade-off between achieving broad global coverage and conducting in-depth component analysis. Third, ICD codes for AEMT in the GBD 2021 may have not fully captured all AEMT cases. Healthcare providers could be reluctant to report AEMTs, as they are often perceived as ‘mistake’. This perception may drive providers to report alternative ICD codes that align more closely with the patient’s symptoms rather than the AEMT itself [38]. Moreover, certain events resulting from inpatient care issues such as nosocomial infections (ICD-10 code, Y95), falls due to inadequate hospital safeguards (W09), or decubitus ulcer and pressure area (L89) may not be classified as AEMTs in the GBD [39]. Lastly, the burden of AEMT could not be subdivided into different severities and its preventability, unlike previous study by Panagioti and colleagues [5]. Despite its limitations, this study offers unique strength. The GBD 2021 utilized a diverse range of data sources, including health registration systems, national censuses, household surveys, disease-specific registries, and published studies, providing a robust dataset for analyzing AEMT. This contrasts with many previous studies, which were often limited to data from single developed countries [12]. As a result, this study stands out as the most current and comprehensive quantitative longitudinal analysis of the global, regional, and national burden of AEMT, stratified by age, sex, and SDI.
CONCLUSION
This GBD 2021 provides a comprehensive overview of the global burden of AEMT from 1990 to 2021. The findings reveal higher prevalence and incidence rates among the older population in high SDI quintiles, likely reflecting healthcare overuse. Elevated MIRs in children under two in lower SDI quintiles, along with slower declines, compared to high SDI quintiles, underscore the need for targeted interventions. Enhancing neonatal care in lower SDI regions and ensuring consistent follow up care are essential to reducing preventable harm and global disparities in AEMT outcomes.
KEY MESSAGE
1. The higher burden of AEMT among older adults in high SDI quintiles may reflect healthcare overuse.
2. MIRs were higher in lower SDI quintiles, indicating a greater risk of fatal outcomes.
3. From 1990 to 2021, MIRs declined more gradually in lower SDI, suggesting persistent disparities in healthcare quality and access.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement figure 1
Supplement figure 1 Print
Print





